
Outcomes after arthroscopic repair of rotator cuff tears in the setting of mild to moderate glenohumeral osteoarthritis
2022-08-13 03:55:11IanHongAllisonRaoTylerCarlLeeJoshuaMeadeDanielHurwitGregoryScarolaDavidTrofaShadleySchiffernNadyHamidPatrickConnorJamesFleischliBryanMichaelSaltzman
World Journal of Orthopedics 2022年7期
INTRODUCTION
Rotator cuff pathology is a common source of shoulder pain.A significant proportion of individuals have rotator cuff tears with increasing age and can become disabled[1-3].In older patients,onset of new symptoms correlate to the progression of rotator cuff tear size and increasing morbidity[3].
Some handsome pillars still stood amongst the heaps of ruins, and several rooms, which yet remained in fair preservation63, gave evidence of former splendour
Like rotator cuff pathology,glenohumeral osteoarthritis (GHOA) is related to advancing age and is estimated to affect 16%-20% of adults over age 65[4,5].It can be debilitating and a source of shoulder dysfunction,pain,and loss of motion[6,7].
Although rotator cuff pathology and GHOA are two prevalent shoulder pathologies,there are limited studies evaluating the relationship of GHOA to outcomes after rotator cuff repair (RCR)[8-11].Cases of severe GHOA accompanied by rotator cuff pathology are most appropriately managed with either reverse total shoulder arthroplasty (RTSA) or total SA (TSA) with RCR.However,a recent study by Jeong[8] suggests that patients with mild GHOA and repair of large rotator cuff tears fare similarly to their counterparts without GHOA in terms of clinical outcomes and progression to GHOA.In contrast,another study found that GHOA was associated with lower outcome scores after RCR at 1-year follow-up[10].
Studies have shown that patients with concomitant GHOA and rotator cuff tears can range from 13%-27% of patients treated for rotator cuff tears;to our knowledge,the outcomes of these patients after RCR are lacking within literature[12,13].This study evaluated the effect of the presence or absence of GHOA on short and mid-term clinical outcomes after arthroscopic repair of small to large rotator cuff tears,comparing the rates of conversion to shoulder arthroplasty (TSA or RTSA) as well as PROM’s at followup > 2 years from their RCR surgery.We hypothesized there would be no significant differences in clinical outcomes or rates of subsequent conversion to shoulder arthroplasty in patients with small to large rotator cuff tears undergoing arthroscopic repair with or without concurrent GHOA.
MATERIALS AND METHODS
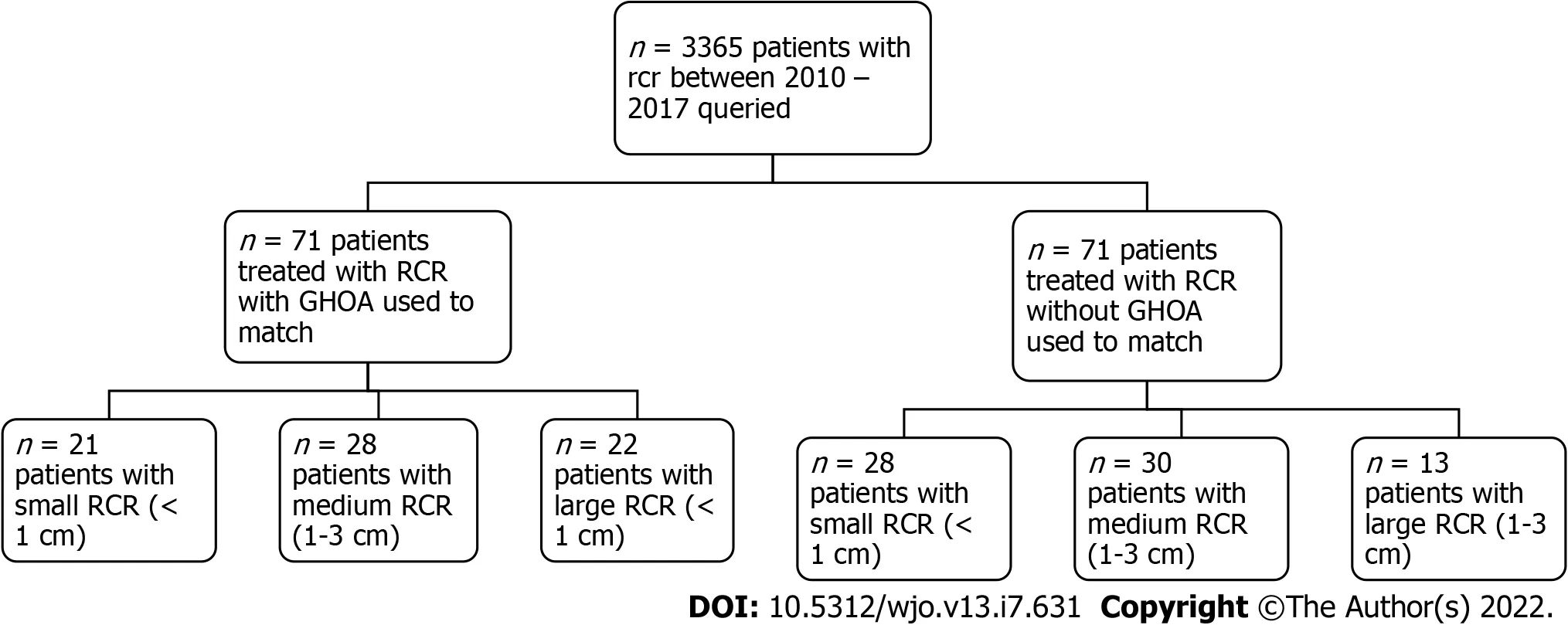
Following International Review Board approval,patients who underwent arthroscopic RCR of small (<1 cm),medium (1-3 cm),or large (3-5 cm) rotator cuff tears with GHOA were identified at a large singlecenter academic orthopedic group.All patients treated between January 2010 and June 2017 were identified using Current Procedural Terminology code 29827 for “arthroscopy,shoulder,surgical,with rotator cuff repair.” Patients with GHOA were initially identified and paired with patients without GHOA.The three criteria for matching the patients involved: Age ± 3 years,clinical follow-up ± 1 year,and same sex (Figure 1A).
Inclusion criteria consisted of patients who: (1) Were 18 years old at the time of index surgery;(2) Had a rotator cuff tear measuring 0-5 cm;(3) Had a preoperative plain radiograph;(4) Had a preoperative magnetic resonance imaging (MRI);and (5) Had a minimum of 2 year follow-up after their index RCR procedure.Patients were excluded if they had any of the following: (1) Open physes;(2) Post-traumatic osteoarthritis;(3) Post-dislocation glenohumeral arthropathy;(4) Avascular necrosis;(5) Prior surgical intervention on the ipsilateral shoulder;and/or (6) Autoimmune conditions such as rheumatoid arthritis.The data was collected and stored using REDCap electronic data capture tools hosted at OrthoCarolina Research Institute[4].
Due to the retrospective design,there are aspects to patient selection and classification that may introduce confounding biases.The heterogeneous nature of the patients with regard to demographics,surgical technique,and being treated by multiple surgeons at a single academic institution may limit the ability to make accurate comparisons between groups.Furthermore,no preoperative PROs were obtained which may have served as a baseline measure to observe any improvements or exacerbations following RCR.Our follow-up period may be reflective of short- term outcomes with a lack of findings for longer-term outcomes (greater than 5 years or 10 years).However,a recent study by Manderle[24] showed that the vast majority of RCR patients achieve MCID,substantial clinical benefit and patient acceptable symptomatic state for various PROs within 1 year.Therefore,our minimum 2-year follow-up period may be sufficient to evaluate and make comparisons of the postoperative PROs following RCR in this patient population.
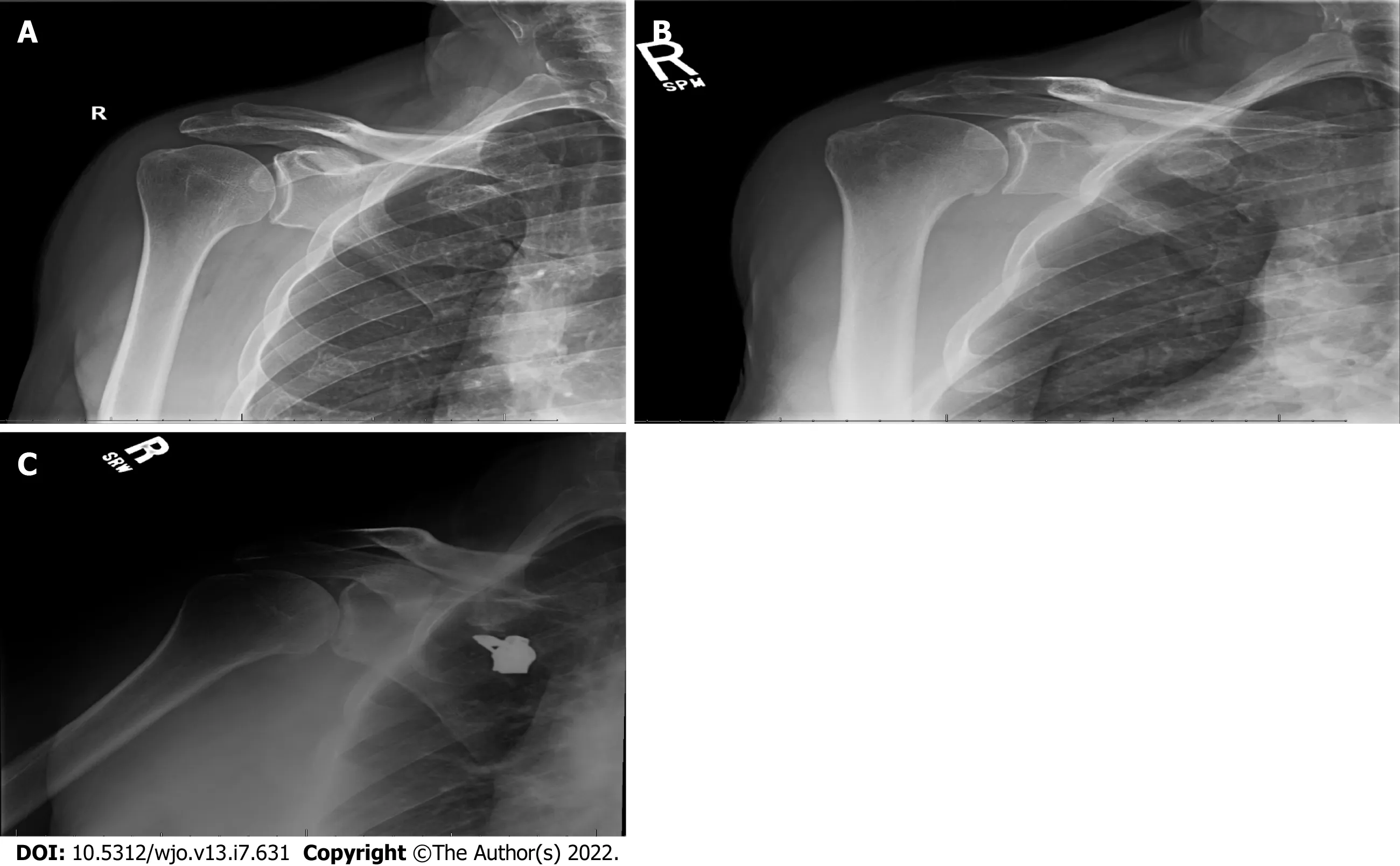
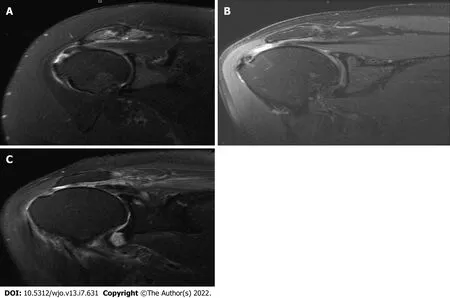
Demographical information such as age,sex,body mass index (BMI),smoking history,diabetes,and injury mechanism (ultra-lowlowhigh energy) where applicable was obtained.Using preoperative plain radiographs and MRI,the Samilson-Priesto Classification (Figure 2),Goutallier classification,and Warner atrophy grade were obtained to assess GHOA severity,fatty degeneration of rotator cuff muscles,and muscle atrophy,respectively.Each patient was classified based on the presence of GHOA in the setting of a small,medium,or large rotator cuff tear (Figure 3).The different rotator cuff tear sizes,largely based on level of retraction,were determined by two independent fellowship trained sports medicine and shoulder orthopedic surgeons using MRI imaging.Coronal oblique images were obtained and used to identify the tears,and were classified as either small (<1 cm) medium (1-3 cm) and massive (<5 cm).
The procedural variables captured using operative notes included: surgical technique,fixation technique,and concomitant procedures (distal clavicle excision,subacromial decompression,capsular release,debridement,chondroplasty,biceps tenotomy,and/or biceps tenodesis).Postoperative variables were measured: complications,re-operation (s) and the type of secondary procedure.PROs following surgery were collected during routine clinical follow-up at 2 or more years.Patients without the standard of care 2-year follow-up were contactedphone or email to answer questions regarding PROs,subsequent rotator cuff re-tear,or re-operation outside of our institution.
The nearer she approached the more miserable44 it appeared, and at length she saw a little old woman sitting upon the door-step, who said grimly: Here comes one of these fine beggars who are too idle to do anything but run about the country! Alas! madam, said Celandine, with tears in her pretty eyes, a sad fate forces me to ask you for shelter
And what was inside after all? Why, nothing but a serpent s skin, which her husband, who was, unknown to her, a magician, put on when he was at work; and at the sight of it the girl was turning away in disgust, when the earth shook violently under her feet, the palace vanished as if it had never been, and the bride found herself in the middle of a field, not knowing where she was or whither to go
Statistical analysis
All data underwent descriptive statistical analysis using SAS version 9.4 (SAS Institute,Cary,NC;http://www.sas.com/software/sas9).Two groups were defined based on presence or absence of primary GHOA and stratified based on rotator cuff tear size.For normally distributed continuous data,mean and standard deviation,were reported.For non-parametric continuous data,median and interquartile range were reported.Frequencies and proportions were reported for categorical variables.A Wilcoxon rank sum test was used for non-parametric continuous variables and a two-sample t test was used for normally distributed data.For categorical variables,a chi-square test (or Fisher’s exact test,where appropriate) was used for comparisons between groups.Significance was determined by an alpha level of 0.05.
RESULTS
Between January 2010 and June 2017,71 patients were identified that underwent arthroscopic RCR of small to large tears with the presence of GHOA.These patients were subsequently matched with 71 patients without GHOA that underwent the same procedure.
To determine patient report outcomes and rate of conversion to arthroplasty for patients with GHOA after undergoing a rotator cuff repair procedure.With favorable outcomes,and low conversion rates to arthroplasty,these objectives were realized in our data set.
The demographics of the comparison study groups can be found in Table 1.The median age at time of rotator cuff repair was 64 years (IQR 60,70) for patients in both groups.They had an exact match by sex and 57.7% (41/71) of repairs were performed in males in each respective group.Median BMI at the time of repair was 29.8 (IQR 26.7,33.2) and 28.5 (IQR 25.5,31) respectively.In patients with GHOA,57.7% (41/71) reported having never smoked tobacco products,40.8% (29/71) have smoked previously and 1.4% (1/71) were actively smoking.In patients without GHOA,60.6% (43/71) reported having never smoked tobacco products,33.8% (24/71) have smoked previously and 5.6% (4/71) were actively smoking.
The Emperor told him he had more than he knew what to do with, and that a new one had been captured that very night for trying to steal his magic bird, but that as he had already more than enough to feed and support, he was going to have this last captive hanged next morning
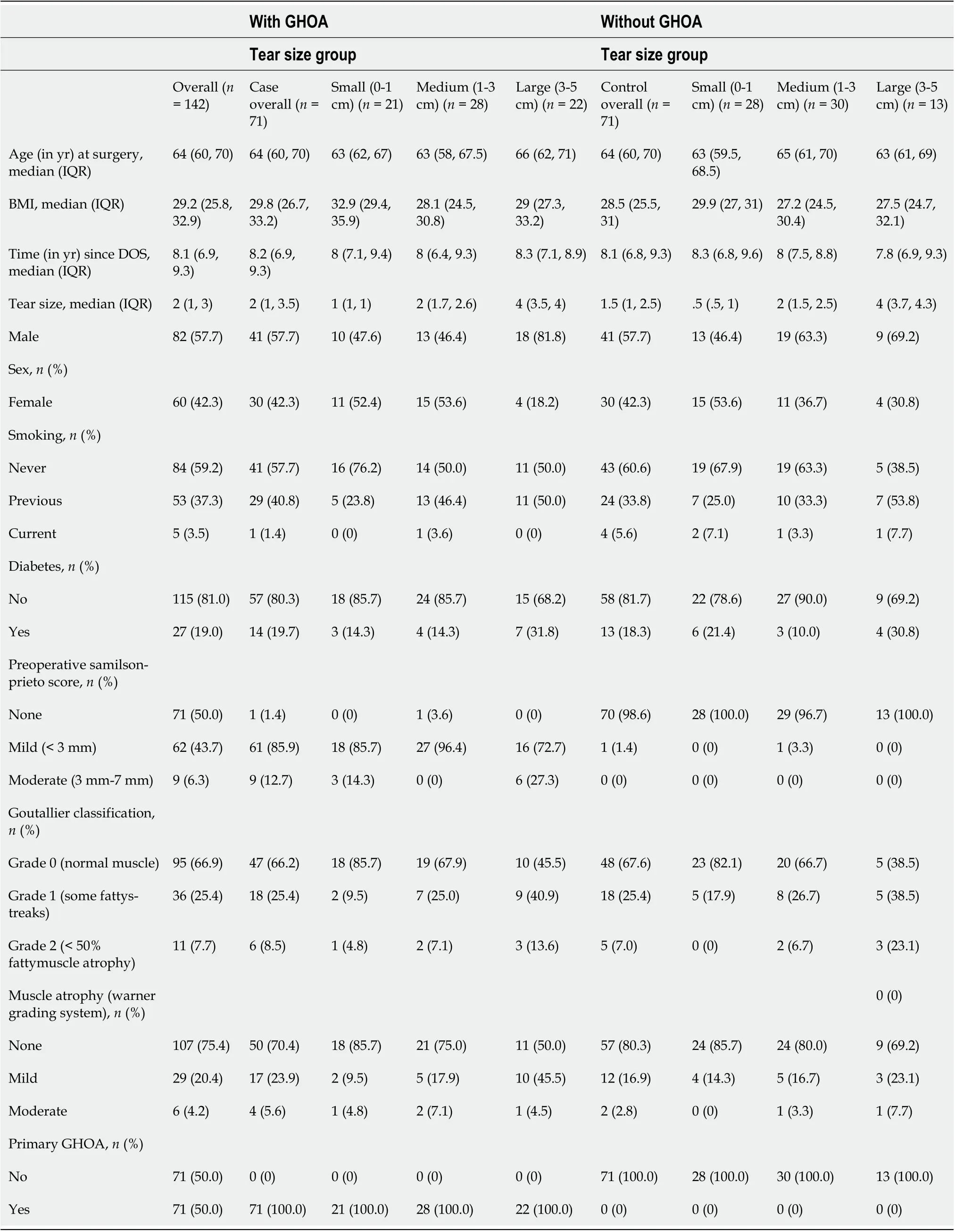
Using the Samilson-Prieto classification to grade GHOA severity,85.9% (61/71) had a grade of 1 (mild or <3 mm),and 12.7% (9/71) had a grade of 2 (moderate or 3 mm - 7 mm).Goutallier classification of the rotator cuff revealed that patients with GHOA: 66.2% (47/71) had a grade of 0 (normal muscle),25.4% (18/71) had a grade of 1 (some fatty streaks),and 8.5% (6/71) had a grade of 2 (less than 50% fatty muscle atrophy).In comparison,the Goutallier classification of the rotator cuff for patients without GHOA revealed: 67.6% (48/71) with grade of 0,25.4% (18/71) with a grade of 1,and 7.0% (5/71) with a grade of 2.Finally,in patients with GHOA the Warner grading system for muscle atrophy revealed: 70.4% (50/71) with no atrophy,23.9% (17/71) with mild atrophy,and 5.6% (4/71) with moderate atrophy.For patients without GHOA,the Warner grading system for muscle atrophy revealed: 80.3% (57/71) with no atrophy,16.9% (12/71) with mild atrophy,and 2.8% (2/71) with moderate atrophy.
“I know nothing about it,” said the emperor. “Music! music!” he cried; “the large Chinese drum! that I may not hear what they say.” But they still went on, and Death nodded like a Chinaman to all they said. “Music! music!” shouted the emperor. “You little precious golden bird, sing, pray sing! I have given you gold and costly presents; I have even hung my golden slipper round your neck. Sing! sing!” But the bird remained silent. There was no one to wind it up, and therefore it could not sing a note.
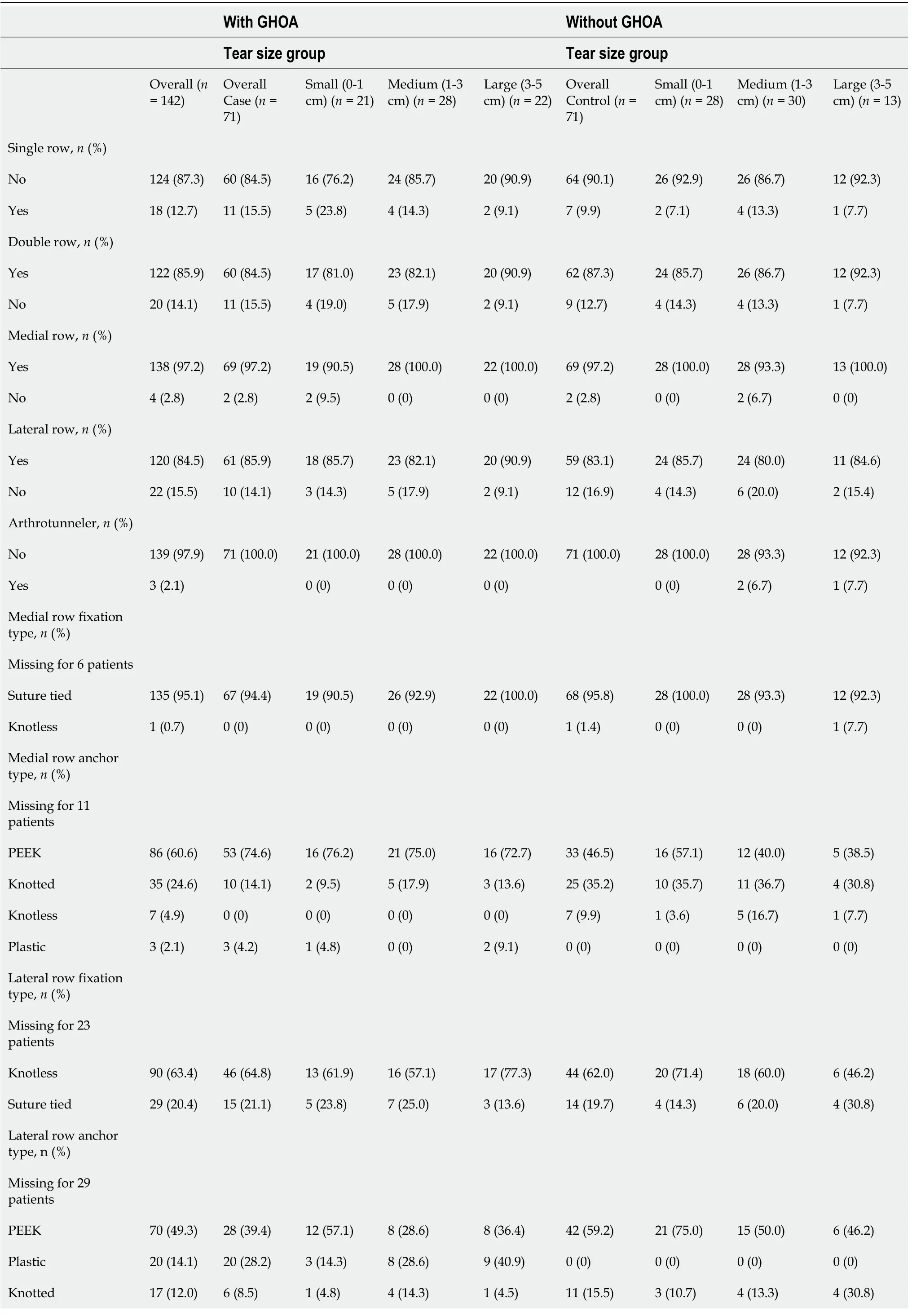
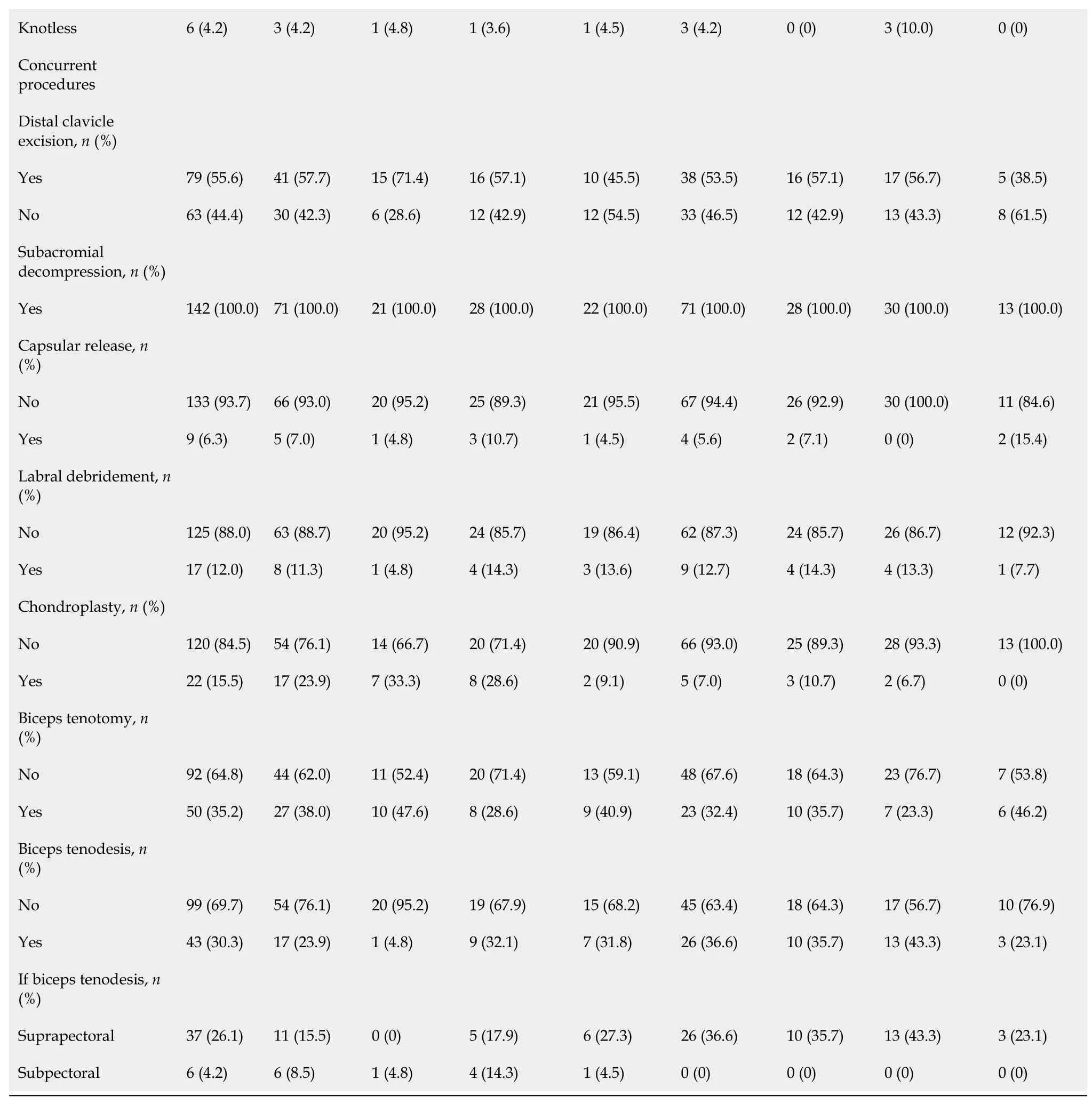
Detailed data regarding RCR surgical technique,type of anchors used,fixation method and concurrent procedures for patients with or without GHOA stratified by rotator cuff tear size can be found in Table 2.
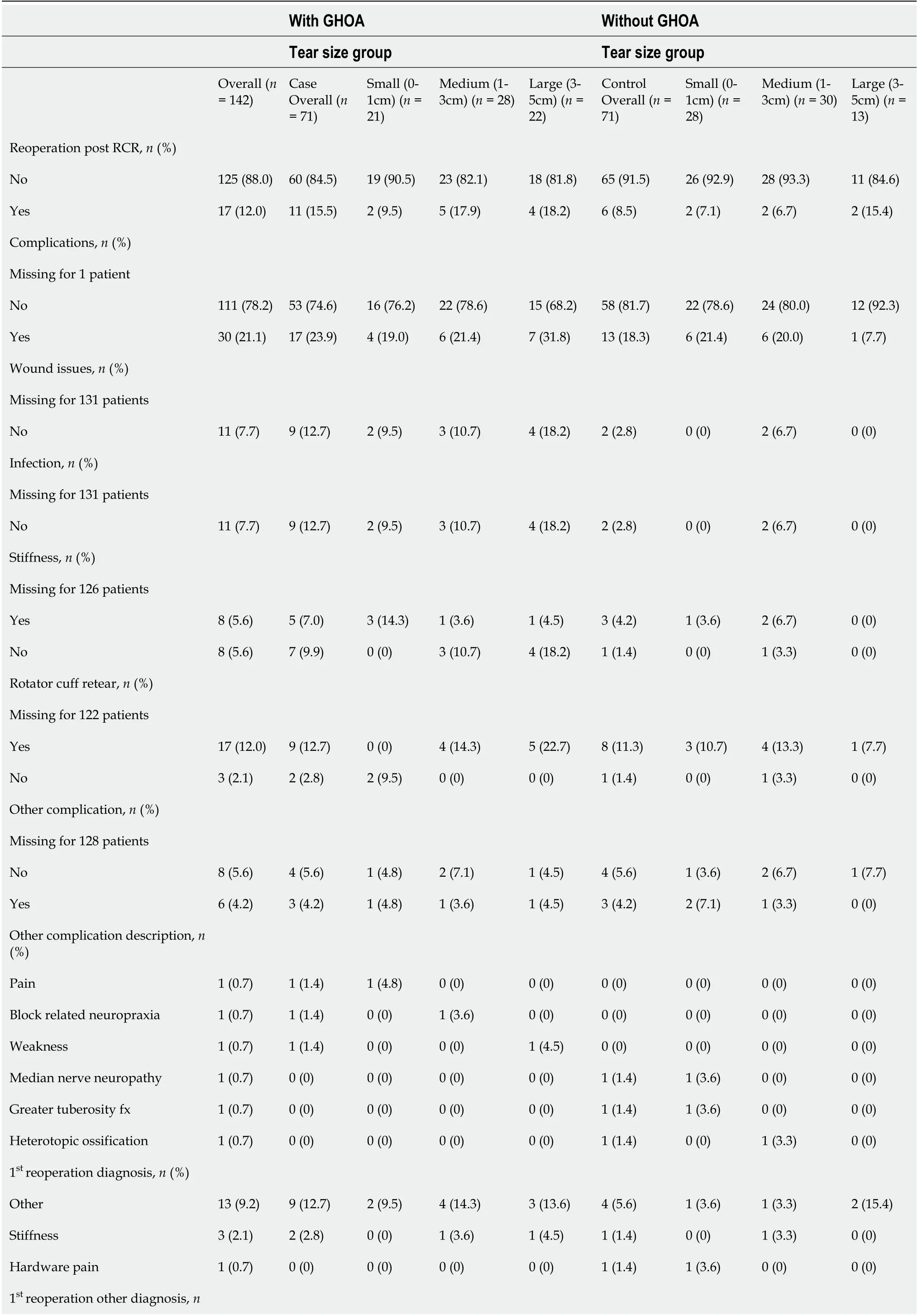
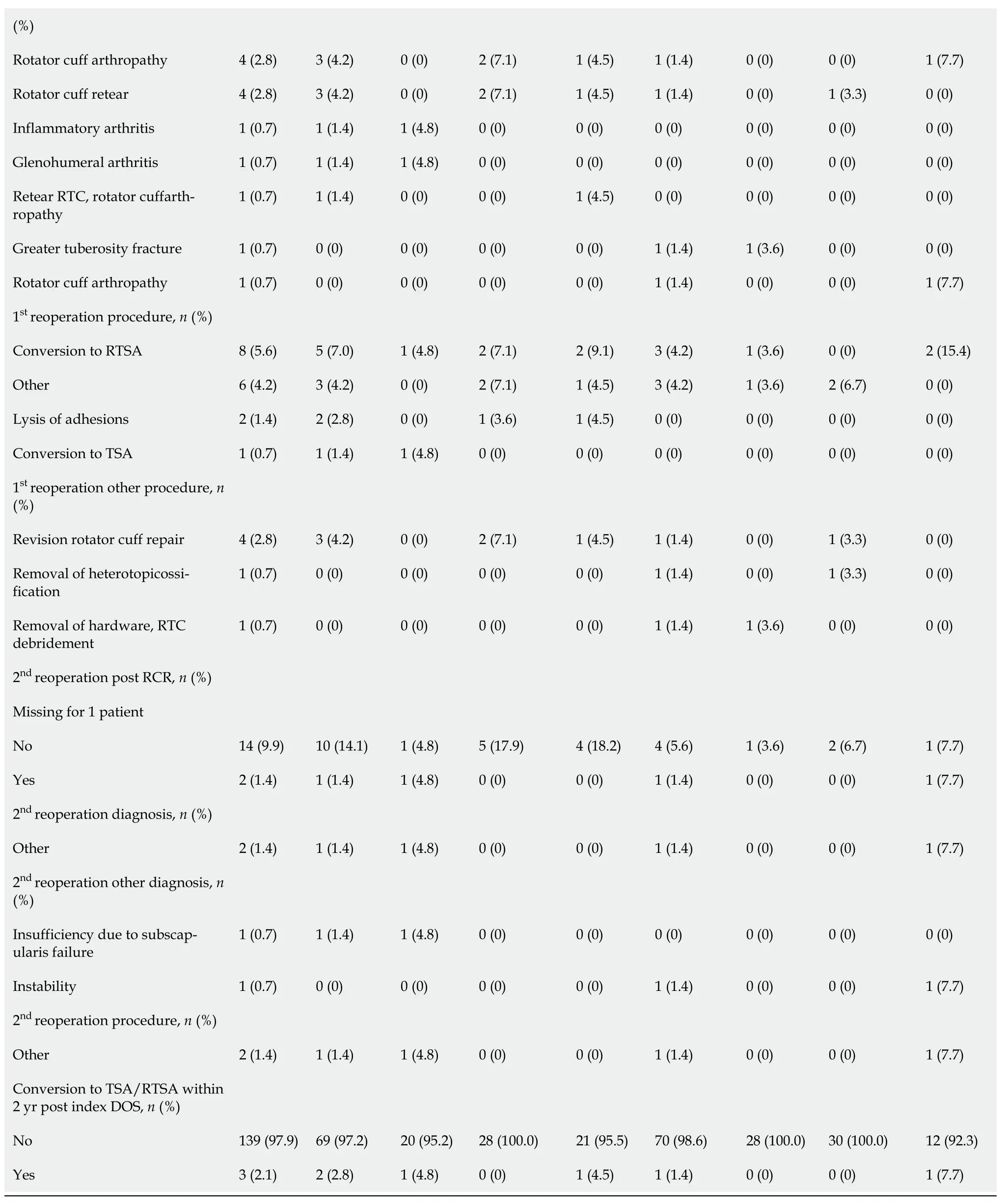
The re-operation rate was 15.5% (11/71) and 8.5% (6/71) in patients with GHOA and without GHOA respectively.The mean follow-up period for both groups was 12.45 mo,with a range from 0-104 mo for the GHOA group,and 0-94 mo for the patients without GHOA.Within two years after rotator cuff repair,2.8% (2/71) patients with GHOA underwent TSA or RTSA in the ipsilateral shoulder compared to 1.4% (1/71) patients without GHOA.Both patients developed rotator cuff arthropathy and pain with range of motion,and eventually underwent RTSA.The non GHOA patient eventually underwent an RTSA for rotator cuff arthropathy.Beyond the two year follow-up 4 patients with GHOA and 2 patients without GHOA underwent the conversion to TSA or RTSA.Complication rates after initial rotator cuff repair was 23.9% (17/71) and 18.3% (13/71) for patients with GHOA and without GHOA respectively and 12.7% (9/71) of patients with GHOA experienced rotator cuff re-tear after RCR compared to 11.3% (8/71) of patients without GHOA as determined by post op MRI or intra-operative findings (Table 3).
So that evening, when the Princess came once more with her sleeping-drink, he pretended to drink, but threw it away behind him, for he suspected that it was a sleeping-drink
But, sitting lonely, time soon began to hang heavy on her hands. One day she said to the old woman: It is dull for me, grandmother, to sit idly hour by hour. My hands want work to do. Go, therefore, and buy me some flax, the best and finest to be found anywhere, and at least I can spin.
DISCUSSION
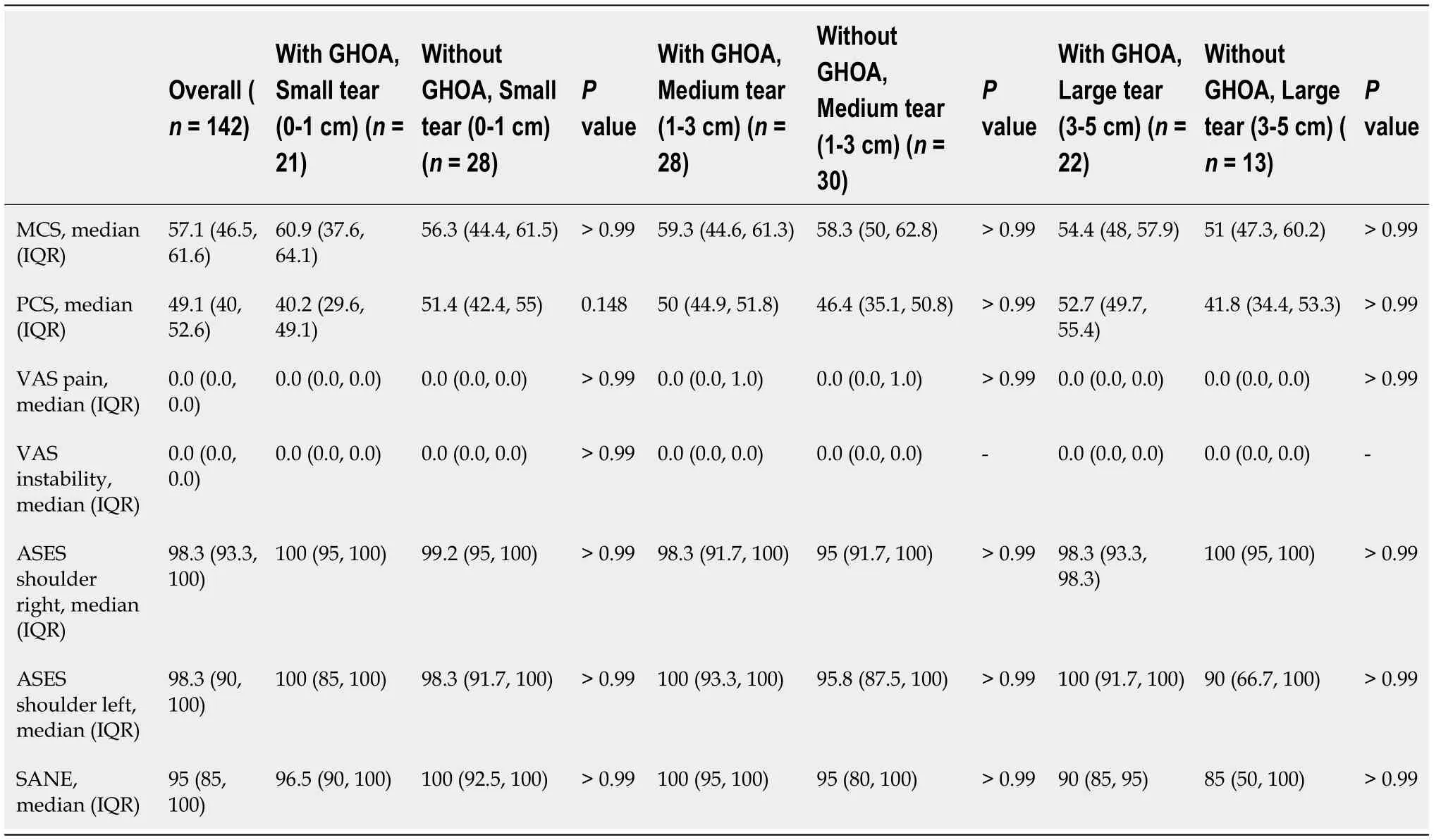
Overall,the results of our PROs after a short to medium term follow-up period show favorable results in VR-12,VAS,ASES,and SANE regardless of tear size or presence of GHOA.In patients with mild to moderate GHOA,there were no significant differences in all categories of PROs when comparing to patients without GHOA stratified by small to large rotator cuff tears.The minimal clinical important difference (MCID) was established to define minimum difference in PROs that is required to provide a clinically relevant benefit for patients rather than relying on statistically significant differences.The MCID for VR-12 PCS,MCS,VAS pain,ASES,and SANE following RCR has been reported to be 4.94,5.99,1.4,21.0,and 11.80 respectively[18,19].VR-12 PCS was the only PROs that showed MCID when patients with small or large rotator cuff tears were compared by presence or absence of GHOA.Surprisingly,patients with mild to moderate GHOA and small RCR had worse VR-12 PCS scores.A literature review of histopathology of rotator cuff tears showed that inflammatory cell infiltrate and number of blood vessels are inversely correlated with tear size[20].Immunochemistry has also shown torn rotator cuff tendons with lower vascularity have fewer new nerve fibers and is linked to lower chronic pain[21].
The first thing people asked was what about the Blue Jay. Had he stayed blue? Yes, he was still the same color. No longer were there two colors in the world, but just one -- the color blue. And because the Blue Jay was a color like everybody and everything else people began to lose interest. Now that he was neither more nor less important crowds stopped coming and one day, six months into the year that the world had turned blue, somebody let him out of his cage and he flew off looking happy to be free.
A recent study by Jeong[8] retrospectively evaluated the clinical outcomes of large to massive RCR in patients with and without mild GHOA.The authors found that preoperative and postoperative variables (VAS scores,ROM,muscle strength,University of California,Los Angeles (UCLA) scores,and Constant scores) at final follow-up (2 years) showed no significant differences between the two groups.Our study also included VAS and similarly did not show any significant difference between groups at final follow up period of 2 years.Jeong[8] reported mean VAS scores in patients with large to massive tears with mild GHOA and without mild GHOA to be 0.3 ± 0.7 and 0.3 ± 0.8,respectively which are similar to our overall median VAS score of 0.0 (IQR 0.0,0.0).These combined results indicate that patients with small to large rotator cuff repairs in the setting of mild to moderate GHOA can expect to have a pain score close to 0 after a minimum of 2 years after RCR.
A study by Kukkonen[10] evaluated outcomes using Constant scores in patients with or without GHOA after undergoing supraspinatus tendon repair with tear sizes ranging from 0.5 cm to 2.5 cm.Both pre and post-operative Constant scores were significantly lower in patients with GHOA.These results differ from ours and Jeong’s which showed no difference in PROs in patients with or without GHOA[8].Kukkonen’s study only included males,had final follow-up of 1 year,and used the Kellgren-Lawrence classification to determine GHOA severity and status[10].In contrast,our study and the study by Jeong[8] included males and females with a follow-up of 2 years and used the Samilson-Priesto classification for GHOA grading.A study of radiographic classifications of GHOA found that the Kellgren-Lawrence provided inferior inter-observer agreement in diagnosis of GHOA compared to Samilson-Priesto due to the challenge of identifying minor joint space narrowing in the non-weight bearing shoulder joint[17].The aforementioned finding may limit comparative value of studies using different radiographic classification methods.
The results demonstrate the conversion to shoulder arthroplasty,patient-reported clinical outcome scores,and rates of re-operation were no different when comparing RCR done in the setting of GHOAwithout GHOA in short-term follow-up.Our results indicate that the presence of GHOA at the time of RCR did not seem to influence the progression of GHOA.There is general agreement within literature that severe primary GHOA is an appropriate indication for TSA or RTSA[14,15].Additionally,rotator cuff tear arthropathy,rotator cuff insufficiency,and superior migration of humeral head - is considered another indication for RTSA[14-16].While GHOA and rotator cuff tears both contribute to morbidity due to decreased shoulder function,there are limited studies evaluating the outcomes of joint-preserving treatmentRCR in the setting of GHOA.
The rate of conversion to TSA or RTSA within 2 years after RCR were low for patients with and without GHOA at 2.8% (2/71) and 1.4% (1/71),respectively.This is the first study to report conversion to TSA or RTSA as an outcome variable while comparing outcomes following RCR in patients with or without GHOA.Results of previous studies,which showed that the progression of GHOA did not negatively affect PROs at final follow-up in patients who underwent RCR or arthroscopic debridement of massive irreparable rotator cuff tears[8,22,23],led us to hypothesize patients with GHOA would have conversion rate to TSA or RTSA are comparable with patients without GHOA.The results of our study report good PROs and very low conversion rates to shoulder arthroplasty after RCR with concomitant GHOA.
The primary outcome variable was the rate of conversion to TSA or RTSA within 2 years from the index surgery.Secondary outcomes were clinical patient-reported outcome measures (PROs) including American Shoulder and Elbow Surgeons (ASES) score,Single Assessment Numeric Evaluation (SANE),VAS for pain,and Veterans RAND 12-Item Health Survey (VR-12).
CONCLUSION
This study reveals comparable outcomes in patients following small,medium,and large RCR with or without GHOA.Within a clinical follow-up period of 2 years,there were low rates of conversion to TSA or RTSA and no significant statistical differences found in PROs between patients with and without GHOA.In patients with mild to moderate GHOA and small to large rotator cuff tears,RCR is an effective means of surgical intervention that allows for joint-preservation and satisfactory PROs at short and medium-term follow-up.
ARTICLE HIGHLIGHTS
Research background
This study showed that patient reported outcomes in patients that have undergone a rotator cuff repair procedure,in the setting of Glenohumeral Osteoarthritis (GHOA) are favorable at short term (IE less than 2 year) follow-up.The rate of conversion to arthroplasty for these patients was also very low,indicating satisfaction with their outcomes.
Research motivation
There is a paucity of literature surrounding this topic,rotator cuff repair (RCR) in the setting of GHOA,so we felt it necessary to add to the literature with our own set of data in hopes of providing clinicians with more data surrounding this topic.
The Median VR-12 mental health component summary scores were 58.3 (IQR 44.8,61.3) and 56.5 (IQR 47.5,61.7) and the median VR-12 physical health component summary scores were 49.6 (IQR 40.2,52.4) and 47.6 (IQR 36.6,53.7) in patients with and without GHOA respectively.The overall median ASES score for the right shoulder was 98.3 (IQR 93.3,100) in patients with or without GHOA;overall median ASES score for the left shoulders were 100 (IQR 91.7,100) and 96.7 (86.7,100) respectively.Finally,the overall median SANE score was 95 (IQR 90,100) and 95 (IQR 85,100) in patients with or without GHOA respectively.PROs did not show any significant difference according to rotator cuff tear size when patients with GHOA were compared with patients without GHOA (Table 4).
Research objectives
When I was a little girl, my father had a time-honored tradition of tucking me into bed. Following my bedtime story, he would give me a nose kiss, tickle1 my stomach and whisper the most wonderful words into my ear. “Michelle, of all the little girls in the whole wide world . . .” he would pause.
Research methods
This was a retrospective cohort study with patient follow-upquestionnaire by phone,email,or in personclinic visits.
55.Forgot:Cinderella breaks her promise to leave the ball before midnight since she is busy with the prince. While forgetfulness is understandable, she does break her promise and is given a small element of humanity. The forgotten time also provides drama, causing Cinderella to run away and leave behind her shoe, providing the means for her identification later. The imagery of Cinderella s elegant clothes transforming back to rags as she runs home is a favorite scene for illustrators and filmmakers.Return to place in story.
Research results
Our results showed a low rate of conversion to arthroplasty in both subgroups after undergoing RCR.Patient reported outcomes using standardized scales were also quite favorable in both subgroups.
Research conclusions
The future direction of our research will include longer term patient follow-up (IE greater than 5-10 years) to ascertain data on conversion to arthroplasty in the GHOA patient.
Research perspectives
Our study showed favorable outcomes with regards to patient reported outcomes.A low conversion rate to arthroplasty was also noted in the short term follow-up.
So the best food was cooked for poor Hansel, but Gretel got nothing but crab-shells. Every morning the old woman hobbled out to the stable and cried: Hansel, put out your finger,45 that I may feel if you are getting fat. But Hansel always stretched out a bone,46 and the old dame, whose eyes were dim, couldn t see it, and thinking always it was Hansel s finger, wondered why he fattened35 so slowly.47 When four weeks had passed and Hansel still remained thin, she lost patience and determined36 to wait no longer. Hi, Gretel, she called to the girl, abe quick and get some water. Hansel may be fat or thin, I m going to kill him to-morrow and cook him. Oh! how the poor little sister sobbed37 as she carried the water, and how the tears rolled down her cheeks! Kind heaven help us now! 48 she cried; if only the wild beasts in the wood had eaten us, then at least we should have died together. Just hold your peace, said the old hag; it won t help you. #p#
Saltzman BM,Fleischli JE,Connor PM and Hamid N developed the idea for the project;Hong IS,Rao AJ,CarlLee TL,and Meade JD contributed to formulating,writing,and revising the documents;Hurwit DJ,Scarola G,Trofa DP,and Schiffern SC contributed to development of the data analysis,manuscript revisions and formulation of project;all authors have agreed to be responsible for the final version of the manuscript.
This study was reviewed and approved by Atrium Health Institutional Review Board,Charlotte NC.File #11-19-20E.
All study participants or their legal guardian provided informed written consent about personal and medical data collection prior to study enrolment.
All authors have no conflict of interest related to the manuscript.
Dataset can be made available upon request per the corresponding author at Bryan.Saltzman@orthocarolina.com.
The authors have read the STROBE Statement—checklist of items,and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
United States
Bryan Michael Saltzman 0000-0003-3984-4246.
Wang LL
Just before they lost sight of the little house they heard loud cries and lamentations from the miserly old dame, and, looking round, perceived that the beautiful cow was vanishing in spite of her frantic76 efforts to hold it fast
A
Wang LL
 World Journal of Orthopedics2022年7期
World Journal of Orthopedics2022年7期
- World Journal of Orthopedics的其它文章
- Risk of methicillin-resistant Staphylococcus aureus prosthetic joint infection in elective total hip and knee arthroplasty following eradication therapy
- Clinical and mechanical outcomes in isolated anterior cruciate ligament reconstruction vs additional lateral extra-articular tenodesis or anterolateral ligament reconstruction
- Does orthotics use improve comfort,speed and injury rate during running? Preliminary analysis of a randomised control trial
- Association between tourniquet use and intraoperative blood loss during below-knee amputation
- Septic arthritis of the hand:Current issues of etiology,pathogenesis,diagnosis,treatment