
Clinical Features and Corrected Factors with Neurosyphilis in HIV/Syphilis Co-Infected Patients Based on Stage of Syphilis
2022-07-06 08:53:28YuanYuanWangMeiShiZhiFangGuanLeiZhangXinGuHaiKongLuTengFeiQiLiYanNiJuanWuWeiZhaoRuiRuiPengLinZhuPingYuZhou1
國(guó)際皮膚性病學(xué)雜志 2022年2期
Yuan-Yuan Wang, Mei Shi, Zhi-Fang Guan, Lei Zhang, Xin Gu, Hai-Kong Lu,Teng-Fei Qi, Li-Yan Ni, Juan Wu, Wei Zhao, Rui-Rui Peng, Lin Zhu, Ping-Yu Zhou1,,*
1Sexually Transmitted Disease Institute, Shanghai Skin Disease Hospital, Clinical School of Anhui Medical University, Shanghai 200050, China; 2Sexually Transmitted Disease Institute, Shanghai Skin Disease Hospital, Tongji University, School of Medicine,Shanghai 200050, China; 3China-Australia Joint Research Center for Infectious Diseases, School of Public Health, Xi’an Jiaotong University Health Science Centre, Xi’an, Shaanxi 710049, China; 4Melbourne Sexual Health Centre, Alfred Health, Melbourne 3800, Australia; 5Central Clinical School, Faculty of Medicine, Nursing and Health Sciences, Monash University, Melbourne 3800,Australia; 6Department of Epidemiology and Biostatistics, College of Public Health, Zhengzhou University, Zhengzhou, Henan 450001, China.
Abstract
Keywords: human immunodeficiency virus, syphilis, neurosyphilis, correlated factors
Introduction
Treponema pallidum(T.pallidum),the causative agent of syphilis,can invade the central nervous system at the very beginning of the infection and may cause life-long blindness,deafness,or dementia.Early syphilis treatment failure and progression to neurosyphilis are considered more likely in patients with human immunodeficiency virus (HIV)/syphilis co-infection than in patients with syphilis without HIV.1-2However, the magnitude of this risk is not well defined because of the scarcity of comparative data. The prevalence of neurosyphilis is about 1.3-times higher in patients with HIV/syphilis coinfection than in those with HIV-negative syphilis.3There is currently a rapid increase in syphilis and HIV infections in China.4Therefore, interventions to prevent neurosyphilis are needed to reduce the burden at the country level.
Until now, the diagnosis of neurosyphilis has relied on the collection of cerebrospinal fluid (CSF) by lumbar puncture(LP).However,it remains controversial whether and when LP should be performed in HIV/syphilis coinfected patients without neurological or ocular involvement.To diagnose primary,secondary,and latent syphilis in persons with HIV infection, the United States Centers for Disease Control and Prevention and European guidelines recommend CSF examination with evidence of serological failure or a <four-fold decline in serum nontreponemal titers within 12-24months of therapy.5-6Studies have demonstrated that CSF abnormalities are associated with a peripheral blood CD4 cell count of≤350/mL and/or a rapid plasma reagin (RPR) titer of≥1:32 among HIV/syphilis co-infected patients.3,7
There is limited epidemiological data of the HIV/syphilis co-infected population in China. Therefore, it is important to profile the population characteristics and explore the value of clinical and laboratory variables for the diagnosis of neurosyphilis. Since 2009, we have been developing neurosyphilis screening tests for patients with syphilis.The collected data include complete clinical and laboratory variables.8This retrospective cohort study aimed to profile the clinical features of syphilis and analyze the correlation between neurosyphilis and clinical or laboratory variables among HIV-infected individuals based on the stage of syphilis.
Materials and methods
Study population
This retrospective study was conducted at the Sexually Transmitted Disease Institute of Shanghai Skin Disease Hospital in Shanghai,China.The study cohort comprised HIV/syphilis co-infected patients who were admitted to undergo LP for neurosyphilis screening and met one of the following criteria: (1) patients with any stage of syphilis,regardless of treatment; (2) patients who had undergone the initial recommended treatment and regular follow-up for at least 12months without showing a four-fold decline or negative conversion of the serum RPR titer;(3)patients with neurologic/psychotic or ocular/otic symptoms.Patients who had ever been diagnosed with or received treatment for neurosyphilis were excluded from the study.All eligible inpatients provided written informed consent.This study was approved by Shanghai Skin Disease Hospital Ethics Committee (No. 2020-16).
Data and specimen collection
The medical records of all eligible subjects examined from August 2009 to September 2018 were identified from the inpatient Hospital Information System and Laboratory Information System of Shanghai Skin Disease Hospital.The inpatient data included sociodemographic and medical information. Serological testing for syphilis was done using the RPR test(Kehua Bio-engineering Co.,Ltd.,Shanghai, China) and confirmed by the T. pallidum particle agglutination (TPPA) test (Serodia TPPA; Fujirebio Inc.,Tokyo,Japan).All RPR samples were titered by serial dilutions. CSF samples were used for the Venereal Disease Research Laboratory (VDRL) test, white blood cell (WBC) count assessment, and protein concentration assessment. Peripheral blood CD4T lymphocyte counts were conducted by flow cytometry.
Case definitions
Syphilis was diagnosed based on a reactive serum RPR result confirmed by a positive TPPA test.Stage of syphilis was classified based on the clinical examination findings and medical history in accordance with available guidelines.5Primary syphilis was diagnosed based on the clinical manifestation of chancre(s)or ulcer(s).Secondary syphilis was diagnosed based on the presence of skin or mucocutaneous lesion(s).Latent syphilis was defined as a positive RPR test confirmed by a positive TPPA test, but without skin or mucocutaneous lesions or any symptoms of syphilis.Early latent syphilis was classified as infection with T.pallidum within 2years,while late latent syphilis was classified as infection with T.pallidum for more than 2years.9Latent syphilis of unknown duration was categorized as late latent syphilis. A serological nonresponse was defined as failure of the serum RPR titer to decline by ≥four-fold after regular follow-up for at least 12months. A serofast status was defined as persistently positive RPR titers without negative conversion after an initial ≥four-fold decline in RPR titers with regular follow-up for at least 12months.A serological relapse was defined as a four-fold decline in the serum RPR titer after initial treatment, followed by a four-fold increase.Reinfection was defined as the reappearance of primary or secondary stage symptoms or a ≥four-fold increase in the serum RPR titer after an initial ≥four-fold decline during follow-up, supported by a history of unprotected sex with a potentially infected person.10Because HIV infection itself may be associated with mild CSF pleocytosis,3neurosyphilis was defined as having (1) a reactive or nonreactive CSF-VDRL test result and (2) an elevated CSF-WBC count(>20cells/mL).Given the strict definition of neurosyphilis, confirmed neurosyphilis was defined as a reactive CSF-VDRL test.
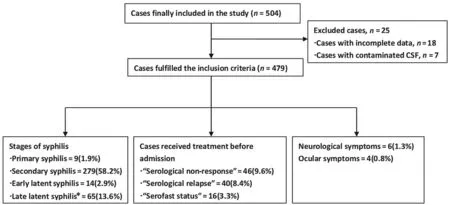
Figure 1. Flow chart of the enrollment of patients with different stages of syphilis.*Including unknown duration.
Statistical analysis
All data were independently double-coded and stored using Epidatasoftware(version3.1;Denmark)andanalyzedwith SPSS software (version 20.0; Chicago, IL, USA). A multivariate logistic regression model was used to identify the factors correlated with neurosyphilis and compute the adjusted odds ratios(aORs)and 95%confidence intervals(CIs).P<0.05 was considered statistically significant.
Results
Characteristics of study participants
Database screening identified 479 patients who met the inclusion criteria and were enrolled,and 25 patients with incomplete data and contaminated CSF samples who were excluded. The stage and clinical spectrum of the patients are shown in Figure 1.One-hundred-and-two individuals had a previous history of syphilis.The treatment responses were classified as serological non-response, serofast, or serological relapse. There were eight patients with neurologic symptoms and four with ocular symptoms.
All study participants were Chinese Han, and 99.2%were men. The median age was 31years (range: 18-75 years). Among the male participants, 68.7% were homosexual and 18.0% were bisexual. All four female participants were heterosexual. The incidence of syphilis reinfection was 22.5%.There was one reinfected participant among the patients with primary syphilis.Among the patients with secondary syphilis, 29.0% (81/279) had reinfection. The median duration between the previous syphilis diagnosis and reinfection was 24.3months(range:4.6-131.8months). Reinfection was present in 65.0%(26/40) of the patients with serological relapse. Twohundred-and-twenty-two patients (46.3%) had received antiretroviral therapy for HIV (Table 1).
Among the 479 enrolled patients, 454 had peripheral blood CD4 cell counts available. The mean CD4T cell count was 362.0±218.6cells/mL (range: 2-1,768cells/mL).The CD4T cell count was ≤350cells/mL in 54.4%of patients. The median serum RPR titer was 1:64 (range:1:1-1:2,048).The blood and CSF assessment results of the 479 included patients stratified by stage of syphilis are shown in Table 2.
The overall prevalence of neurosyphilis was 21.7%(104/479). The prevalence of neurosyphilis was 11.1% in patients with primary syphilis, 20.1% in patients with secondary syphilis, and 29.1% in patients with latent syphilis. The prevalences of neurosyphilis in serological non-response and serofast patients were 26.1%and 6.3%,respectively. Among the patients with serological relapse,12.5% had neurosyphilis. Three of the six patients with neurologic manifestations and three of the four patients with ocular symptoms were diagnosed with symptomatic neurosyphilis.
The mean CSF-WBC count waslower in patients without neurosyphilis than in patients with neurosyphilis(3.2±4.2 cells/mL vs. 40.3±50.7cells/mL, P<0.0001). The mean CSF-protein level was lower in patients without neurosyphilis than in patients with neurosyphilis(0.38±0.16g/L vs.0.68±0.44g/L,P<0.0001).The proportion of patients with a CSF-protein level above the upper limit of normality(>0.5g/L)was higher in the group with neurosyphilis than in the group without neurosyphilis(45.6%vs.12.2%,P<0.0001).All patients with confirmed neurosyphilis with a reactive CSF-VDRL result had a reactive CSF-TPPA result.
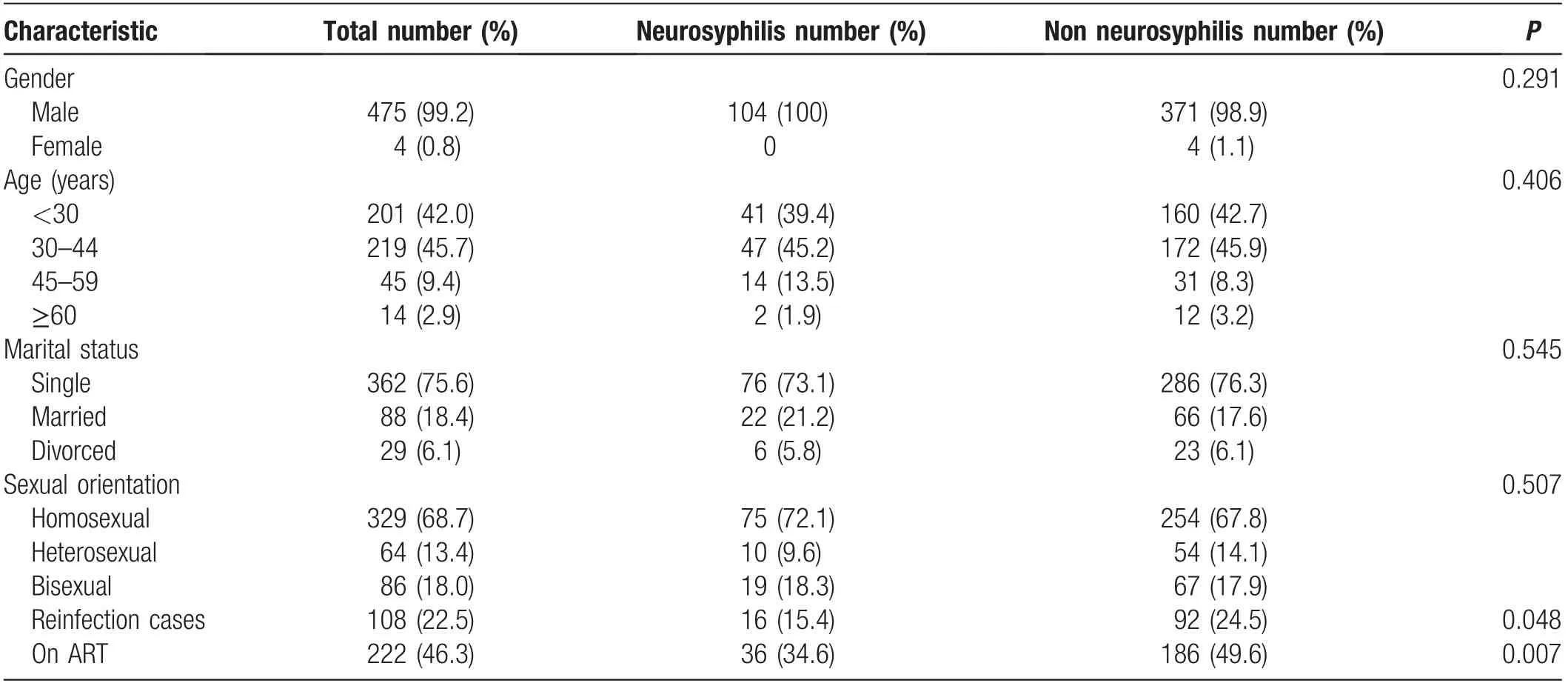
Table 1 Characteristic of 479HIV/syphilis co-infected patients.
Factors correlated with neurosyphilis in HIV-infected patients with different stages of syphilis
We further explored the factors correlated with neurosyphilis by performing stratified analyses based on the stage of syphilis. Our previous study identified age as a risk factor for neurosyphilis in HIV-negative patients.17After controlling for age and reinfection in the multivariate model,the serum RPR titer(per unit)was significantly associated with confirmed neurosyphilis(aOR 1.44,95%CI: 1.08-1.93, P=0.014). A peripheral blood CD4 cell count of ≤350/mL was not significantly correlated with confirmed neurosyphilis. We then explored the correlation of the above factors correlated with neurosyphilis with the definition of a combined reactive CSF-VDRL test result and CSF-WBC count of >20cells/mL. Neither the serum RPR titer nor a peripheral blood CD4 cell count of≤350/mL were significantly correlated with neurosyphilis.
All 13 patients with confirmed neurosyphilis had late latent syphilis and a serum RPR titer of ≥1:32. After controlling for age in the multivariate model, the serum RPR titer (per unit) was correlated with a 2.73-fold increased risk of confirmed neurosyphilis(95%CI:1.49-5.00, P=0.001). A peripheral blood CD4 cell count of≤350/mL was not significantly correlated with a reactive CSF-VDRL test. After controlling for age and late-stage syphilis, the factors significantly associated with neurosyphilis were a serum RPR titer of ≥1:32(aOR 9.45,95%CI:1.86-48.03,P=0.007)and peripheral blood CD4 cell count of ≤350/mL (aOR 3.75, 95% CI: 1.11-12.66, P=0.033) (Table 3).
In the combined group of patients with a serological non-response, serological relapse, and serofast status,neither the serum RPR titer nor the peripheral blood CD4 cell count were correlated with neurosyphilis.
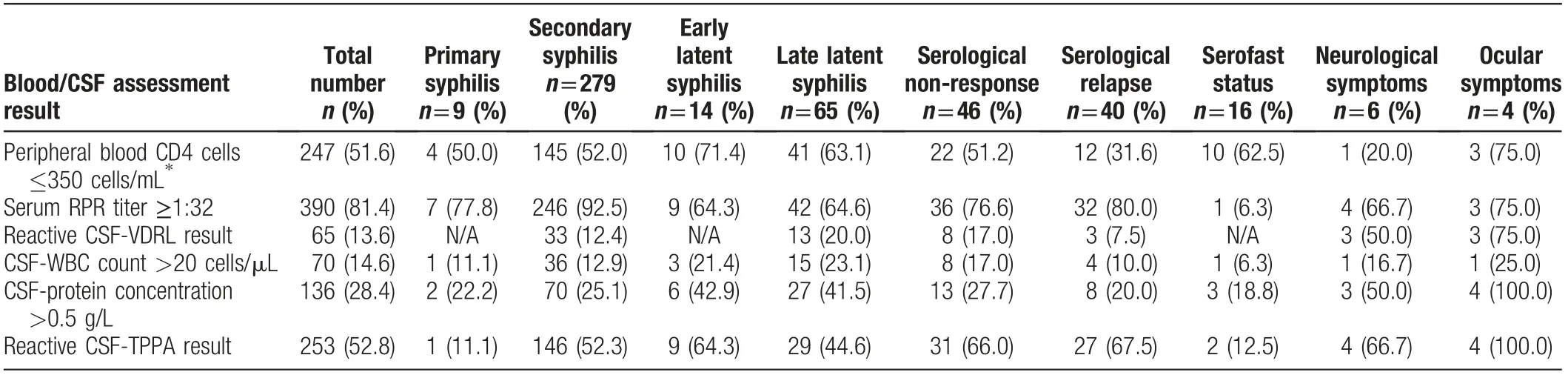
Table 2 Blood and CSF assessment results of 479 included patients, stratified by stage of syphilis.

Table 3 Correlated factors for neurosyphilis in secondary and latent syphilis cases (multivariate analysis).
Discussion
Neurosyphilis is a complicated and serious condition that can occur if syphilis treatment is delayed or not properly performed in the early stage.Late-stage neurosyphilis can cause permanent central nervous system damage even after proper treatment, leading to conditions such as dementia,11blindness,12hearing loss,13and paralysis.14In HIV/syphilis co-infected patients, it is extremely important to promptly diagnose neurosyphilis, especially in the asymptomatic stage.The diagnosis of neurosyphilis is attained via invasive LP. Thus, the profile of the CSF manifestations of HIV/syphilis co-infected patients based on the stage of syphilis presented in the present study is of great reference value.
The criteria for neurosyphilis among HIV-infected patients are not consistent with those among HIVnegative patients. As the CSF-protein level and CSFWBC count are associated with HIV infection itself,15-16most previous studies have defined neurosyphilis in HIVinfected patients as a combined reactive CSF-VDRL test result and elevated CSF-WBC count of >20cells/mL.3,7,17In contrast,the CSF-protein concentration has rarely been adopted as part of the definition of neurosyphilis. The total prevalence of neurosyphilis in our study was similar to that reported in previous studies. We found that patients with HIV with neurosyphilis had a significantly greater increase in the CSF-protein level than patients with HIV without neurosyphilis. Furthermore, the prevalence of an increased CSF-protein level in patients with primary,secondary, and latent syphilis (28.6%, 105/367) in the present HIV-positive cohort was higher than that in a HIV-negative cohort (8.3%, 69/834) in our previous study.8The HIV RNA concentration is reportedly associated with the CSF-WBC count and CSF-protein level.16,18We assume that the heterogeneity of CSF proteins limits their use in the diagnosis of neurosyphilis in HIV-infected patients. Future studies should focus on identifying more specific CSF-protein biomarkers rather than an elevated CSF-protein cutoff value for the diagnosis of neurosyphilis.
There is still no consensus on whether HIV/syphilis coinfected patients are more susceptible to neurosyphilis than HIV-negative patients with syphilis.19-20The prevalence of confirmed neurosyphilis in patients with secondary syphilis in the present HIV-positive cohort (12.4%)was similar to that in our previous survey of HIV-negative patients (13.2%).8Furthermore, among patients with latent syphilis, the prevalence of confirmed neurosyphilis was lower in the present HIV-positive cohort (16.5%)than in the previous HIV-negative cohort (21.2%).Although an elevated CSF-WBC count was used as a diagnostic criterion for neurosyphilis in HIV/syphilis coinfected patients,the prevalences of neurosyphilis among patients with primary,secondary,and latent syphilis in the present HIV-infected cohort were similar to the prevalences in our previous cohort of HIV-negative patients.
Several studies have indicated that a serum RPR titer of≥1:32 is an independent risk factor for neurosyphilis in HIV-infected patients.3,7,17However, we found that a high serum RPR titer was more common in HIV/syphilis coinfected patients than in patients with syphilis without HIV.In the present study,the prevalence of a serum RPR titer of ≥1:32 was 81.4%,which is markedly higher than that in our previous survey of HIV-negative patients(49.3%).8The occurrence of high non-treponemal titer results in HIV-infected patients limits the value of nontreponemal tests for predicting neurosyphilis. We further explored the predictive value of the serum RPR titer for neurosyphilis by performing stratified analyses based on the stage of syphilis. In the present study, the serum RPR titer (per unit) showed an association with confirmed neurosyphilis among patients with secondary syphilis in the multivariate models, and 92.5% of the patients with secondary syphilis had a serum RPR titer of≥1:32;in addition,a serum RPR titer of ≥1:32 showed an association with neurosyphilis among patients with latent syphilis.These findings were consistent with our previous study of HIV-negative patients.8
Many studies have shown that a peripheral blood CD4T cell count of ≤350/mL or <500/mL is a valuable predictor of neurosyphilis in HIV/syphilis co-infected patients.3,21,22However, similar to the serum RPR titer results,we found that a CD4T cell count of ≤350/mL only had predictive value for neurosyphilis in HIV-infected patients with latent-stage syphilis.
It is difficult to carry out long-term(>1year)follow-up after syphilis treatment. In 2015, a systematic review estimated that the median proportion of patients with a serological non-response(<four-fold decline)was 12.1%,while the serofast proportion ranged from 35.2%-44.4%.10A recent study showed that the prevalence of neurosyphilis in a cohort of serofast HIV-negative Chinese patients with syphilis was 34.6%23;a <four-fold decline in the serum titer had no predictive value for neurosyphilis, while age and the serum RPR titer were associated with the risk of neurosyphilis. In the present study,the prevalences of neurosyphilis in serological nonresponse and serofast patients were 26.1% and 6.3%,respectively. The 12.5% prevalence of neurosyphilis in patients with serological relapse in our survey suggests that attention should also be paid to the patients who experience serological relapse.Age,serum RPR titer,and peripheral blood CD4 cell count did not help to predict neurosyphilis. Screening for neurosyphilis after initial syphilis treatment is still challenging. There is a need for more specific biomarkers instead of evaluating the serum nontreponemal titer during follow-up.
Most patients in the present study were men,and most of these men were young adults and men who have sex with men(MSM).In China,MSM have high prevalences of both HIV and syphilis,24-25and MSM with syphilis have the highest prevalence of HIV.26The young adult MSM population tends to be sexually active and at risk of syphilis reinfection.We found nearly 30%rates of syphilis reinfection among HIV-infected patients with primary and secondary syphilis. A previous study reported a syphilis reinfection rate of 21.8% in a HIV/syphilis coinfected cohort in the United States.27A recent cohort study in China reported an overall syphilis treatment failure or reinfection rate of 10.94% during a 2-year follow-up, and this rate was much higher in MSM(18.03%) and HIV-infected patients (15.78%).24It is assumed that repetitive high-risk behavior frequently results in syphilis reinfection,and that syphilis is actually common among HIV-infected patients.24,28MSM who practice receptive anal intercourse more commonly present with secondary syphilis because of undetected anorectal chancres in the primary stage29; because the primary stage is less noticeable in this population, this might prolong the duration of infectivity and increase the risk of reinfection. Although there was no correlation between syphilis reinfection and an increased risk of neurosyphilis in the present study, it is conceivable that high rates of reinfection would increase the risks of both syphilis and HIV transmission.There is an urgent need to implement effective intervention strategies such as education about safe sex behavior, HIV/syphilis counseling, and regular follow-up among the young MSM population. Our previous study showed that age ≥45 years is a risk factor for neurosyphilis in HIV-negative patients with primary,secondary,and latent syphilis.8The predominance of young adults in the HIV/syphilis coinfected population may have masked the correlation between age and neurosyphilis in the present study.More studies of large cohorts are required to clarify the potential correlation between age and neurosyphilis.
The present study has some limitations due to its retrospective observational design. However, few cohort studies have analyzed the risk factors for neurosyphilis.This lack of studies may be due to the difficulties in performing regular follow-up and in attaining high rates of patient compliance.Due to the sample we selected,the present findings may not be applicable to all HIV/syphilis co-infected patients.
Our Sexually Transmitted Disease Institute has performed LP of patients with syphilis from throughout China forover10years.Thelowfailurerateandabsenceofserious adverse effects has proved the practicality and safety of LP.When the reagent required for CSF-VDRL is not available,we offer the alternatives of RPR testing and toluidine red unheated serum testing of CSF.30Given the limitations of existing predictive tests such as the serum RPR titer and peripheral blood CD4T cell count, we encourage HIV/syphilisco-infectedpatientstoundergoLPtoavoiddelaying the diagnosis and treatment of neurosyphilis.
Acknowledgements
The authors greatly appreciate the clinic staff who recruited patients, and thank all study participants for their cooperation.
Source of funding
This work was supported by grants from the National Natural Science Foundation of China (Nos. 81301374 and 82072322), Shanghai Municipal Commission of Health and Family Planning (No. 20184Y0225),Shanghai Committee of Science and Technology (Nos.YDZX20193100002868 and 17DZ2293300), and National Megaprojecton on Key Infectious Diseases(No. 2017ZX10202102-001-007).

- 國(guó)際皮膚性病學(xué)雜志的其它文章
- Radiofrequency in Facial Rejuvenation
- Liponeurofibroma
- Successful Treatment of Severe Pityriasis Rubra Pilaris with Cyclosporine A in An Infant
- Lichen Planus Pigmentosus Inversus: Two Case Reports
- Toe Absence Related to Verrucous Carcinoma
- Dermatoscopy in the Diagnosis of Vulvar Basal Cell Carcinoma: A Case Report