
Βiliary obstruction following transjugular intrahepatic portosystemic shunt placement in a patient after liver transplantation:A case report
2022-07-04 07:37:30PeterMacingaDarinaGogovaJanRaupachJanaJarosovaLiborJanousekEvaHonsovaPavelTaimrJuliusSpicakJiriNovotnyJanPeregrinTomasHucl
World Journal of Hepatology 2022年5期
Peter Macinga,Darina Gogova,Jan Raupach,Jana Jarosova,Libor Janousek,Eva Honsova,Pavel Taimr,Julius Spicak,Jiri Novotny,Jan Peregrin,Tomas Hucl
Peter Macinga,Darina Gogova,Jana Jarosova,Pavel Taimr,Julius Spicak,Tomas Hucl,Department of Gastroenterology and Hepatology,Institute for Clinical and Experimental Medicine,Prague 14021,Czech Republic
Jan Raupach,Department of Radiology,University Hospital,Hradec Kralove 50005,Czech Republic
Libor Janousek,Department of Transplant Surgery,Institute for Clinical and Experimental Medicine,Prague 14021,Czech Republic
Eva Honsova,Department of Pathology,Institute for Clinical and Experimental Medicine,Prague 14021,Czech Republic
Jiri Novotny,Jan Peregrin,Department of Diagnostic and Interventional Radiology,Institute for Clinical and Experimental Medicine,Prague 14021,Czech Republic
Abstract BACKGROUND Transjugular intrahepatic portosystemic shunt(TIPS)is a method used to decrease portal hypertension.Biliary stricture is the rarest of the complications associated with this procedure with only 12 cases previously reported in the literature.None of these cases have documented the resolution of biliary stenosis induced by a stent graft.The only curative solutions reported are liver transplantation or bypassing the stenosis with an artificial biliary tract using advanced endoscopic techniques.CASE SUMMARY This is the first reported case of biliary obstruction secondary to TIPS placement in a transplanted liver.In our patient,a portosystemic shunt was created to treat severe veno-occlusive liver graft disease manifesting itself primarily by fluid retention.A cholestatic liver lesion and cholangitis with abscesses developed due to a stent graft-induced stricture in the dorsal segment of the right hepatic duct and the stricture diminished following percutaneous drainage.Endoscopic drainage was performed after unsuccessful removal of the percutaneous catheter resulting in a bilio-cutaneous fistula.Although the liver graft now functions well,the stricture remains refractory even after 44 mo of treatment.CONCLUSION Biliary strictures caused by TIPS in both transplanted and native livers seem refractory to endoscopic treatment.
Key Words: Biliary stricture;Transjugular intrahepatic portosystemic shunt;Liver trans-plantation;Sinusoidal obstruction syndrome;Literature review;Case report
lNTRODUCTlON
Transjugular intrahepatic portosystemic shunt(TIPS)is a procedure in which an artificial portosystemic shunt is applied to decrease portal hypertension.The most common indications are refractory ascites and uncontrolled variceal bleeding which often serves as a bridge to liver transplantation.Common complications of TIPS include encephalopathy,cardiac failure,occlusion and infection.Serious biliary complications are rare and occur in less than 1% of cases[1].
TIPS insertion can create a tract between the shunt and non-vascular structures,typically resulting in a biliary-TIPS fistula.This fistula can cause haemobilia and jaundice and is associated with acute and chronic TIPS occlusion[2].Such complications have been significantly reduced with the use of covered stent grafts.Biliary stenosis secondary to TIPS placement is extremely rare with only 12 cases documented(7 case reports and 1 case series)(Table 1).Interestingly,a single-center retrospective study found TIPS-related segmental intrahepatic cholestasis in 4 of 135 intervened patients(2.9%)[3].However,this observation has yet to be confirmed by further studies.
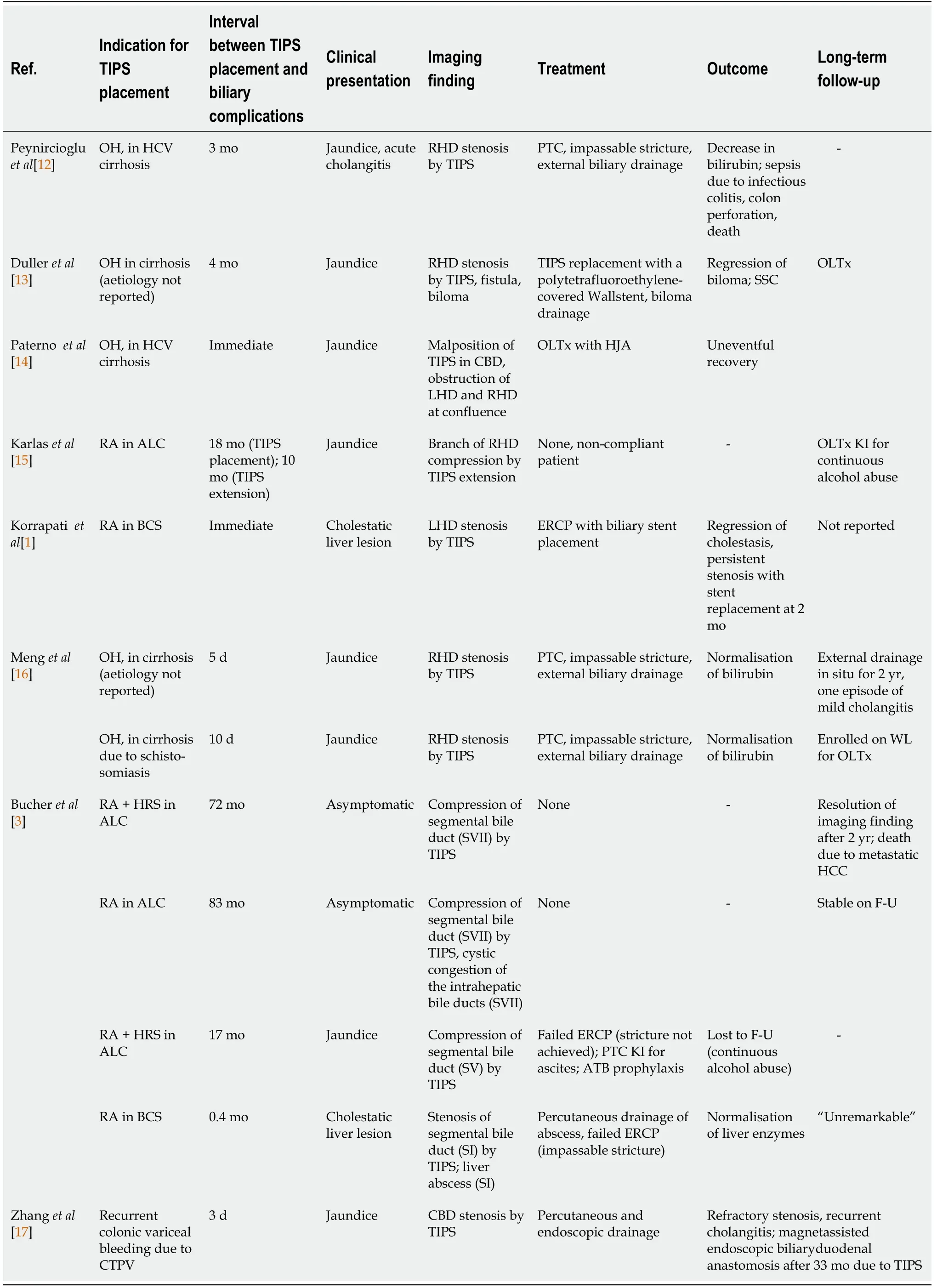
Table 1 Characteristics of previously published cases of transjugular intrahepatic portosystemic shunt-induced biliary strictures
This report documents the very first case of a TIPS-related bile duct stricture in a liver graft.
CASE PRESENTATlON
Chief complaints
Dyspnoea in a patient early after liver transplantation.
History of present illness
A 40-year-old Caucasian male underwent orthotopic liver transplantation for alcoholic liver cirrhosis(see Figure 1 for timeline).He received a full graft from an ABO-compatible 74-year-old cadaveric donor.Cold ischemia time was 3 h 21 min.The transplantation was performed using piggyback technique with side-to-side caval anastomosis(Belghiti Technique)and standard end-to-end hilar anastomoses.The duration of the procedure was 2 h 52 min.The postoperative course was uneventful.The immunosuppressive regimen consisted of tacrolimus,mycophenolate mofetil and corticosteroids.A month later,the patient presented with symptomatic ascites,large right-sided pleural effusion and normal liver function.Upper endoscopy revealed esophageal varices and the consequent catheterization of the hepatic veins showed a portosystemic gradient of 28 mmHg.Liver biopsy revealed microvascular damage corresponding to sinusoidal obstruction syndrome(SOS)(Figure 2).The patient wassubsequently indicated for placement of a TIPS stent graft.This procedure was successfully performed and reduced the portosystemic gradient to 11 mmHg(Figure 3).Immediately after placement of the shunt,a rise in cholestatic enzyme levels was observed.
Figure 1 Timeline of the reported case.ALC: Alcoholic liver cirrhosis;B-C: Bilio-cutaneous;I-E: Internal-external;OLTx: Orthotopic liver transplantation;RHD: Right hepatic duct;SOS: Sinusoidal obstruction syndrome.
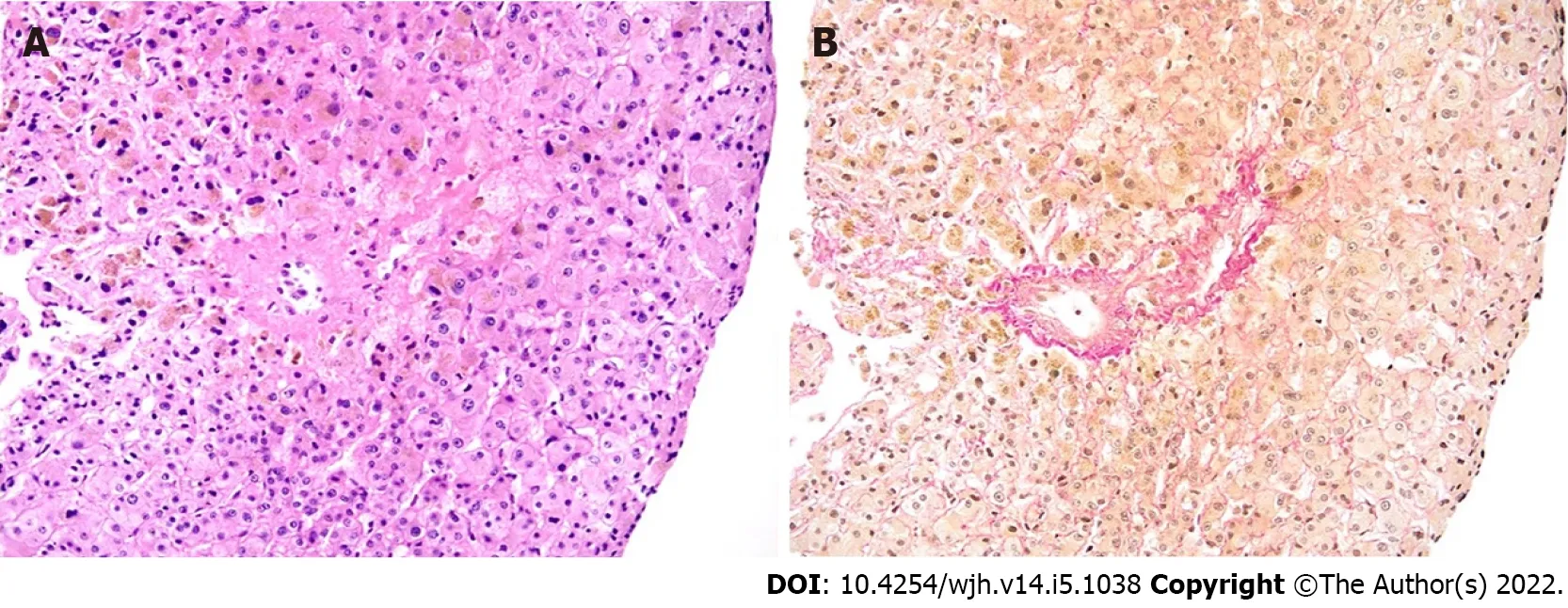
Figure 2 Histological findings in liver biopsy.Centro lobular vein with wall edema and narrowing of the lumen by connective tissue,focal obstructive fibrosis of the surrounding sinuses;hematoxylin-eosin(A)and Elastica van Gieson(B)staining,original magnification x 100.

Figure 3 Transjugular intrahepatic portosystemic shunt implantation.
History of past illness
In the pre-transplant period,the patient was diagnosed with alcoholic liver cirrhosis but displayed no other significant comorbidities.He suffered from several severe episodes of hepatic encephalopathy(including coma)and was also treated for hepatorenal syndrome.At the time of transplantation,he had a MELD score of 27 and his Child-Pugh class was C(14 points).
Personal and family history
The patient had a history of alcohol addiction but had been abstaining from alcohol for 2 years before liver transplantation.He had smoked 20 cigarettes a day for 20 years prior to quitting 18 mo prior to the present illness.His family history was unremarkable.
Physical examination
Upon initial examination,the patient was sarcopenic,pale,anicteric and dyspneic at rest with an oxygen saturation of 88%.He had tachycardia at 102 pulses per minute but blood pressure was within normal values.Breath sounds were inaudible on the right side and percussion in the right chest was dull.The patient exhibited large ascites and a palpable liver but no lower-limb oedema.No remarkable abdominal wall collateral vessels were noted on physical examination.After TIPS placement,we observed a significant regression in physical signs of both ascites and pleural effusion.
Laboratory examinations
Upon admission,bilirubin and liver enzymes were within normal limits(total bilirubin 0.86 mg/dL,AST 18.67 U/L,ALT 26.51 U/L,ALP 96.58 U/L and GGT 62.99 U/L).Total serum protein was 46.5 g/L and the albumin level was 23.7 g/L.After shunt placement,we observed an elevated ALP(292.74 U/L)and GGT(435.51 U/L),but levels of bilirubin,AST and ALT remained at normal values.
Imaging examinations
The initial abdominal ultrasound showed marked hepatomegaly(20.5 cm in the craniocaudal length)and massive ascites.After TIPS placement,liver ultrasound revealed a patent shunt with appropriate blood flow.Subsequent magnetic resonance analysis revealed tight stenosis of the right dorsal hepatic duct caused by the compression of the previously placed stent graft with prestenotic tract dilation and multiple small abscesses(Figure 4).
FlNAL DlAGNOSlS
The patient was diagnosed with cholangitis and abscess formation due to biliary stenosis secondary to TIPS.
TREATMENT
Intravenous antibiotics were administered.Endoscopic cholangiography confirmed our previous magnetic resonance finding.However,an attempt at biliary stent placement proved unsuccessful(Figure 5A).Following failed endoscopic drainage,an internal-external catheter was placed percutaneously(Figure 5B).
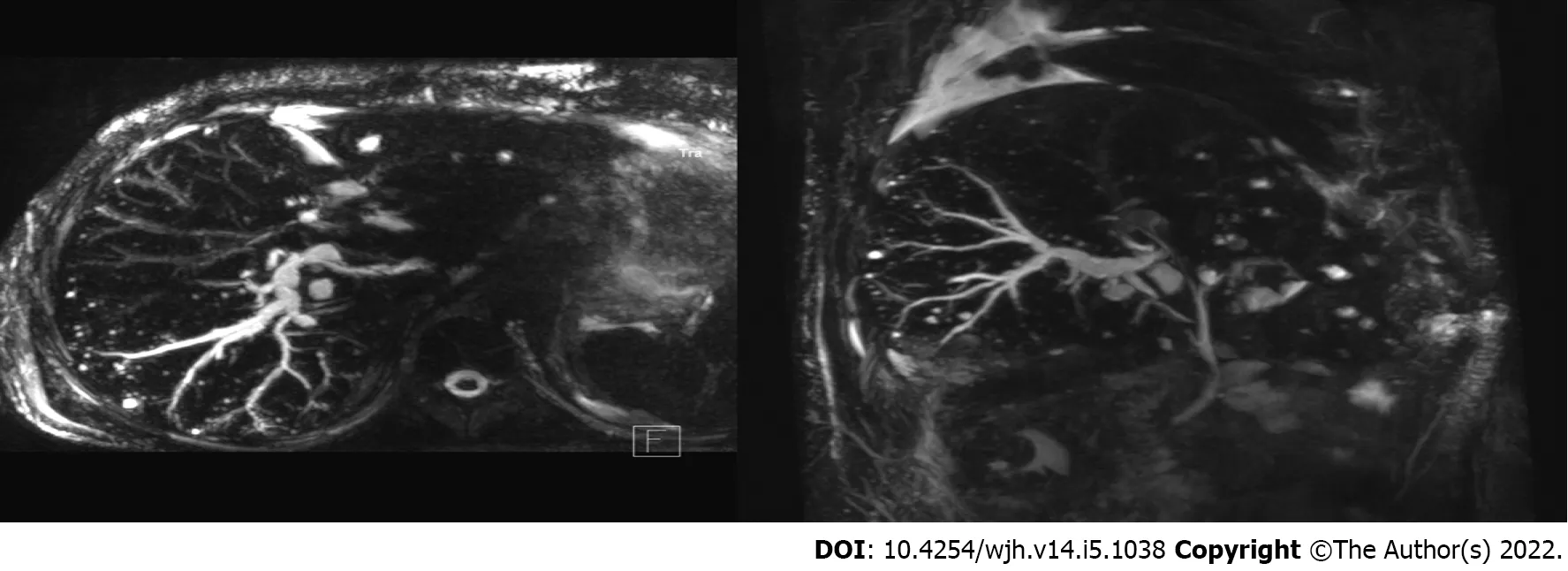
Figure 4 Magnetic resonance imaging scan after transjugular intrahepatic portosystemic shunt placement.Dilation of dorsal branch of right hepatic duct with multiple small abscesses of the right lobe.
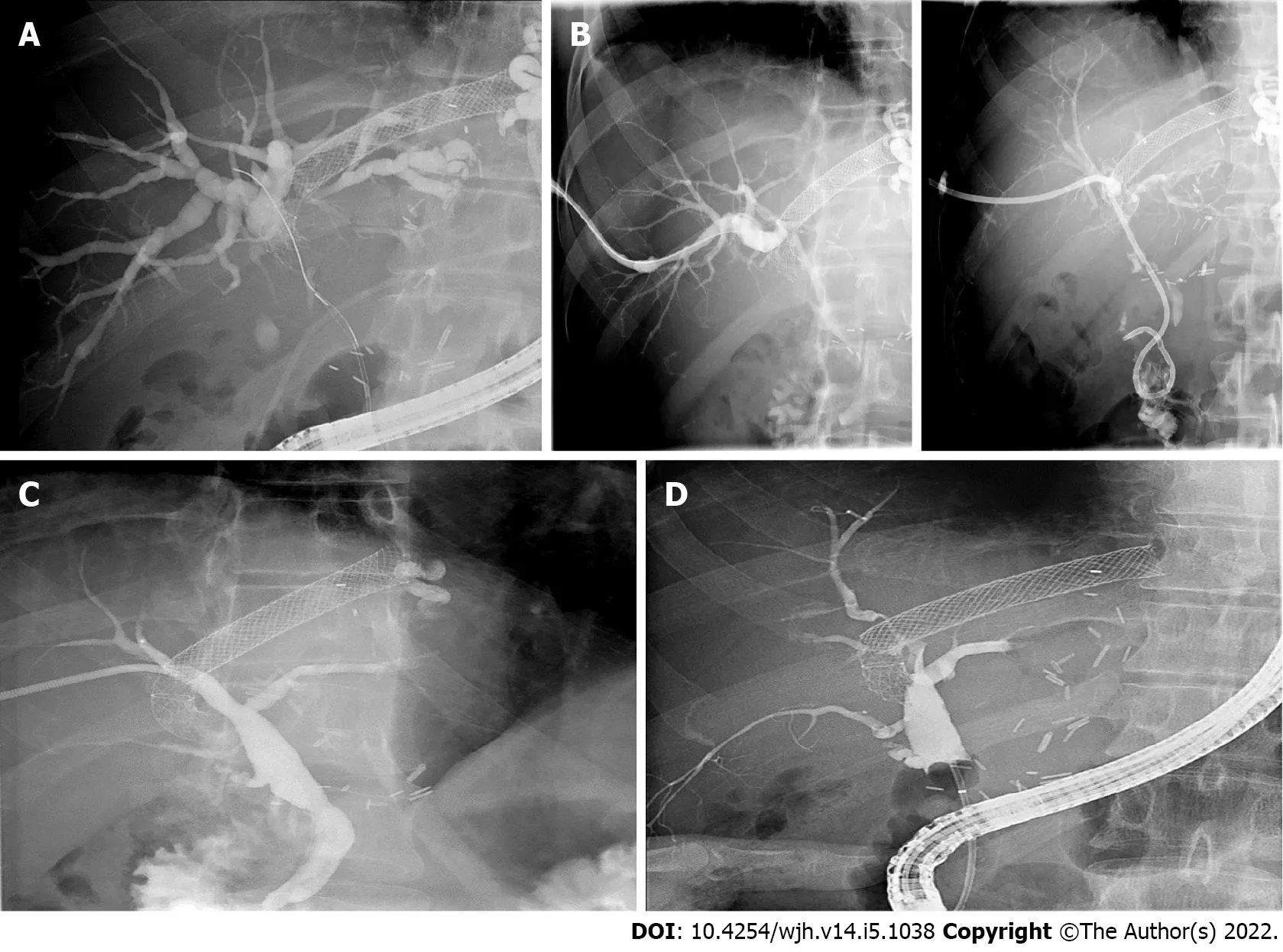
Figure 5 lmages of cholangiogram.A: Endoscopic cholangiogram.Tight stenosis in the dorsal segment of the right hepatic duct caused by the transjugular intrahepatic portosystemic shunt stent graft;stent not placed;B: Percutaneous cholangiogram.Stricture passed with a wire;external-internal catheter placed in duodenum;C: Percutaneous cholangiogram.Apparent regression of the visualized stricture with drain removed;D: Eight endoscopic cholangiograms.Persistent stricture of the right hepatic duct.
OUTCOME AND FOLLOW-UP
Percutaneous intervention led to a prompt reduction in cholestasis and the disappearance of hepatic abscesses.As a result,the patient was discharged.During follow-up,ascites and pleural effusion resolved completely.After 17 mo involving five replacements of the percutaneous drain,we observed a significant regression in biliary stenosis allowing for drainage extraction(Figure 5C).Shortly afterwards,however,the patient presented with a biliary leak due to opening of the cutaneous channel.Endoscopic cholangiography revealed persistent biliary stenosis.Endoscopic stent placement resulted in the resolution of the biliary fistula.Over the next 26 mo,the patient underwent eight ERCPs with repeated balloon dilations and stent replacements.Stricture location and anatomy do not allow for metal stent implantation and the stenosis has thus far proved refractory to treatment(Figure 5D).To date,the patient has suffered from two episodes of acute cholangitis and the liver graft has remained functional.
DlSCUSSlON
Biliary complications are common in liver transplant recipients occurring in approximately 30% of patients[4].Among the most common are anastomotic(AnS)and non-anastomotic strictures(nAnS),with incidence of 6%-12% and 0.5%-10%,respectively[5].Anastomotic strictures account for up to 80% of all stenotic complications and respond excellently to endoscopic treatment,especially those that occur early(< 3 mo after OLTx)[4].AnS require the placement of repetitive multiple plastic stents or selfexpandable metal stents to achieve sufficient radial tension.Recurrence of the stricture after treatment is uncommon,representing less than 20% of cases[6].In contrast to AnS,endoscopic treatment of nAnS is difficult and often unsuccessful,resulting in compromised graft survival[7].We know of no other reported case of non-anastomotic stricture in a transplanted liver due to TIPS placement.
Hepatic sinusoidal obstruction syndrome(SOS;previously known as veno-occlusive disease)is a rare endothelial disorder that occurs particularly after exposure to drugs or toxins.Obstruction of the terminal hepatic venules and sinusoids is typical following hematopoietic cell transplantation and as a consequence of myeloablative preparation(in up to 15% of patients)[8].SOS is also infrequently observed in liver transplant recipients(with an approximate prevalence of 2%)[9],presumably as an immune-mediated condition related to rejection episodes or azathioprine therapy.SOS is also associated with inferior graft and patient survival[9,10].The typical clinical manifestation of the disease is a triad of hepatomegaly,fluid retention and jaundice;treatment usually relies on fortification of immunosuppression.A few other pharmacological agents can be used for SOS therapy,but evidence of their efficacy in solid organ transplant recipients is limited.It has been documented that in the case of severe disease refractory to medical treatment,TIPS placement prior to re-transplantation is a justifiable therapy in patients after liver transplant;however,very few cases have been reported in the literature[11].
In our case,veno-occlusive disease manifesting in hepatomegaly and portal hypertension was successfully treated by TIPS intervention.Cholestatic injury developed as a consequence of biliary stenosis induced by the TIPS stent graft.The tight stenosis initially only allowed for percutaneous drainage,which was then converted to internal biliary stents after an unsuccessful attempt at removal.To date,even after a total follow-up time of 44 mo,endoscopic treatment has failed to resolve the stenosis.The patient remains dependent on repeated stent exchange due to refractory and persistent right hepatic duct stenosis.
Our observations are consistent with the outcomes of previously reported cases.Biliary stenosis due to TIPS has been reported in twelve patients thus far.In ten of these(83%)cases,patients were symptomatic and required treatment.Seven patients were indicated for biliary drainage: ERCP was attempted in three patients and percutaneous therapy in four patients.ERCP as a first-line treatment was technically successful only in one of the three patients,failing in the remaining two.One patient was contraindicated for percutaneous drainage due to ascites,but ERCP subsequently failed and the patient was lost to follow-up.In the other patient,laboratory findings normalized solely due to percutaneous drainage of a hepatic abscess proximal to the stricture.Surprisingly,however,the longterm outcome of this patient was designated “unremarkable” in spite of the stenosis having not been resolved.A primary percutaneous approach was successful in all of the remaining four cases.However,in three of these cases,only external drainage due to an impassable stricture was possible,with the fourth patient later converted to internal drainage.Altogether,successful stenting of TIPS-induced stenosis has been reported in only two published cases,both having either unknown or unfavorable long-term outcomes.While in the first patient only a very short 2-mo follow-up was reported,in the second patient the stricture remained refractory even after almost 3 years of percutaneous and subsequent endoscopic drainage.
The above observations may be attributable to characteristic differences between TIPS-induced stenosis and other etiologies.In TIPS-induced stenosis,ducts narrow due to external compression of the metal stent graft.In these instances,radial force cannot be completely reverted by balloon dilation or implantation of plastic stents or drains,as with,for example,fibrotic stenosis.Resolution of symptomatic TIPS-induced biliary strictures was only achieved in four of the ten patients: three by liver transplantation and one by magnet-assisted endoscopic biliary-duodenal anastomosis.Of the remaining six patients,one died from colon perforation,two were lost to follow-up due to continuous abuse of alcohol,one patient remained on internal biliary drainage and another on external biliary drainage.In the last patient,the stricture became unexpectedly asymptomatic after percutaneous drainage of a liver abscess induced by stenosis.
CONCLUSlON
We present here a peculiar case of a liver transplant recipient with a unique non-anastomotic biliary stricture caused by a TIPS stent graft implanted as a treatment for a very rare post-transplant complication,hepatic sinusoidal obstruction syndrome.To our knowledge,this extraordinary case is the first to document biliary complication due to TIPS placement in a transplanted liver.In our patient,cholestatic liver injury was reverted by successful biliary drainage,resulting in preserved graft function.To date,even after a long follow-up period,the stenosis remains refractory to endoscopic treatment,with the patient dependent on repeated stent replacements.These results correspond with outcomes from previously published rare cases of TIPS-induced biliary strictures in native livers,in which complete resolution was only achieved as a result of liver transplantation or advanced endoscopic techniques.
FOOTNOTES
Author contributions:Hucl T,Peregrin J and Macinga P created the conception and design of this research;Macinga P and Hucl T wrote the paper,Gogova D and Jarosova J reviewed the literature and contributed to manuscript drafting;Raupach J performed transjugular intrahepatic portosystemic shunt placement;Janousek L performed liver transplantation and provided surgical consultations;Honsova E performed histological examination;Novotny J performed percutaneous transhepatic biliary drainage and interpreted the imaging findings;Hucl T,Spicak J,Taimr P and Peregrin J were responsible for the revision of the manuscript for important intellectual content;All authors revised the manuscript and issued final approval for the version to be submitted.
Supported byCzech Health Research Council,No.17-30281A.
lnformed consent statement:The patient provided us with consent to publish his case and all relevant imaging documentation.
Conflict-of-interest statement:The authors have no conflicts of interest to declare.
CARE Checklist(2016)statement:The authors have prepared and revised this manuscript according to the CARE Checklist(2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Czech Republic
ORClD number:Peter Macinga 0000-0003-3699-6914;Darina Gogova 0000-0003-4731-0412;Jan Raupach 0000-0002-1529-2355;Jana Jarosova 0000-0003-0010-0637;Libor Janousek 0000-0001-7572-8416;Eva Honsova 0000-0002-1625-1993;Pavel Taimr 0000-0002-2655-7603;Julius Spicak 0000-0002-3823-2881;Jiri Novotny 0000-0002-0824-8620;Jan Peregrin 0000-0001-9306-1088;Tomas Hucl 0000-0002-5648-4011.
S-Editor:Ma YJ
L-Editor:Filipodia
P-Editor:Ma YJ
 World Journal of Hepatology2022年5期
World Journal of Hepatology2022年5期
- World Journal of Hepatology的其它文章
- Role of biliary complications in chronic graft rejection after living donor liver transplantation
- Reply to "Six-minute walking test performance is associated with survival in cirrhotic patients" to the editor
- Prognostic non-invasive biomarkers for all-cause mortality in nonalcoholic fatty liver disease:A systematic review and meta-analysis
- Prospective validation to prevent symptomatic portal vein thrombosis after liver resection
- Dietary phytochemical consumption is inversely associated with liver alkaline phosphatase in Middle Eastern adults
- Angle of covered self-expandable metallic stents after placement is a risk factor for recurrent biliary obstruction