
Prophylactic fixation of the unaffected contralateral side in children with slipped capital femoral epiphysis seems favorable: A systematic review
2022-05-30 05:51:26StevenVinkRenvanStralenSophieMoermanChristiaanvanBergen
World Journal of Orthopedics 2022年5期
lNTRODUCTlON
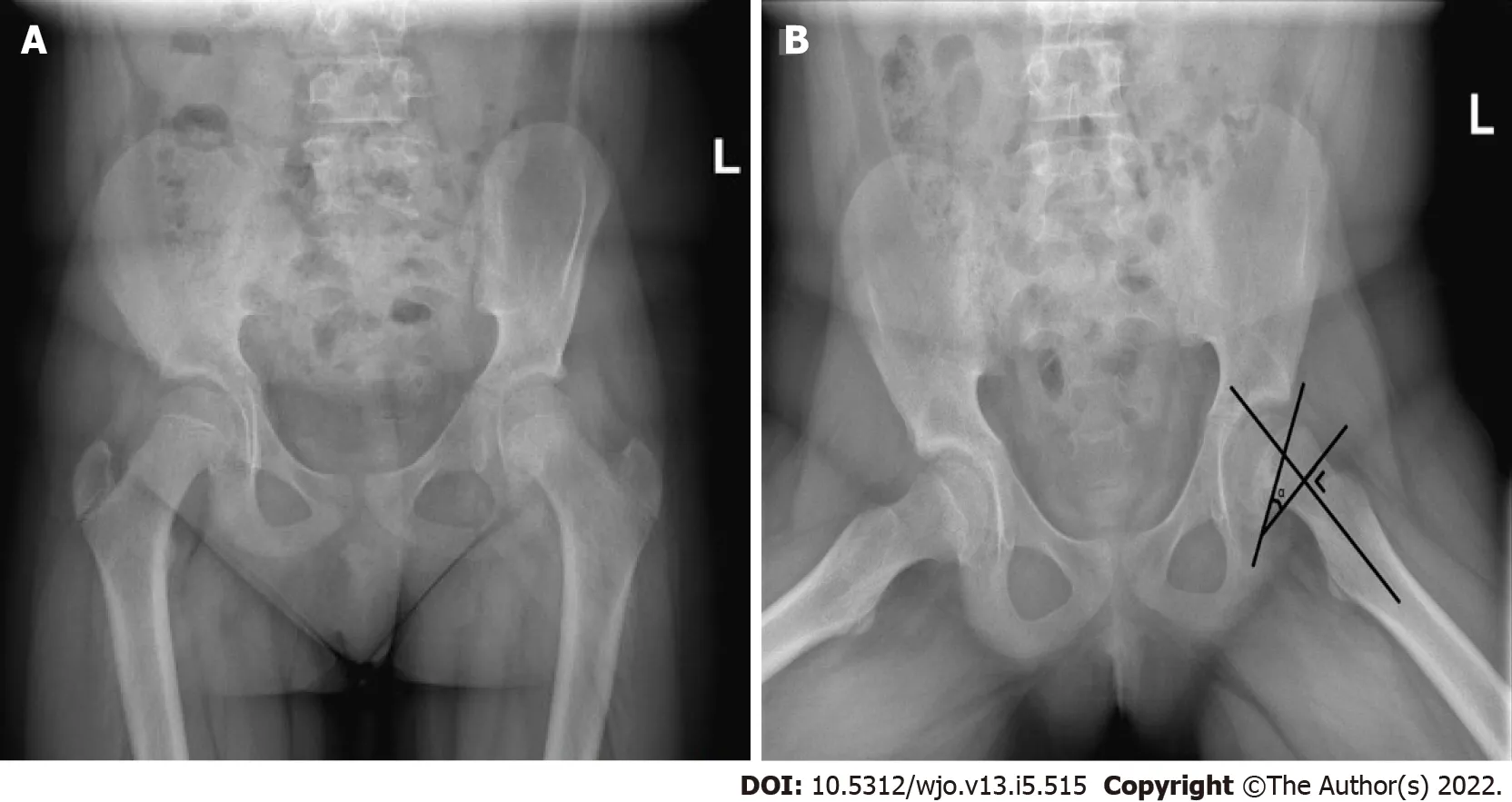
Slipped capital femoral epiphysis (SCFE) is a medical condition of the hip that occurs in adolescents.The name of this condition is in itself misleading, as it is rather the metaphysis that moves in relation to the epiphysis, while the latter remains in its position in the acetabulum. When suffering from SCFE, a patient will usually have intermittent pain in the groin area. The hip, thigh and knee may also be painful. If the slip is more severe, the patient might also present with a complete inability to bear weight on the affected leg, which is defined as unstable[1]. Furthermore, slips can be categorized according to the duration of symptoms; referred to as acute (< 3 wk of pain), chronic (≥ 3 wk) or acute-on-chronic (a traumatic event occurring in a chronic SCFE)[2]. For the diagnostic process, plain anteroposterior and frog-leg lateral hip or pelvic radiographs are generally used (Figure 1).
The overall incidence of SCFE is approximately 10.8100000 children, which differs with gender,race, and seasonal variations[3,4]. The average age of onset is reported to be 12.7 years for boys and 11.2 years for girls[4]. The cause of the slip is unknown but is thought to be multifactorial and has been related to obesity, renal failure, endocrinological disorders (, hypothyroidism, hypogonadism, or hypopituitarism) and radiation therapy[5-8]. SCFE appears to be more apparent around the time of the growth spurt and it is more common in boys than girls[5-8].
So the Prince was appointed Imperial Swineherd. He had a dirty little roomclose by the pigsty11; and there he sat the whole day, and worked. By theevening he had made a pretty little kitchen-pot. Little bells were hung allround it; and when the pot was boiling, these bells tinkled12 in the mostcharming manner, and played the old melody,
The long-term outcome of SCFE is related to the severity of the slip. This can be classified as mild(Southwick angle ≤ 29°), moderate (30°-50°), or severe (> 50°)[2]. A higher-grade slip causes decreased range of motion and higher risk of chondrolysis, avascular necrosis (AVN) of the femoral head and osteoarthritis at a later age[9]. The overall incidence of chondrolysis in SCFE patients is estimated to be 7%[10]. AVN rates vary from 7% to 21%, depending on the stability of the slip[11-13]. The etiology of AVN in SCFE patients is not fully known, but it is suggested that it is the result of a disturbance in epiphyseal blood supply and intracapsular tamponade[11]. Additionally, it has been reported that the anatomical features of a post-SCFE hip are significantly altered, even after adequate treatment, with up to 40% developing femoroacetabular impingement (FAI) and 53% developing osteoarthritis[14-16].
Percutaneousfixation is the gold standard for treatment of mild and moderate grade SCFE,whereas open reduction and internal fixation is sometimes performed for severe slips[17]. Nowadays,the most commonly used surgical method is pinning with a single screw. The screw is aimed to start from the anterior aspect of the femoral neck, in order to cross to the physis perpendicularly and enter into the central portion of the femoral head (Figure 2). In severe slips, insertion may have to be relatively oblique at the intertrochanteric region in order to prevent impingement. Another reported method is by means of double screw fixation, in which screws are inserted in a similar orientation as fixation with a single screw. In bovine femurs, this was measured to yield a 33% increase in stiffness[18]. In addition,some surgeons use Kirschner wires/pins (K-wires) rather than screws forfixation[19,20].

For years, research has been conducted on the fate of the contralateral hip, which is at an increased risk of slipping in patients with unilateral SCFE[21,22]. The exact incidence of contralateral slips is unknown, as various rates have been reported in the literature[14,23,24].
When presented with a unilateral SCFE, the attending physician has several options with regard to the contralateral side. The first is to observe the patient with regular monitoring and radiographic imaging until closure of the physis, after which the risk of developing a slip has ceased to exist. Alternatively, the surgeon may choose to prophylactically pin the contralateral side in order to prevent a potential slip. Finally, one may consider several stratifications and risk factors of the specific patient in order to estimate the risk of a contralateral slip, and decide based on this risk analysis. Recently, several risk factors have been analyzed in a systematic review and meta-analysis[25]. To this day, however, no consensus has been reached on the indication for prophylactic pinning of the contralateral side of otherwise healthy children. The present systematic review aims to provide an overall risk rate of contralateral SCFE, and a comprehensive assessment of the advantages and disadvantages that can be considered when deciding on whether or not to pin the contralateral hip of unilateral SCFE in otherwise healthy patients.
MATERlALS AND METHODS
A systematic literature search was performed on April 21, 2020, in the Embase, Medline, Web of Science Core Collection and Cochrane databases. Search terms included ‘slipped capital femoral epiphysis,’‘fixation,’ ‘contralateral,’ and derivatives thereof (Supplementary material). The searches rendered 293 unique results (Figure 3). Two authors (SV and RvS) first assessed eligibility independently by reviewing titles and abstracts, after which 89 articles remained. 73 of these were available in English and were partitioned between the four authors and again assessed independently by reviewing the full texts.Articles were considered eligible for inclusion in the current review if they reported about children with primarily unilateral SCFE that were otherwise healthy and the outcomes of prophylactically pinning the unaffected contralateral side (prevention of slip and perioperative and mid- to long-term complications), or about rates of contralateral slips and their complications. Cross-referencing led to a further inclusion of relevant publications. A total of 26 articles that specifically addressed the incidence and follow-up of contralateral SCFE were included (Table 1). The study quality of these 26 articles was then assessed independently by the authors by means of the methodological index for non-randomized studies (MINORS) criteria (Table 1, primary data available upon request)[26]. Considering the results of Loder[27] and Swarup[28], a follow-up period of 18 mo was deemed to be adequate, since a contralateral slip takes place in the first 18 mo in 88% of children[27,28]. In addition, 39 articles were found that described advantages or disadvantages of contralateral pinning.
She sprang to the door and would have run away, but on the stairs a man caught her and brought her back; and when she looked at him it was King Thrushbeard again


RESULTS
This systematic review of the literature identified 26 studies including a total of 12897 healthy patients presenting with unilateral SCFE (Table 1). The included articles report on the incidence of symptomatic contralateral slips where researchers chose not to prophylactically pin the unaffected side. In general,authors had a follow-up of at least 18 mo (mean, 46 mo) after the initial slip. When evaluating the articles eligible for inclusion in this review, the mean time after which the contralateral side slipped was 9 mo, based on 1250 slips, with a range extending to 50 mo[28]. The methodological quality of the included articles was assessed by means of the MINORS criteria for non-randomized surgical studies[26]. The methodological quality was scored at an average of 63% (Table 1).
Risk rates of contralateral SCFE and advantages of prophylactic pinning
The literature provides a substantial discussion about prophylactic fixation. Prophylactically pinning the unaffected contralateral hip has been reported to be advantageous for several reasons. It is mainly aimed at preventing the potential short- and long-term adverse effects on the development of the contralateral hip.
The incidence of a consecutive symptomatic slip on the contralateral side in SCFE patients was reported to be between 9% and 69%, with a total of 1762 patients (14%, Table 1). In addition to symptomatic slips, several authors report on the incidence of clinically asymptomatic slips. H?gglund[14] was the first in the available literature to report on the matter and noted that 104 of 237 patients(44%) presenting with unilateral SCFE had signs of an asymptomatic contralateral slip at a follow-up of 16 years to 66 years after initial presentation[14]. Since then, several other authors have reported on patients who developed asymptomatic contralateral slips, as objectified on plain radiography[29-33].The prevalence of an asymptomatic contralateral slip varied between 19% and 49%. The combined data from these and H?gglund’s reports add up to a 174 of 456 hips, a mean incidence of 38% (Table 1).
As slipping of the epiphysis causes evident negative short- and long-term outcomes, the main purpose of prophylactic pinning is to prevent the epiphysis from slipping. To assess whether this might be an appropriate measure, it is important to better understand the magnitude of the problem. Castro[2] reported that children who present with unilateral SCFE are 2335 times more likely to develop a second SCFE than the general population[2].
The little hare took it and cried, Now it is my turn to pierce them, and as he spoke he passed the rod back through the reeds and gave Big Lion s tail a sharp poke15
Evidence suggests that, despite being subclinical at adolescence, patients with asymptomatic slips are also at an increased risk of developing negative outcomes in adulthood, such as a pistol-grip deformity and cam morphology. Subsequently, such patients suffer from decreased hip function, femoral acetabular impingement syndrome, and are at an increased risk of developing early osteoarthritis[21,34-37]. Specifically, H?gglund[14] reported that 28 of the 104 patients with asymptomatic slips (27%)showed osteoarthritis of that side at a later age[14]. Jensen[30] noted that 4 of 16 patients (25%) with asymptomatic slips showed signs of osteoarthritis at follow-up, merely 22 years after the primary operation for unilateral SCFE and at an average age of 36 years[30].
In addition, Hesper[38] reviewed 39 patients that had undergone computed tomography (CT)imaging of the pelvis between 2008 and 2014 after unilateral SCFE and compared the untreated contralateral hips to those of healthy age- and sex-matched controls[38]. They recorded that the unaffected hips of SCFE patients showed decreased concavity of the head-neck junction with a higher alpha angle, as well as a reduced head-neck offset. Thus they noted a lower epiphyseal extension but a more posteriorly tilted epiphysis. These resembled a mild slip deformity and subsequent cam morphology, hence also posing an increased risk of developing early osteoarthritis.
In conclusion, prophylactically pinning may prevent 14% of children with a primarily unilateral SCFE from developing a consecutive symptomatic slip, as well as another 38% from developing an asymptomatic one. Both types of consecutive slips, as well as untreated contralateral hips that do not slip, are prone to developing disadvantageous morphological and functional outcomes at a later age.
Disadvantages of prophylactic pinning
Simultaneously, prophylactic pinning poses several potential disadvantages, which have to be weighed against the advantages.
Infection
There is a small risk of postoperative infection. O’Beirne[39] reported that after inserting a single pinan open lateral approach, 1 of 15 hips (7%) developed a deep wound infection which was resolved by removal of the pin[39]. Emery[40] mostly used three pins at a time to fixate 95 hips of which 5 (5%) developed a superficial wound infection[40]. These rates have decreased more recently.Seller[19] and Woelfle[20] noted that none of 94 and 1 of 65 (2%) patients, respectively,developed infections after fixation with three or four K-wires[19,20]. When using a single percutaneous screw fixation, the risk of infection seems very low; Kumm[41] (0 of 34), Dewnany and Radford[36][1 of 65 (2%)], Sankar[42] (0 of 99) and Bhattacharjee[43] [1 of 44 (2%)] all report low rates of wound infections[36,41-43].
AVN and chondrolysis
AVN of the femoral head, although infrequent, is another risk of surgical fixation. Even though prophylactic fixation aims to prevent slip and thereby also AVN, this complication may also develop after the procedure itself. In retrospective studies, Sankar[42] reported that AVN developed in 2 of 99 patients (2%), whereas none of the 26 and 24 prophylactically pinned hips reviewed by Seller[44]and Cousins[45], respectively, developed AVN[42,44,45]. Herngren[37] reported no cases of AVN in the prophylactically treated group of their prospective cohort study[37]. Other studies report no cases of AVN[19,20,36,39-43]. Chondrolysis was also not seen by any of the referenced authors.
Implant-related problems
Peri-implant fractures may occur shortly or at a later stage after surgery. These are usually subtrochanteric fractures starting around the entrance site of the screw. Sankar[42] reported that 2 of their patients (2%) developed peri-implant fractures[42]. They suggested that there is a higher fracture rate if the screw enters distal to the level of the lesser trochanter or medial to the intertrochanteric line. Likewise, Herngren[37] noted 2 peri-implant fractures (1%) in their prospective study[37].
Some authors argue that the surgical procedure increases the risk of the development of dysmorphology of the prophylactically pinned hip in the long term, with functional limitations as a result. Lerch[46]performed a follow-up study of 33 prophylactically pinned hips after an average of 12 years[46].Although noting no intra- or postoperative complications, they did find radiographic evidence of cam morphology in 10 patients (30%), of whom four (12%) developed FAI syndrome as a result and required additional surgery. No patient had developed radiographic signs of osteoarthritis by then. Dodds[16] reported that 4 out of 7 prophylactically pinned hips (57%) developed a pistol grip deformity,though none of these patients experienced FAI syndrome[16]. These findings were recently supported by Kulkarni[47], who reported femoral head asphericity in 37% of their patients, rendering them at risk of developing FAI syndrome[47]. The question remains whether the secondary deformities are caused by the surgery or by the natural history of these hips.
Growth alteration and morphologic changes
Several authors also report on the displacement, migration and loss of fixation of the hardware,especially with use of non-threaded pins and wires. Emery[40] reported that at the time of radiological fusion of the epiphyseal plate, the femoral head had grown off of as much as 29% of their Crawford Adams pins[40]. As such, the pins did not cross the epiphyseal plate anymore and thus only penetrated the femoral neck and trochanteric area of the shaft, rendering them useless. Additionally, in 17% of the cases of both Seller[19] and Woelfle[20], a reoperation was necessary because the Kwires did not catch the epiphysis anymore due to the physiological growth of the proximal femur,especially when it concerned very young patients[19,20].
Perhaps you will serve me for another year yet, said the troll, and you will get six bushels of money for it; that m&kes twelve in all, and that is a pretty penny
A similar concern of pinning the unaffected hip is the possibility of premature closure of the physis.Cousins[45] compared the articulo-trochanteric distance (ATD), the trochanteric-trochanteric distance (TTD), and the neck length shortly after surgery and on average 20 mo thereafter between 24 prophylactically pinned hips and 26 observed unaffected hips[45]. The difference in TTD:ATD ratio proved to be significant, suggesting that pinning resulted in a coxa breva and relative coxa vara. It was suggested that these morphological alterations could lead to FAI syndrome and therewith osteoarthritis.Moreover, the neck length was significantly higher at follow-up in the observed group, thereby concluding that the pinned group showed less residual growth. The mean difference in final leg length between the SCFE side and the prophylactically pinned hip has been reported to be 5.7 millimeters, with a maximum of 1 centimeter[19,44]. The residual growth might be dependent on the type of fixation;W?lfle-Roos[48] reported that the residual growth was a mean of 4.4 millimeters more when using three or four K-wires, as compared to a single screw[48]. Considering the primary SCFE side, one may argue that a reduced residual growth after pinning the contralateral side is actually an advantage. The primary SCFE side also shows less residual growth as compared to healthy hips, therefore the difference in final leg length will thus decrease as compared to children who have not undergone prophylactic pinning.
Risk factors
Numerous studies have aimed to identify risk factors for developing sequential contralateral involvement in unilateral SCFE patients. Swarup[25] performed a comprehensive systematic review and meta-analysis of potential risk factors[25]. The most significant demographic factors that were reported to be associated with a contralateral slip were a body mass index (BMI) greater than the 95percentile and a younger age at presentation. Clinically, a shorter duration of symptoms before the actual first slip was also reported to be a risk factor. When evaluating the anteroposterior and frog-leg lateral hip or pelvis radiographs, several suggested risk factors can be assessed including the posterior sloping angle (PSA, Figure 1), alpha angle and modified Oxford score (a measure for skeletal maturity)[25,49]. In the included studies of the meta-analysis, conflicting results were reported in regard to the slip angle, with studies showing an increased risk of contralateral slip when a lower angle was found, while other researchers reported the risk to be increased when a higher angle was present[25].The alpha angle of the primary SCFE was reported to be a weak but significant prognostic factor.Patients with a mean angle of 51 degrees were at a higher risk of developing contralateral SCFE compared to a mean angle of 45 degrees. The PSA of the healthy side was reported to be significantly higher in patients that developed a subsequent contralateral slip. A mean of 16 degrees was related to a higher risk of subsequent slip compared to a mean of 12 degrees. According to the meta-analysis by Swarup[25], a younger age at the time of the first slip (mean difference, -0.9 years) and a higher PSA(mean difference, 4.7 degrees) remained independent significant risk factors. For other factors, such as sex, BMI, endocrine abnormality, slip stability and modified Oxford score, no significant differences were identified in the meta-analysis.
Several researchers have specifically studied additional imaging modalities to further evaluate the risk of a contralateral slip in order to detect early evidence of morphologic changes preceding symptomatic and asymptomatic slips. Balch Samora[50] assessed the use of focal or diffuse physeal widening, abnormal signal and bone marrow edema adjacent to the physis on magnetic resonance imaging (MRI) in predicting contralateral SCFE[50]. Eleven of 33 enrolled patients developed a contralateral SCFE. Overall, the sensitivity of the MRI predictors was reported to be 80%, specificity 92.9%, positive predictive value 66.7% and negative predictive value 96.3%, with an interrater reliability of 100%. In addition, Futami[51] evaluated unilateral SCFE cases and their unaffected counterparts with MRI[51]. They scanned 10 patients for a total of 33 times. In all SCFE cases, physeal widening was observed. In 4 of the 10 patients, the unaffected side showed physeal widening without a slip. Lesions were observed in the physis which were similar to lesions in the affected hips. These were then prophylactically pinned. Neither these, nor the other observed hips that did not show physeal widening,slipped during a mean follow-up time of 36 mo. Nevertheless, the authors suggested that the physeal widening, clearly visible on MRI, may reduce epiphyseal stability and requires prophylactic pinning.Wensaas[52] also reported on MRI scans of 22 primarily unilateral SCFEs[52]. They measured the MRI slip angle, greatest focal widening of the physis, global widening of the physis measured at three locations, periphyseal bone marrow edema, the presence of pathological joint effusion and the amount of joint effusion measured from the lateral edge of the greater trochanter. These parameters were significantly altered in primarily affected hips. However, they could not discern a significant difference between the 6 hips of patients who did and the remainder who did not develop contralateral SCFE.
I prayed for your health and your happiness, and for your ability to be supplied with the tools necessary to complete your task as teacher and educator and mentor16
DlSCUSSlON
They were almost up to him when he dashed into a very narrow cleft24 in the rock, much too small for them to follow; but in his hurry he had left one of his long ears sticking out, which they just managed to seize
A robe, he said, scanning the aisles until he caught sight of her hair, a dark green shoulder, her bent27 head revealing the elegant pale curve of her neck
At this the witch became so furious that she danced about and knocked everything to pieces that she could lay her hands upon, so that the splinters flew about the ears of the prince and princess, who now stood there in her own beautiful shape
When surgical fixation is considered, a decision with regard to the surgical technique needs to be made. K-wires as a method of fixation, may cause that the wires unintentionally migrated within the femur mostly due to physiologic growth of the proximal femur[19,20,40,53]. However, this migration rarely led to epiphysiolysis or other symptoms such as pain. Nonetheless, it can be argued that this migration does pose additional risks. On the other hand, fixation with threaded screws has a higher impact on the residual growth of the femur. One might argue that the reduced residual growth of the unaffected side can be considered an advantage, as the difference in leg length between the unaffected and affected sides at follow-up is decreased when the unaffected side is pinned as well[42]. Recently,researchers have also tested a new type of free-gliding screw, which is intended to allow growth of the physis and thereby decrease the influence of fixation on the final leg length. The first results of biomechanical studies have been reported and appear to be promising[54]. Thus, some of the possible negative effects of pinning on growth could be overcome within the foreseeable future for either side.
This article aims to provide a comprehensive review and summary of the scientific evidence regarding the prevalence of contralateral SCFE and fixation in otherwise healthy patients with unilateral SCFE.According to the reviewed data, prophylactic fixation of the contralateral side would prevent 14% of patients from developing sequential symptomatic contralateral involvement. Another 38% of asymptomatic slips may also be prevented. Because prevention of a contralateral slip may drastically reduce the possible negative outcomes, such as osteoarthritis in the long term, these rates may outweigh the small risk of complications due to the additional surgery. However, multiple patient, surgical and radiographic factors should be taken into account in the shared-decision process with the patients and their parents. The most important risk factors of a subsequent contralateral SCFE are a younger age at the time of presentation and a higher PSA on plain radiography[25].
Opponents of prophylactic fixation argue that the patient is exposed to the risk of iatrogenic injury to an otherwise healthy hip[55]. Indeed, some of the associated complications such as AVN and chondrolysis are serious. However, they are minor in incidence, with only 0%-2% of cases developing AVN and no cases of chondrolysis reported at all in the presently reviewed literature. Other reported complications include anatomic changes such as cam morphology. However, various studies have shown that the ‘unaffected’ side often has dysmorphic features without having been operated on, as visualized on CT and MRI[34,50-52]. This finding questions whether the morphologic changes are a result of the surgical procedure or rather a result of the natural course of these hips.
After a little time a second snake crept out of the corner, but when it saw the first one lying dead and in pieces it went back and came again soon, holding three green leaves in its mouth
On the other hand, fixation of the contralateral side also involves risks. However, surgical complications occur only incidentally and the clinical implications of secondary morphologic changes as a result of surgical intervention remain unclear. Hence, the disadvantages appear to be relatively infrequent and insignificant as compared to the possible advantages that can be achieved through fixation.Nonetheless, both perspectives should be taken into consideration, and the choice as to whether or not to pin the unaffected side should remain a patient-tailored one.
The present review has some limitations. Although the literature was searched systematically, there might be additional relevant research in the literature that would add to our data. Methodological quality of the included studies was quantified, but showed that the research conducted did not meet all of the MINORS criteria, averaging at 63% of the total applicable score. In addition, few authors reported about the severity of the contralateral slips that developed after initial unilateral involvement.Therefore, no definitive conclusions could be drawn as to the distribution of mild, moderate and severe contralateral slips. Additional data on the distribution of severity within this population may prove more insightful in whether the risks of surgery outweigh the possible complications related to (severe)slips. However, with our search terms, we have sought to include a representative and comprehensive amount of data on the basis of which we present the considerations and conclusions.
CONCLUSlON
That night the boss came home to his 14-year-old son and sat him down. He said, The most incredible thing happened to me today. I was in my office and one of the junior executives came in and told me he admired me and gave me a blue ribbon for being a creative genius. Imagine. He thinks I m a creative genius. Then he put this blue ribbon that says Who I Am Makes A Difference on my jacket above my heart. He gave me an extra ribbon and asked me to find somebody else to honor. As I was driving home tonight, I started thinking about whom I would honor with this ribbon and I thought about you. I want to honor you.
In an attempt to be able to make a more protocolized decision, researchers have developed different decision analysis models. However, the outcomes of their respective research are contradictory. Kocher[55] described an expected-value decision analysis on the indication for strategy-prophylacticpinningobservation[55]. According to their systematic review, the expected value of prophylactic pinning remained lower than for observation. They therefore concluded that careful observation is the better strategy unless the probability of a contralateral slip exceeds 27%. In contrast, Schultz[56]concluded in a different model that prophylactic pinning of the contralateral hip is, in general, favorable for long-term outcomes[56]. Taking these conclusions to heart, the discussion on the indication for prophylactic fixation is still open, and careful education of patients and meticulous clinical and radiographic follow-up could provide an alternative to prophylactic pinning. However, one might argue that prophylactic pinning of the hip saves the time and trouble of an intensive follow-up process until physeal closure with the associated necessary additional radiographic imaging.
ARTlCLE HlGHLlGHTS
Research background
Slipped capital femoral epiphysis (SCFE) is an important medical condition occurring in adolescents. It may cause severe short and long term complications. At present, there is no clear consensus on whether or not to prophylactically fixate the unaffected side in unilateral SCFE. The current review provides a comprehensive assessment of the deliberations to be made when treating this condition.
Research motivation
The risks of subsequent contralateral slipping after primary unilateral SCFE are discussed. Consequently, the advantages, but also the risks, rendered by prophylactic fixation are outlined.
The contralateral hip in otherwise healthy patients presenting with a unilateral symptomatic SCFE remains a controversial subject. Literature suggests that a substantial rate of these patients are at risk of developing a subsequent slip of the contralateral side or in fact simultaneously have an asymptomatic slip. Such slips consequently may lead to morphologic changes, decreased hip function and early osteoarthritis. Fixation of the contralateral hip may thus prevent these negative long-term outcomes.
Research objectives
The risk rates of subsequent contralateral slipping and its sequelae after primary unilateral SCFE are evaluated. Several imaging modalities and their interpretation in regard to the risk assessment are presented. The advantages and disadvantages of prophylactic pinning are evaluated and an overall outline is presented as to the treatment strategy.
Research methods
A systematic review of the literature was performed and the results were presented in a qualitative manner with descriptive statistics.
Research results
When presenting with unilateral SCFE, a patient has a 2335 times increased likelihood of developing a consecutive contralateral slip, with 14% developing a symptomatic and 38% asymptomatic slip. Both clinical and subclinical slips are at an increased risk of developing harmful sequelae of the hip. Prophylactic pinning of the contralateral side negates the development of such sequelae. This surgical intervention renders complications such as infection, avascular necrosis, implant related problems and morphologic changes, albeit only at very low rates. A number of methods to assess the risk of a contralateral slip have been described in the current literature, most significantly the posterior sloping angle (PSA) on plain radiographs.
Research conclusions
A substantial rate of patients presenting with unilateral SCFE develop a contralateral slip, posing an increased risk to developing harmful sequelae. The advantages of negating these developments by prophylactic pinning of the primarily unaffected side appear to be outweighing the infrequently occurring disadvantages of the surgical intervention. The decision remains to be patient-tailored and can be aided by evaluation of the PSA on plain radiographs.
Research perspectives
Additional studies evaluating a watchful waiting strategy that elaborate on the severity of subsequent slips and its sequelae may prove insightful to better weigh this against the surgery associated risks. In addition, further research directly comparing the short and long term outcomes of watchful waiting and prophylactic pinning may aid in formulating an unambiguous treatment strategy. Also, research concerning the risks for developing a primary SCFE may further the prevention of the condition arising in the first place in the adolescent population, thereby improving their long term functioning.
ACKNOWLEDGEMENTS
The authors wish to thank Wichor Bramer from the Erasmus Medical Centre Medical Library for developing the search strategies.
FOOTNOTES
Vink SJC drafted and finalized the manuscript; van Stralen RA and Moerman S contributed to the data collection; van Bergen CJA supervised the writing process; All authors contributed to the inclusion and assessment of the study quality of eligible articles, reviewed and commented on the text and approved the final version.
The authors declare no conflict of interests for this article. This study did not receive funding.
The authors have read the PRISMA 2009 Checklist, and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
He bought a nice, big fat cat and let him stay there. The cat had a nice time hunting the mice and killing1 them. The mice could not move freely now. They were afraid that anytime the cat would eat them up.
Netherlands
Steven J C Vink 0000-0001-8775-3010; Renée A van Stralen 0000-0002-8390-8051; Sophie Moerman 0000-0001-5766-6709; Christiaan J A van Bergen 0000-0001-8336-9070.
Fan JR
I had worked in prisons for too many years to be fooled by his shyness. I knew that many of the inmates10 had learned at a very young age that they could do nothing right. They had been abused and tormented11 as children and lacked any self-confidence. But no matter how much I praised the other prisoners he wouldn’t relent. He went back to his dormitory that evening with his writing tucked into his jeans pocket. Many of the other men just left their work on the desks. Not him. He was taking no chance that I would read it after he was locked away behind the bars. He was right, of course. 1 would have made a beeline right for his desk the minute he got out the door. He had judged me right.
Filipodia
Fan JR
 World Journal of Orthopedics2022年5期
World Journal of Orthopedics2022年5期
- World Journal of Orthopedics的其它文章
- Extensive adhesion formation in a total knee replacement in the setting of a gastrointestinal stromal tumor: A case report
- lntramedullary bone pedestal formation contributing to femoral shaft fracture nonunion: A case report and review of the literature
- Prosthetic joint infection of the hip and knee due to Mycobacterium species: A systematic review
- Effect of non-steroidal anti-inflammatory drugs on fracture healing in children: A systematic review
- Anterior vertebral body tethering for idiopathic scoliosis in growing children: A systematic review
- What factors are important to new patients when selecting an orthopedic oncologist?