
Effects of a remote,YouTube-delivered exercise intervention on young adults’physical activity,sedentary behavior,and sleep during the COVID-19 pandemic:Randomized controlled trial
2022-04-18 11:32:04DnielMcDonoughMelinHelgesonWenxiLiuZnGo
Dniel J.McDonough *,Melin A.Helgeson ,Wenxi Liu Zn Go
a School of Kinesiology,University of Minnesota-Twin Cities,Minneapolis,MN 55455,USA
b Carlson School of Management,University of Minnesota-Twin Cities,Minneapolis,MN 55455,USA
Abstract
Keywords:High-intensity interval training;Resistance-training;Self-determination theory;Social media;Video
1.Introduction
To optimize health,the World Health Organization recommends adults engage in a minimum of 150 min per week of moderate-to-vigorous physical activity(MVPA)and at least 2 days per week of muscle-strengthening physical activities(PAs)targeting all major muscle groups.1However,recent population-level surveillance data indicate that over 80%of U.S.adults fail to meet the minimum recommendations for aerobic and muscle-strengthening PAs.2This pandemic of physical inactivity3,4has become a major public health challenge,given that physical inactivity greatly increases the risk of developing non-communicable diseases and premature mortality5and that physical inactivity-related morbidities now account for approximately 85%of total health care costs in the United States annually.4Additionally,high levels of physical inactivity have been observed to adversely affect individuals’sleep quality6(i.e.,sleep duration and efficiency7),which contributes to the incidence of hypokinetic diseases8and all-cause mortality9and further burdens the economy indirectly by decreasing daytime productivity.10
With the outbreak of the coronavirus disease 2019(COVID-19)pandemic and the enacted regulations to reduce its transmission(e.g.,physical distancing,gym and recreation center closures,home quarantine11-14),we are currently facing an infectious disease pandemic that has compounded the preexisting physical inactivity pandemic.3,15While all demographics have been affected by these regulations,U.S.young adults in particular have been forced to make extraordinary changes to their lifestyle and behavioral patterns,16which has created exceptional barriers to their PA participation and has further exacerbated the issue of poor sleep quality in this population.16,17Further,with the home environment emerging as the only viable indoor opportunity for PA,the inaccessibility of commercial exercise equipment has decreased young adults’autonomous motivation to engage in PAs.18Accordingly,the American College of Sports Medicine has released a call to action for health professionals to develop novel and flexible approaches to PA that account for these unprecedented circumstances.19Thus,there is an urgent need to develop innovative and enjoyable home-based PA promotion interventions that minimize human contact,are cost-effective,and have a wide reach in order to help mitigate the compounding effects of the COVID-19 pandemic on physical inactivity and poor sleep quality among U.S.young adults.
One PA promotion intervention strategy that fulfills the preceding criteria is delivery by social media.Indeed,over 90%of U.S.young adults use online social media regularly20and have demonstrated high interest in receiving health-related information on these platforms,thereby widening access to health behavior change interventions in this population.21Further,social media platforms are cost-effective methods of increasing user interaction and providing peer-to-peer support,21which may be especially beneficial to young adults during the COVID-19 pandemic considering their increased levels of anxiety and depression during this time.16Thus,it stands to reason that social media would be an effective medium by which to disseminate a home-based PA intervention during the COVID-19 pandemic,especially among young adults who are the primary consumers.20However,a meta-analysis of randomized controlled trials(RCTs)observed social media-based health behavior change interventions to be ineffective in promoting PA in this population.22Notably,the PA interventions included in this analysis were delivered via Facebook groups,Twitter,or custom websites with social components(e.g.,forums)—textbased platforms wherein participants were instructed to read PA-related information and apply it in their daily lives.However,eye-tracking studies23,24have indicated that text-based media consumption on the Internet is primarily nonlinear(i.e.,time is primarily spent browsing,keyword spotting,and/or scanning),thereby limiting information processing and the likelihood that participants will put the provided information into action.Further,global consumer Internet video traffic now accounts for over 80% of all consumer Internet traffic,25and Internet-based video consumption is on track to surpass television for consuming video-based content,26demonstrating a recent shift in preferred media consumption.Indeed,unlike text,online videos minimize the cognitive effort required to process information,27thereby leading to improved comprehension,and have shown to be more engaging than content-identical,text-delivered content.27,28That said,it is not surprising that YouTube—a video-based social media platform—is now the most used social media platform and is regularly used by over 94%of U.S.young adults.29,30Therefore,the use of video-based social media platforms like YouTube to disseminate a remote,home-based PA promotion intervention warrants investigation.
Interestingly,despite the preceding statistics demonstrating the preference for,and benefits of,Internet-based video consumption over content-identical,text-based media consumption,the research empirically examining its utility for disseminating remote PA interventions is scant.Limited pilot trials28,31,32with small sample sizes have demonstrated Internet-based,video-delivered PA content to be more effective than text-delivered content for promoting PA in adults.However,these trials were underpowered and were further limited by self-reported PA measures and short intervention durations.Interestingly,a large-scale RCT33that addressed the preceding limitations found that Internet-delivered PA videos were not more effective than content-identical PA information delivered via text for increasing adults’MVPA.However,this trial had notable limitations,which we believe hindered the effectiveness of utilizing video to increase individuals’PA levels:(1)Attrition was very high(49%at 12 weeks)primarily from loss of intervention interest—likely due to low frequency of video dissemination(only 8 videos were disseminated over 12 weeks);(2)Too many behavior change theories were used when meta-analyses34,35have shown multi-theory-based interventions to be less effective for PA behavior change compared to single-theory-based interventions;(3)Content within the videos was not guided by empirically-based content analyses and principles of health-based video quality;36and(4)Example footage(i.e.,“B-roll”)—one of the inherent benefits of using remotely-disseminated video—was not optimally utilized to demonstrate on-screen aerobic and muscle-strengthening PAs that participants could follow along to,thereby missing the opportunity to promote physical literacy,which is a major barrier to PA in young adults,37,38especially with the recent confinement to the home without access to familiar exercise equipment.
Taken together,in response to the preceding COVID-19-related barriers to young adults’PA participation and the resulting decrease in autonomous motivation for engaging in homebased PA,16-18a timely health behavior change intervention should aim to promote more intrinsically-regulated forms of PA motivation among this population.Thus,given the seamless integration of health behavior change theory in social media-based PA interventions,39,40the intervention should be grounded in a behavior change theory that fosters more internally-regulated forms of motivation for PA.Self-determination theory(SDT)is a widely-used health behavior change theory that has demonstrated effectiveness for improving young adults’intrinsic motivation for PA and exercise.41Briefly,SDT postulates that by fulfilling 3 basic human psychological needs—competency(i.e.,experience of mastery and effectiveness),autonomy(i.e.,experience of willingness and volition),and relatedness(i.e.,experience of connecting to others)—one’s motivation will progress along a continuum to more internally-regulated forms ranging from amotivation(i.e.,no motivation)to extrinsic motivation and then to intrinsic motivation,which helps foster long-term PA adherence.41
Therefore,this study’s purpose was to examine the effects of a remote,home-based,YouTube video-delivered aerobic and muscle-strengthening PA intervention grounded in SDT as compared to a YouTube video-delivered general health education control intervention on young adults’free-living MVPA(primary outcome)and sedentary behavior(SB),light PA(LPA),muscle-strengthening PA frequency,self-determined PA motivation,and perceived PA barriers(secondary outcomes).We hypothesized a priori that,compared to the control group,intervention participants would significantly improve their daily MVPA,SB,and LPA levels,muscle-strengthening PA frequency,intrinsic PA motivation,and perceived PA barriers after 12 weeks.Findings from this study may better inform clinicians and other health professionals of the utility of Internet-based video platforms to disseminate PA promotion interventions suitable for improving young adults’aerobic and muscle-strengthening PA and sleep quality at scale to help attenuate the compounding effects of the COVID-19 pandemic on the preexisting pandemic of physical inactivity.
2.Materials and methods
We followed the CONSORT guidelines42(Supplementary Table 1)while drafting this manuscript.Further,this study was approved by the University of Minnesota Institutional Review Board(STUDY00010444)in November 2020,and we registered the trial with ClinicalTrials.gov(NCT04499547).All study questionnaires were distributed to participants using Qualtrics(Qualtrics;Provo,UT,USA)—an online survey software.Notably,for all survey questions within this software,we applied the“force response”function to ensure a 100%survey response and completion rate.
2.1.Study design and sample
We employed a prospective,12-week,parallel RCT wherein participants were randomized(1:1)into either the experimental group(received weekly YouTube video-delivered aerobic and muscle-strengthening PA videos grounded in SDT)or the control group(received weekly YouTube video-delivered general health education videos with no PArelated content).In detail,64 participants from the University of Minnesota took part during Fall 2020-Winter 2021,and all participants started the study concurrently.Given national COVID-19-related campus closures,we only recruited participants via email communications,using various university email servers to sample from a variety of disciplines.We included participants who were between the ages of 18 years and 35 years,were enrolled or employed at/by the study university,had a body mass index(BMI)≥18.5 kg/m2,had PA levels below national recommendations1over the last month(verified by questionnaire),possessed no self-reported diagnosed physical/mental disability and had no contraindications to PA participation(assessed by the PA Readiness Questionnaire),had Internet access and a device capable of accessing YouTube,and were willing to be randomized into either study group.Participants were excluded from participation if they were younger than 18 years or older than 35 years,had a BMI<18.5 kg/m2,met or were above the PA recommendations over the last month,answered“yes”to at least 1 question on the PA Readiness Questionnaire,did not have access to the Internet and/or YouTube,or were not willing to be randomized into either study group.We obtained Institutional Review Board approval from the University of Minnesota and written informed consent(digitally signed)from participants prior to recruitment and data collection.Further,all participantinvolved procedures were performed in accordance with the ethical standards of the institution and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.43Participants were paid USD30 for successful study completion.
2.2.Procedures
Interested participants were instructed to respond directly to the recruitment email,after which the project manager(MAH)responded with an email link containing the online consent form and questionnaires to determine whether they met the preceding inclusion criteria.Participants who qualified were emailed another link containing a battery of online baseline surveys to obtain demographic information and assess psychosocial and other self-reported study outcomes.The same psychosocial and self-report questionnaires were re-distributed at 12 weeks for post-intervention assessments.Additionally,at baseline and 12 weeks,participants who qualified for the study were mailed an ActiGraph accelerometer GT9X+(ActiGraph,LLC.,Pensacola,FL,USA)with an adjustable wrist strap,the associated wear instructions,and a sleep log;they were also provided a self-addressed stamped envelope to return the accelerometer and sleep log after the 7-day wear periods.Notably,the wear log was only utilized as a wear-compliance strategy,given that our analysis of raw accelerometer data did not require sleep log input.All accelerometers were disinfected based on World Health Organization guidelines44as well as study university policies before being distributed to participants.Accelerometers were mailed back by participants in the supplied envelopes with pre-paid postage,and the returned accelerometers were left untouched(i.e.,quarantined)for≥14 days to rid them of any potential COVID-19 contamination.44
Following the 7-day baseline testing period,the project manager(MAH)informed participants of their group allocation.To preserve participants’privacy and to blind the study investigators(DJM,WL,and ZG)to participants’group allocation,participants were instructed by the project manager(MAH)to create a new YouTube account that was linked to their university email under a pseudo username(i.e.,a creative username other than their given name)so they could not be identified(e.g.,“YouTube Study Participant 2021”).Participants were then instructed to subscribe to the YouTube channel for their respective study group and turn on upload notifications by clicking the“bell”icon.Turning on upload notifications was used as an intervention adherence strategy as it ensured that participants would be immediately notified via email when each video was uploaded to the study channel.As a part of our intervention fidelity protocol,participants were encouraged to contact the project manager(MAH)with questions and were also contacted every 3 weeks during the study with standardized emails encouraging continued intervention adherence.Lastly,to prevent intervention contamination,we asked participants to refrain from sharing their group allocation and/or content from their group videos with friends/peers who were enrolled in the study.
2.3.Interventions
We used YouTube as the delivery vehicle for our intervention videos to maximize ecological validity as our formative testing among young adults at the study university revealed this platform to be the primary place of consumption for Internet-based video,which is consistent with statistics demonstrating YouTube to be the top social media platform both globally and in the United States,particularly among young adults(used by 94%).30Additionally,social media platforms like YouTube are cost-effective methods of increasing user interaction and providing peer-to-peer support16,21through interactions in the“comments section”of the videos,which our formative testing revealed to be an enjoyable intervention component.
We conducted formative testing in the Spring and Fall of 2020 among young adults around the university by distributing surveys and conducting small focus groups to help identify preferred PA-based video content(e.g.,preferred video lengths and upload frequencies,preferred PA-and SB-related content,workout interests,etc.).Based on our findings,to achieve high intervention adherence and make the study videos enjoyable for both groups,we adhered to the American Medical Association’s video quality guidelines45for video and sound recording and best practices for video editing(e.g.,utilizing“jump-cuts”for conciseness).Also based on feedback from our formative testing,we utilized“A-roll”(i.e.,primary footage of the main subject(MAH)wherein the main content was taught interview-style)and overlaid the A-roll footage during post-production editing with“B-roll”(i.e.,supplemental video footage)to visually demonstrate what was being talked about and show how to properly execute the information in order to facilitate participants’physical literacy.36To further increase video quality and participants’comprehension of the intervention content,during post-production editing we overlaid our video footage with text using dynamic motion graphics titles,relevant stock images and video footage(Shutterstock.com;Shutterstock,New York,NY,USA),copyright-free music,and utilized multiple camera angles to demonstrate the proper biomechanics of the exhibited exercises.To track intervention adherence(i.e.,watching all study videos in their entirety),we instructed both groups to reply to “in-video response questions”(embedded randomly within the videos)within the comments section of each video.We also tracked adherence using watch-time metrics provided by YouTube’s Creator Analytics and informed participants that if we deemed video adherence too low,they may be removed from the study.Lastly, to improve ecological validity and facilitate SDT-related social support,we encouraged participants to interact with one another and to provide feedback on their replies to the response questions within the comments section of each video.
2.3.1.Experimental intervention
In addition to our formative testing,our videos were informed by an empirically-based content analysis36examining the best practices for disseminating PA and SB information via video(e.g.,emphasis should be placed more on increasing PA rather than reducing SB).Moreover,given research demonstrating young adults’decreased autonomous motivation for engaging in home-based PAs,18the intervention group videos were grounded in SDT.41We demonstrated SDT and how we grounded our intervention group videos in SDT in Fig.1.
The intervention group received 1 YouTube video per week(duration=6.3±3.9 min,mean±SD)and were asked not to consume other PA-related YouTube videos during the duration of the 12-week intervention.In detail,the videos contained SB-related content(e.g.,the negative effects of prolonged SB and different strategies for how to break up daily SB),PA-related content(e.g.,taught participants the aerobic and muscle-strengthening PA guidelines1and various strategies to increase their daily MVPA and muscle-strengthening PAs),and/or home-based aerobic and muscle-strengthening workouts that participants could follow along to on-screen.Regarding the home-based workout videos,in the absence of commercial gym equipment,high-intensity interval training has been observed as a feasible and effective option for home-based aerobic PA with limited space.46Briefly,we leveraged pre-recorded video and edited in on-screen countdown timers(green timers indicated work intervals and red timers indicated rest intervals),so participants could follow along and workout during the video and we added in up-tempo music during the workout intervals to increase enjoyment and workout intensity.Likewise,muscle-strengthening exercise(e.g.,resistance-training)could effectively be achieved in the home setting using one’s own bodyweight and by manipulating various resistance-training variables(e.g.,focusing on eccentric muscle actions,shortening between-set rest intervals,etc).46Additionally,because the muscle-strengthening exercises were more difficult to follow along to on-screen(identified during formative testing),we demonstrated all exercises within each video and created high-quality PDF files(e.g.,Supplementary Figs.1 and 2)containing written versions of the workouts and then linked them directly under the YouTube videos so participants could download and readily access them any time they wanted to re-visit the workouts,ideally helping them to meet the weekly muscle-strengthening PA guideline.Lastly,given only 1 video per week was uploaded,we encouraged participants to re-visit the previous study videos and PDF workout files and to perform the provided workouts multiple times per week to further increase MVPA and muscle-strengthening PA levels.Full access to the control group’s videos was provided after successful completion of the 12-week intervention.

Fig.1.Self-determination theory-grounded intervention videos.
2.3.2.Control condition
The control group also received 1 video per week during the 12-week intervention and participants were asked not to consume other health-related YouTube videos during the 12-week intervention.In detail,these videos were delivered on the same days/times as the intervention group videos but contained no PA-related content.Rather,the video content within the control group covered a variety of general health education topics relevant to young adults(e.g.,nutrition,anxiety,mental health).As an additional incentive for intervention fidelity in the control group,full access to the intervention group’s videos was provided after successful completion of the 12-week intervention.
2.4.Outcomes
We conducted the following tests to measure free-living MVPA(primary outcome)and sleep quality,adherence to the muscle-strengthening PA guidelines,SDT-related motivation,and perceived PA barriers(secondary outcomes).All study outcomes were determined a priori.
2.4.1.Baseline demographics and anthropometric measures
We used the online survey software to collect participants’self-reported demographic information(e.g.,age,sex,previous YouTube use/experience,COVID-19-related effects on their PA levels,etc.)using a variety of response types(e.g.,multiple-choice,short answer).Full demographic information for our sample by study group is provided in Table 1.Given the fully remote nature of our study,baseline anthropometric measures(e.g.,height(cm),weight(kg))were also self-reported,and BMI was calculated as weight(kg)/height(m2).These data were collected at baseline and analyzed descriptively to characterize our sample.
2.4.2.Free-living PA,SB,and sleep quality
We measured daily minutes in MVPA,LPA,SB,and sleep quality using the wrist-worn ActiGraph Link GT9X accelerometer(ActiGraph)—a small(3.5×3.5×100 mm),lightweight(14 g)device that captures one’s movement along the 3 orthogonal axes.We instructed participants to snugly and comfortably fit the accelerometers on the wrist of their non-dominant arm using the provided strap and to remove any other health wearable device(s)for the duration of the wear periods.47To allow for the collection of PA and sleep data,we asked participants to wear the accelerometer all day and night for a period of 7 days with the only exception being during activities of prolonged deep-water submersion(e.g.,swimming).Data were sampled at a frequency of 30 Hz,and we turned the screens off to disable PA-related feedback and prevent performance bias.We defined sleep quality as sleep duration(i.e.,total true sleep time)and sleep efficiency(i.e.,the ratio of time sleeping divided by total time in bed).7We considered accelerometer data valid if the device was worn for at least 4 days,including at least 1 weekend day,and for at least 16 h each day.48
We processed the raw accelerometer data into 5-s epochs using the R Studio-package GGIR(Version 1.2.1335)49in R Version 4.0.4(the R Foundation,Vienna,Austria).Briefly,GGIR calculates PA intensities and detects non-wear time by converting all raw acceleration values into a single omnidirectional acceleration value.Specifically,the raw accelerometer data were auto-calibrated and converted into gravity-corrected vector magnitude units called Euclidian norm minus one with negative values set to zero.For valid wear days,we calculated PA intensities(i.e.,MVPA,LPA,SB)based on previously established cut-points in milligravity(mg)for Euclidian norm minus one with negative values set to zero values:SB(0-56.2 mg),LPA(56.3-191.6 mg),and MVPA(>191.6 mg).50For detection of participants’sleep quality,we used GGIR to estimate change(s)in arm angle relative to the horizontal plane while sleeping,with a change in arm angle of<5°over a 5-min period considered as a possible sleep period.51We calculated the following sleep variables:sleep duration(h/night)and sleep efficiency(total sleep time(h)/time in bed(h)×100%).Mean values for PA,SB,and sleep quality outcomes were calculated at baseline and 12 weeks.

Table 1 Baseline group comparisons(self-reported).
2.4.3.Muscle-strengthening PA frequency
We assessed muscle-strengthening PA frequency using an item from the Behavioral Risk Factor Surveillance System survey—a valid and reliable self-report assessment of adults’habitual participation in muscle-strengthening PAs.52The full script for this item has been published elsewhere.53Notably,participants reported their muscle-strengthening PA frequency as times per week or per month.For those who reported times per month,we divided this number by 4 to provide estimates of weekly muscle-strengthening PA frequency.52Further,we a priori decided to truncate weekly frequency of musclestrengthening PA at 14 times/week to limit the possibility of unrealistic responses.53Mean changes in days/week of muscle-strengthening PA were used as the study outcome and were measured at baseline and 12 weeks.
2.4.4.SDT-related motivation
Participants’SDT-related PA motivation was evaluated using the 24-item Behavioral Regulation in Exercise Questionnaire-3(BREQ-3)survey54—a version of the BREQ-2 survey that is amended to include an assessment for integrated regulation,which has demonstrated good validity and reliability for measuring self-determined motivation for PA in U.S.young adults.Briefly,the BREQ-3 survey is used to quantify the continuum of behavioral regulation types in PA applications by evaluating 3 levels of motivation,progressing from amotivation to extrinsic motivation and then to intrinsic motivation,with 6 subscales progressing along this continuum:(1)non-regulation;(2)external regulation;(3)introjected regulation;(4)identified regulation;(5)integrated regulation;and(6)intrinsic regulation.55In detail,using a 5-point Likert-type scale(1=not true for me;5=always true for me),the BREQ-3 required participants to determine how true different statements were,such as“I don’t see why I should have to exercise”(for non-regulation),and“I exercise because it’s fun”(for intrinsic regulation).We used the mean score for each of the 6 subscales as the outcome,with higher scores indicating a greater regulation type.Participants’SDT-related motivation was assessed at baseline and 12 weeks.Internal consistency(Cronbach’sα)for this measure was good among our sample(α=0.84).56
2.4.5.Perceived PA barriers
Participants’perceived PA barriers were evaluated using the 14-item Perceived Barriers Scale,which has demonstrated good reliability and validity among adults.57In detail,this scale required participants to rate the agreement between their own perceived PA barriers and hypothetical PA barriers using a 4-point Likert-type scale(1=strongly disagree;4=strongly agree)for statements such as“Physical activity takes too much of my time”and“There are too few places to be physically active”.Mean scores were used as the study outcome,with higher scores indicating greater perceived barriers to PA.Participants’perceived PA barriers were assessed at baseline and 12 weeks.Internal consistency for this measure was good among our sample(α=0.81).56
2.5.Sample size calculation,randomization,and blinding
We used G*Power(G*Power;Brunsb¨uttel,Germany)to determine the necessary sample size for this study based on changes in free-living MVPA,which was our primary study outcome.Based on average(small)effect sizes for changes in young adults’MVPA(d=0.30)according to previous social media-delivered PA promotion interventions of the same duration,22,58it was estimated that 60 participants(30 per group)were necessary to detect a significant between-group difference and give 80%power with a two-sided significance level of 0.05.Assuming 15%attrition,our goal was to enroll 69 participants.No interim analysis was planned.
Randomization,participant enrollment,and group allocation were completed by our project manager(MAH),who was blinded to the study questions and outcomes.Specifically,our random allocation sequence was completed using the“randomize”package in R Studio with no block restrictions applied.Given the use of pseudo usernames within the intervention YouTube channels to preserve participants’privacy,all other investigators were blinded to participants’group allocation;the blinding was not broken until the primary and secondary analyses were completed.
2.6.Statistical analysis

3.Results
3.1.Participant flow through the trial
Participant flow through the trial is shown in Fig.2.Briefly,84 young adults expressed interest and were screened for study participation,64 of whom were deemed eligible(reasons for ineligibility at each stage of recruitment are shown in Fig.2).Thus,64 participants completed baseline testing and randomization.Retention was 96.9%in the experimental group and 93.8%in the comparison group.One experimental group participant dropped out for reasons unrelated to the study(illness)and 2 dropouts from the control group were due to loss of contact and illness.
3.2.Baseline participant characteristics
Descriptive statistics for participants’baseline characteristics by group are shown in Table 1.We observed no clinically meaningful baseline differences between groups for participant demographics and therefore determined our randomization procedures to be robust.Accordingly,we did not perform any covariate analyses.Additionally,we determined dropouts’baseline data were not materially different from completers’baseline data and,thus,proceeded with the planned imputation procedures.Overall,the sample was healthy(XBMI=23.1 kg/m2),100%used YouTube prior to the study,and the primary device used for consuming YouTube was a smart phone(78.1%).Notably,56.2%of participants reported using YouTube very often(i.e.,daily),34.4%reported often(i.e.,a few times per week),7.8%reported sometimes(i.e.,a few times per month),and 1.6%reported rarely(i.e.,a few times per year).The primary recruitment strategy was email(90.6%),followed by word of mouth.Lastly,62.5%and 68.8%of intervention and control participants,respectively,reported that COVID-19 had made them“l(fā)ess active”,9.4%and 12.5%reported“more active”,and 28.1%and 18.7%reported“no difference”.
3.3.Primary outcome
3.4.Secondary outcomes
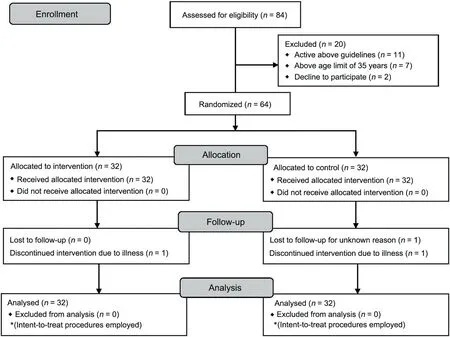
Fig.2.CONSORT flow diagram.

3.5.Adverse events
No adverse events related to the intervention were reported in either study group during the study.However,1 participant dropped out mid-intervention due to contracting COVID-19.
4.Discussion
Our study examined the effectiveness of a home-based,YouTube video-delivered PA promotion intervention grounded in SDT for improving young adults’free-living aerobic and muscle-strengthening PA,SB,sleep quality,SDT-related PA motivation,and perceived PA barriers.We observed statistically significant improvements in free-living MVPA,muscle-strengthening PA frequency,sleep efficiency,SDT-related PA motivation,and perceived PA barriers after 12 weeks in the intervention group.We observed no statistically significant interaction effects for LPA,SB,or sleep duration after 12 weeks,and we observed no statistically significant main effects for time for any outcome in the control group.
Congruent with our hypothesis,participants in the intervention group significantly improved their free-living MVPA after 12 weeks.We believe the intervention group’s post-intervention increases in MVPA were a result of their more internallyregulated motivational states(e.g.,significantly decreased non-regulation and increased integrated and intrinsic regulation)as well as their significantly decreased perceived PA barriers.Regarding SDT-related motivation,as postulated by SDT,41we methodically embedded video components that aimed to progress participants’motivational states from less to more internally-regulated forms by targeting this group’s 3 basic psychological needs:(1)competence(e.g.,videos taught participants the risks of high SB and low PA levels and the benefits of achieving the PA guidelines with B-roll visually demonstrating how to achieve these guidelines);(2)autonomy(e.g.,videos used B-roll to visually demonstrate more and less intense exercise varieties to allow participants to choose which version to perform based on their level of physical fitness);and(3)relatedness(e.g.,videos overlaid the A-roll with B-roll that visually demonstrated partner exercises,thereby encouraging participants to perform these exercises/workouts with a friend or family member who they felt safe to exercise around).Given that young adults have been observed to be less intrinsically motivated to perform PA in the home setting without commercial exercise equipment,46we purport that SDT’s well-documented ability to improve habitual PA behaviors60facilitated the observed changes in MVPA among the intervention group.Notably,although not statisticallysignificant at the adjusted significance level,SB decreased by an average of 30 min per day in the intervention group after 12 weeks,which we believe is practically significant.Because we observed significant changes in MVPA but no significant changes in LPA,we believe that intervention participants replaced some of their SB time with MVPA,shifts which both have clinically meaningful implications independent of one another.1Additionally,we leveraged our videos to create prerecorded high-intensity interval training workouts focusing on full-body exercises that participants could seamlessly follow along to on-screen and perform with the study investigators.Indeed,high-intensity interval training requires maximal or near-maximal effort and has demonstrated effectiveness in an RCT61to improve adults’cardiorespiratory fitness in only 4 weeks.Therefore,we believe performing these workouts weekly greatly contributed to the increased MVPA levels among the intervention group.
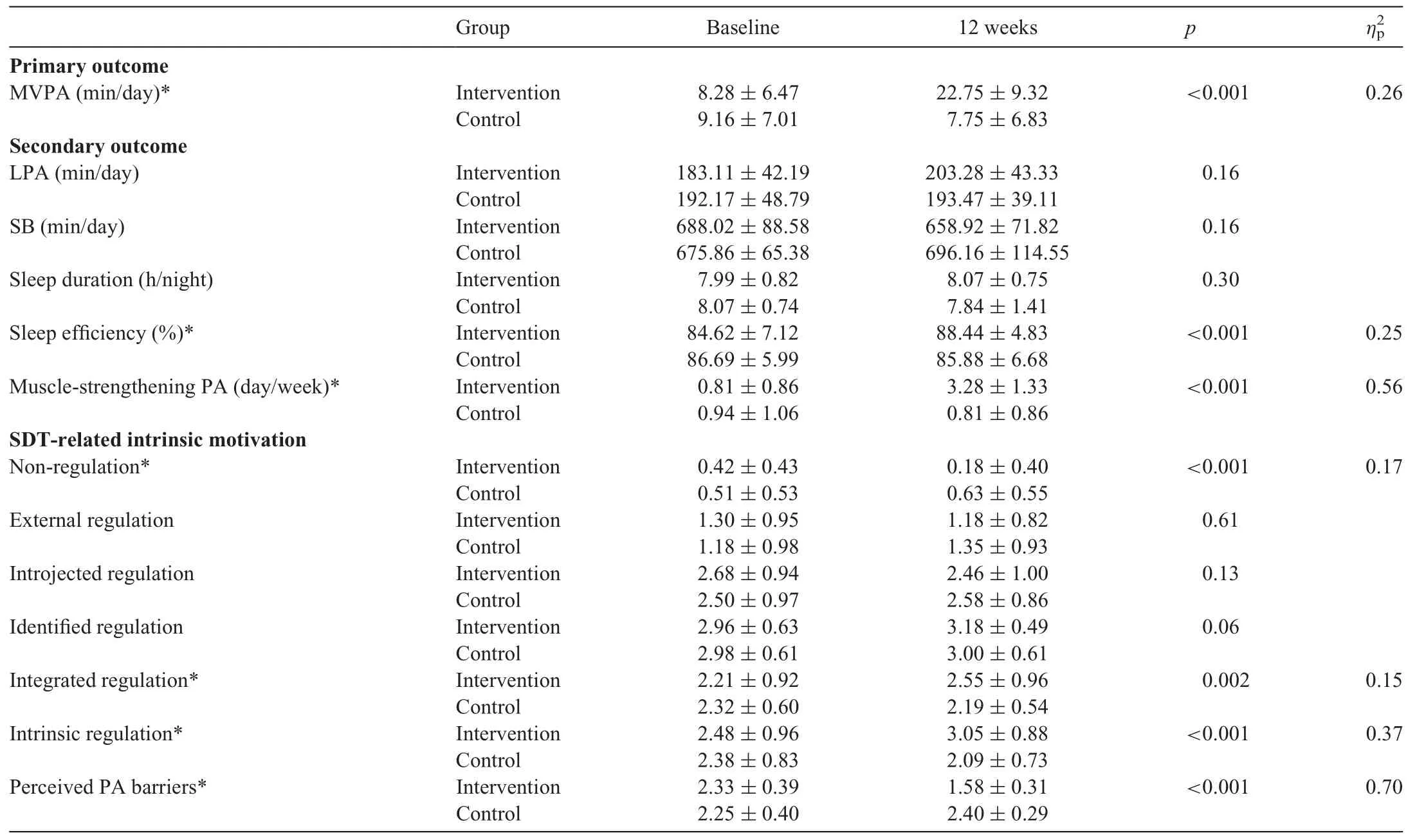
Table 2 Primary and secondary outcomes by groups at baseline and 12 weeks.
Likewise,we observed that participants in the intervention group significantly improved their muscle-strengthening PA frequency after 12 weeks,whereas those in the control group demonstrated no changes in this outcome.Notably,participants in the intervention group increased their average muscle-strengthening PA frequency from less than 1 day per week(i.e.,below the recommended guideline of≥2 days per week)to over 3 days per week(i.e.,exceeding the recommended guideline).Again,we believe the use of video,and particularly B-roll within the intervention videos,helped improve participants’physical literacy—a major barrier to muscle-strengthening PA in this population.37,38,62Also contributing to improved physical literacy was the videos’use of different camera angles and exercise variations based on one’s muscular fitness level,which allowed participants to see how to properly perform these exercises.Being confined to the home during the COVID-19 pandemic without familiar commercial exercise equipment not only affects autonomous motivation to engage in muscle-strengthening activities like resistance-training,46but was likely also a perceived musclestrengthening PA barrier.However,assuming exercise intensity is near-maximal,one’s own bodyweight is sufficient to induce favorable musculoskeletal adaptations(e.g.,muscular strength and hypertrophy).63,64Therefore,our muscle-strengthening-oriented videos promoted various methods of enhancing resistancetraining workout intensity like adding general household items to exercises to increase the working load(e.g.,wearing a loaded backpack during squats to train the legs,holding filled laundry soap containers to perform lateral raises for the shoulders)and introducing various resistance-training techniques like eccentricfocused training,wherein the emphasis is placed on muscle lengthening(or eccentric muscle actions)for longer periods of time.Moreover,not only did we teach the intervention participants the muscle-strengthening recommendations and provide on-screen demonstrations of full-body resistance-training workouts employing various training techniques to increase workout intensity,but we also encouraged participants to perform these activities multiple times per week and provided them with highquality PDF files with the written workouts so they could download and readily access them when they planned to perform the resistance-training workout(s)later in the week.Thus,in the absence of commercial gym equipment in the home setting,prerecorded YouTube videos that teach the muscle-strengthening PA guidelines and demonstrate exercises and workouts using the above strategies could effectively improve muscle-strengthening PA participation,which has a myriad of physical and mental health benefits independent of aerobic PA participation,65,66including improved depressive symptoms,67which may be especially important for young adults during the COVID-19 pandemic.16
Also in line with our hypotheses,only the intervention participants significantly improved their sleep efficiency despite no changes in either group for total sleep duration.The observed increases in sleep efficiency were likely attributed to the observed decreases in this group’s SB and increases in aerobic and musclestrengthening PA levels.These findings are consistent with other findings among young adults demonstrating that there is an inverse relationship between SB and sleep efficiency.68Likewise,a growing body of research has demonstrated that increased PA levels improve adults’sleep quality.Thus,the concurrent decreases in SB and increases in PA among the intervention group—especially that of moderate-and vigorous-intensities—lead to significantly improved sleep efficiency.Interestingly,despite the preceding improvements in sleep efficiency among the intervention group,we observed no differences in sleep duration in either group.Also to our surprise,average sleep duration in both groups was high(about 8 h/night)despite research demonstrating poor sleep behaviors among this population during the pandemic.16,17We believe that because the majority of our sample were college students,the winter break—and therefore lack of school responsibilities—was responsible for the high sleep durations in both groups.Nevertheless,the ability for participants in the intervention group to fall asleep faster and,thus,get more quality sleep,may have great public health implications7regarding their physical health,8,9as well as daytime productivity and being able to contribute to society.10Therefore,the use of video to deliver remote,home-based PA,SB,and aerobic and musclestrengthening information/workouts not only directly improves participants’PA behaviors but also indirectly affects individuals’sleep quality,both of which have major public health implications during the COVID-19 pandemic and beyond.
Our study had several strengths.First,our sufficiently-powered RCT allowed us to examine causal relationships between the independent and dependent outcome variables between homogonous groups of young adults.Second,we employed device-based measurements for our primary PA and sleep quality outcomes as well as valid and reliable questionnaires for our muscle-strengthening PA and psychosocial outcomes.Lastly,our intervention videos were based on formative assessments among young adults,an empirically-based content analysis and principles of health videos,36and were grounded in a single behavior change theory(SDT),which has been observed to be more effective for PA behavior change than multi-theory interventions.34,35However,despite the preceding strengths,our study had some limitations that must be addressed.
First,we employed a self-reported muscle-strengthening PA assessment,which may have been prone to response bias.Nevertheless,this item has demonstrated good validity and reliability among adults and is currently the only viable option for this assessment given objective,device-based assessments for muscle-strengthening PA are not available.Second,we were unable to employ long-term follow-up assessments and examine the long-term effectiveness of this intervention.Third,in an effort to maximize ecological validity(i.e.,have participants consume the intervention YouTube videos as they would in the real world),internal validity may have been compromised insofar as we did not directly assess intervention adherence.Fourth,given our sample was primarily female,this may have influenced the results to some degree and,therefore,future studies should aim to recruit an equal distribution of male and female participants.Lastly,our study was conducted in the middle of the COVID-19 pandemic wherein participants were facing enacted regulations to reduce the transmission of COVID-19(e.g.,home quarantine)and,thus,it remains unknown if this intervention will effectively improve PA behaviors during the post-pandemic era with lifted restrictions(e.g.,no home confinement,access to commercial fitness centers).Similarly,given these special circumstances,participants may have had more time on their hands than usual,and it remains unknown if the observed results would be replicated during pre-pandemic conditions.Likewise,our intervention was conducted in the state of Minnesota during the winter season wherein temperatures are consistently freezing.Participants in both groups may have been more motivated to engage in outdoor PA during the warmer spring/summer months.Thus,post-pandemic research should employ similar interventions in warmer climate regions and/or during warmer seasons and with longer follow-up periods and more representative samples.
5.Conclusion
Our findings indicated that a remote,home-based,YouTube video-delivered PA intervention grounded in SDT significantly improved young adults’free-living MVPA,muscle-strengthening PA,and sleep efficiency,which was likely a result of the intervention’s positive effects on participants’self-determined motivation for PA and decreased perceived barriers to PA.Thus,with COVID-19 still prevalent in the United States and with uncertainty regarding young adults’preferred PA behaviors and environments in the post-pandemic era,remote,home-based interventions utilizing SDT-grounded,prerecorded videos demonstrating PA promotion,SB reduction,and aerobic and muscle-strengthening exercise routines have emerged as an effective intervention strategy for reducing PA barriers and facilitating more autonomous forms of PA motivation to help combat the compounding effects of the COVID-19 pandemic on the preexisting pandemic of PA and poor sleep quality in the United States.
Also noteworthy is that these interventions are cost-effective for both researchers(e.g.,content can be filmed using a smart phone and uploaded for free to YouTube)and participants(e.g.,YouTube content is free to consume)and have mass-reach capabilities.Indeed,additional video-based PA platforms like You-Tube are rapidly emerging,including Apple’s“Apple Fitness+”and video-delivered exercise routines through commercial gyms.Therefore,we encourage qualified health professionals to utilize these findings and remotely disseminate video-based PA interventions using high-traffic video platforms like YouTube.
Acknowledgments
This study was funded by DJM’s Doctoral Dissertation Fellowship through the University of Minnesota as well as DJM’s Professional Development Grant through the University of Minnesota’s School of Kinesiology.
Authors’contributions
DJM conceived the study idea,conducted statistical analyses,drafted the manuscript,and created/edited the study videos;MAH was the subject for all talking-head(“A-roll”)video clips for the intervention and control groups,performed randomization and group allocation,created content for the general health education control group,and oversaw all other managerial tasks;WL facilitated the analyses for raw PA and sleep data and edited and revised the manuscript;ZG helped conceive the study idea,edited and revised the manuscript,and provided the accelerometers.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary material associated with this article can be found in the online version at doi:10.1016/j.jshs.2021.07.009.
 Journal of Sport and Health Science2022年2期
Journal of Sport and Health Science2022年2期
- Journal of Sport and Health Science的其它文章
- Exercise is medicine for type 2 diabetes:An interview with Dr.Sheri R.Colberg
- Application of e-health programs in physical activity and health promotion
- Exercise cardiac power and the risk of heart failure in men:A population-based follow-up study
- A physically active lifestyle is related to a lower level of skin autofluorescence in a large population with chronic-disease(LifeLines cohort)
- Movement behaviors and their association with depressive symptoms in Brazilian adolescents:A cross-sectional study
- Bidirectional relationships of physical activity and gross motor skills before and after summer break:Application of a cross-lagged panel model