
Colorectal cancer screening and surveillance in patients with inflammatory bowel disease in 2021
2022-03-16 06:25:44JoseMariaHuguetLuisFerrerBarcel6PatriciaSuarezEvaSanchezJoseDavidPrietoVictorGarciaJavierSempere
Jose Maria Huguet, Luis Ferrer-Barcel6 , Patricia Suarez,Eva Sanchez, Jose David Prieto, Victor Garcia,JavierSempere
Abstract The detection of dysplasia in patients with inflammatory bowel disease (IBD)continues to be important given the increased risk of colorectal cancer in this population. Therefore, in 2017 , we performed a review and update of the recommendations for the management and follow-up of patients with IBD based on the clinical practice guidelines of various scientific societies. The present manuscript focuses on new aspects of the detection, follow-up, and management of dysplasia according to the latest studies and recommendations. While chromoendoscopy with targeted biopsy continues to be the technique of choice for the screening and detection of dysplasia in IBD, the associated difficulties mean that it is now being compared with other techniques (virtual chromoendoscopy), which yield similar results with less technical difficulties. Furthermore,the emergence of new endoscopy techniques that are still being researched but seem promising (e.g., confocal laser endomicroscopy and full-spectrum endoscopy), together with the development of devices that improve endoscopic visualization (e.g., Endocuff Vision), lead us to believe that these approaches can revolutionize the screening and follow-up of dysplasia in patients with IBD.Nevertheless, further studies are warranted to define the optimal follow-up strategy in this patient population.
Key Words: Colitis surveillance; Colitis screening; Chromoendoscopy; Colorectal cancer;Inflammatory bowel disease; Ulcerative colitis
INTRODUCTION
The worldwide consensus among scientific societies is that screening for colorectal cancer (CRC) in patients with inflammatory bowel disease (IBD)[1 -5 ] should be carried out by means of colonoscopy, preferably during the remission phase and with appropriate bowel preparation[6 -10 ]. The objective is to detect potentially resectable premalignant lesions (dysplasia) and CRC in the early stages, thus improving prognosis[11 -15 ]. While CRC-related mortality has decreased since the introduction of endoscopic screening techniques[16 -19 ], the risk of CRC remains unchanged[20 ].
The differences in the recommendations of scientific societies on screening and surveillance in affected patients led us to review and update the recommendations of the various scientific societies and research groups in 2017 [21 ]. Nevertheless, novel aspects and updates that have appeared since then are worthy of review, even though research in some areas remains incomplete.
SUMMARY OF OUR RECOMMENDATIONS
Below is a summary of our previously published recommendations
To whom should CRC screening be offered?Screening for CRC should be offered to the following patients affected by IBD: patients with ulcerative colitis (UC), regardless of its extent; patients with Crohn’s disease (CD) affecting at least one-third of the colon or accompanied by complex perianal disease; patients with an ileoanal pouch; and patients with indeterminate or unclassified colitis. Endoscopy should be performed preferably in periods of clinical-biological remission and should enable an estimation of the individual risk of CRC, as well as the extent of the disease[21 ].
When should the first colonoscopy screening be performed?The first colonoscopy screening should be offered eight years after a diagnosis of CD or UC. In patients with primary sclerosing cholangitis (PSC), colonoscopy should be performed as soon as possible. In patients with an ileoanal pouch, colonoscopy should be performed one year after the surgical intervention. Patients with first-degree relatives who were diagnosed with CRC before age 50 should be offered the first endoscopy ten years before the age the family member was when affected by CRC or eight years after a diagnosis of IBD (whichever occurs earlier).
Who should be offered endoscopic surveillance?After screening, all patients should undergo endoscopy-based follow-up, except for those with ulcerative proctitis, CD with the involvement of less than one-third of the colon, and those in whom the risks outweigh the possible benefits.
Should the same endoscopic surveillance intervals be followed for all patients?No.We recommend that patients be stratified according to their individual risk.
Are there individual risk factors that allow us to stratify endoscopic surveillance?
Yes. Among patients with left-sided UC or pancolitis and CD affecting at least onethird of the colon, high-risk patients are defined as those having any of the following:PSC, extensive involvement, moderate-severe active inflammation sustained over time(endoscopic or histological), a first-degree relative with CRC before age 50 , or stenosis or dysplasia detected during the previous five years. Intermediate-risk patients are defined as those having any of the following: extensive colitis with mild or moderate sustained active inflammation (endoscopic or histological), inflammatory polyps, or a first-degree relative with CRC after age 50 . A diagnosis of IBD at a young age should be taken into account as a relative risk factor (due to the long duration of the disease).Factors other than high- and intermediate-risk factors should be considered low-risk factors. High-risk factors in patients with an ileoanal pouch are as follows: dysplasia or previous CRC, PSC, and type C mucosa in the pouch (persistent atrophy and severe inflammation) (Table 1 ).
How long should the endoscopic follow-up intervals be?Endoscopic follow-up intervals are recommended as follows: for patients with IBD, according to the presence of risk factors for each patient; for patients with high-risk factors, annual colonoscopy;for patients with intermediate-risk factors, colonoscopy every three years; for patients with low-risk factors or no other risk factors, colonoscopy every five years; for patients with an ileoanal pouch, according to the presence of risk factors; for patients with risk factors, annual colonoscopy; and for patients with no risk factors, colonoscopy every five years (Table 1 ).
What is the recommended endoscopic technique for screening and surveillance?
Chromoendoscopy with endoscopic resection or biopsies aimed at visible lesions is the technique of choice. If this is not possible, high-definition video colonoscopy should be used, and four biopsies should be taken every ten cm of the colon.
How is chromoendoscopy performed?Methylene blue (0 .04 %-0 .1 %) or indigo carmine (0 .1 %-0 .03 %) is used. Caecal intubation is performed, and a dye is applied to the mucosa of the colon as the endoscope is removed, if possible, using a catheter spray. One segment should be examined before applying a dye to the next segment.
Does the occurrence of dysplasia require confirmation?The occurrence of dysplasia must be confirmed by a second pathologist.
What terminology should be used to describe lesions detected with endoscopy?The terms “dysplasia-associated lesion or mass (DALM)” and “flat lesions” should be discontinued. The modified Paris Classification, in which lesions are divided into visible dysplasia and invisible dysplasia depending on whether the biopsy has been taken from a lesion visualized in the colonoscopy or not, should be used. Visible dysplasia is divided into polypoid and non-polypoid depending on whether the lesion protrudes from the lumen ≥ 2 .5 mm. The descriptions of visible lesions should also include a mention of whether they are ulcerated and whether the borders are easily distinguished from the surrounding mucosa (Table 2 ).
How should a visible lesion be managed?Visible lesions that are well delimited, with no evidence of dysplasia in the mucosa adjacent to the lesion and no synchronous dysplasia, should be resected endoscopically regardless of the degree of dysplasia.
How should invisible dysplasia be initially managed?Dysplasia that is not endoscopically visible but found in serial biopsies of the colon must be confirmed by an independent pathologist after chromoendoscopy is performed by an expert endoscopist. If dysplasia is confirmed, management will depend on the degree.
How should invisible dysplasia be managed in relation to the degree of dysplasia?
Endoscopically invisible high-grade dysplasia is an indication for colectomy. The management of low-grade, invisible dysplasia should be agreed upon in a multidisciplinary committee and with the patient: the two possible options are colectomy and endoscopic follow-up.
How should endoscopically resected lesions be followed?The follow-up for resected lesions in healthy mucosa not affected by colitis should be the same as that for sporadic adenomas. Lesions that are endoscopically resected in areas affected by colitis should be examined endoscopically at three months and annually thereafter.
NOVEL ASPECTS IN SCREENING AND FOLLOW-UP
The most recent updates to clinical practice guidelines[22 -24 ] do not contain substantial modifications with respect to candidates for screening, the periodicity ofscreening, or risk factors for CRC in these patients. Similarly, no novel aspects in this regard have been published in recent reviews[25 ]. While neither new research nor changes in current knowledge are expected in this field, it is worth taking into account the observation made by Burkeet al[26 ], who concluded that patients with IBD and high-risk factors should be closely followed up at short intervals. These authors performed a retrospective review of interval CRC associated with IBD and not associated with IBD diagnosed between January 2007 and December 2014 in a largescale American health system. When they compared cases of interval CRC associated and not associated with IBD, they found that associated cases were more common in younger patients (54 .5 vs 70 .4 years; P < 0 .001 ); these had appeared within a shorter interval after the index colonoscopy (20 .7 vs 35 .1 mo; P = 0 .09 ). An evaluation of adherence to American Society for Gastrointestinal Endoscopy guidelines revealed that 53 % (8 /15 ) of cases of interval CRC in patients with IBD were detected in line with surveillance guidelines. All of the patients with interval CRC detected after the surveillance period recommended in the guidelines had high-risk factors during the index colonoscopy, namely, active inflammation, multiple pseudopolyps, previous low-grade or indefinite dysplasia, or a family history (first-degree) of CRC[26 ].

Table 1 Risk factors for the development of colorectal cancer in patients with inflammatory bowel disease and recommended surveillance
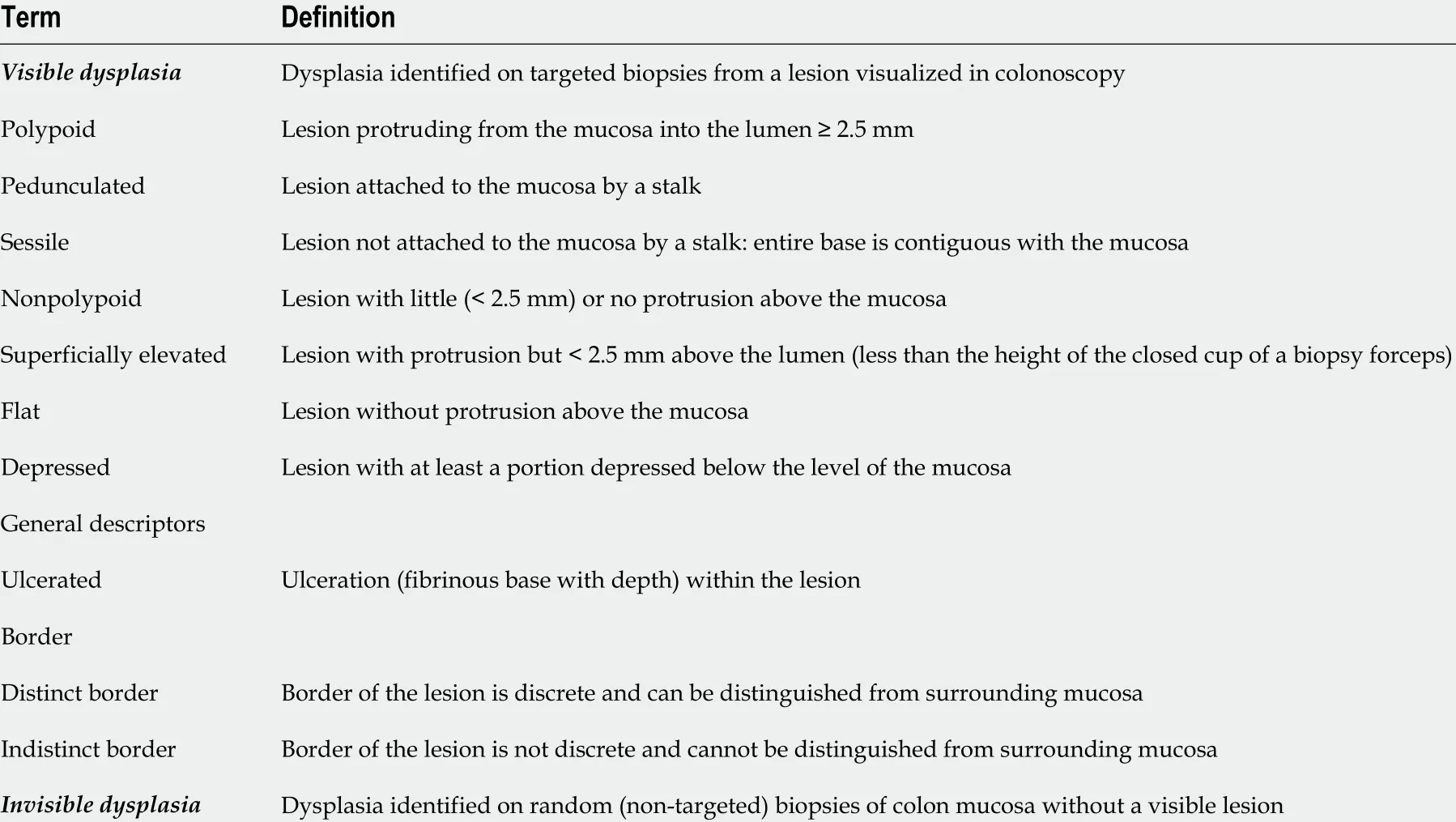
Table 2 SCENIC international consensus
A recent study analysed 9398 pouchoscopy procedures performed in 3672 patients and concluded that the low incidence rate for neoplasm recorded suggests that pouchoscopy was not routinely necessary in asymptomatic patients, in patients with a history of primary sclerosing cholangitis, or in patients with chronic pouchitis,although it is recommended when there is a personal or family history of CRC. More evidence is necessary before guidelines can be changed[27 ].
NOVEL ASPECTS OF THE RECOMMENDED ENDOSCOPIC TECHNIQUE
Up to the time of our review[21 ], there was a general consensus on using chromoendoscopy with methylene blue or indigo carmine as the technique of choice, mainly since the publication of the SCENIC CONSENSUS[28 ]. In situations where chromoendoscopy was not possible, the technique of choice was high-definition video colonoscopy and serial biopsies every ten cm of the colon. New subsequent guidelines maintained this recommendation[29 ], and real-life studies supported the decision[30 ].
However, the recommendation soon began to be called into question, and the new ACG guidelines stated the following:When using high-definition colonoscopes in patients with UC undergoing surveillance, we suggest white-light endoscopy with narrow-band imaging or dye-spray chromoendoscopy with methylene blue or indigo carmine to identify dysplasia (conditional recommendation, low quality of evidence)[23 ]. Furthermore, the difficulties arising with chromoendoscopy were reviewed by our group and included a long examination time, the need for optimal bowel preparation, specialist training,and higher costs[31 ]. These difficulties could have led to chromoendoscopy being performed less frequently than desired, despite recommendations from scientific societies on the application of the technique. Such were the findings of a recent online survey administered to academic gastroenterologists belonging to the Canadian Association of Gastroenterology, which revealed low uptake of chromoendoscopy as a surveillance tool for dysplasia in patients with IBD. The main barriers reported were the long duration of the procedure, cost, and the lack of experience or training in the technique[32 ].
The situation was recently evaluated by Bisschopset al[33 ], who performed a multicentre prospective randomized controlled trial of 131 patients with UC and found that chromoendoscopy and virtual chromoendoscopy (VCE) with narrow-band imaging (NBI) presented no significant differences for the detection of dysplasia or neoplasms associated with UC. Furthermore, the authors concluded that, given the reduced withdrawal time and greater ease of use, VCE with NBI should replace traditional chromoendoscopy. Clarkeet alperformed a retrospective analysis of cases and controls in which they concluded that there were no statistically significant differences in the detection of dysplasia using dye-spray chromoendoscopy compared with high-definition white-light colonoscopy, although the chromoendoscopy procedure took longer[34 ]. Gulati et al[35 ] performed a multifaceted randomized crossover trial to evaluate study feasibility and obtain preliminary comparative procedural and patient experience data. The authors found that the diagnostic accuracy of VCE was higher, although the differences were not statistically significant[93 .7 % (85 .5 %-98 .2 %) vs 76 .9 % (66 .9 %-85 .1 %) for chromoendoscopy]. In addition, the authors found that biopsy based on VCE was less frequent, with fewer dysplastic lesions overlooked than with chromoendoscopy and a failure rate of 9 .1 %, compared with 18 .2 % for chromoendoscopy. Patients generally reported a significant preference for VCE; most had a high risk of cancer requiring more intense and frequent surveillance. While the reasons for this preference were not explored, the authors suggest that it could be because the technique is less time-consuming than chromoendoscopy and there is no need for contrast or abdominal distension.
A study of 270 patients compared three different techniques for surveillance colonoscopy to detect colonic neoplastic lesions in IBD patients: high-definition,chromoendoscopy, and VCE using i-SCAN image-enhanced colonoscopy[36 ]. A randomized noninferiority trial was conducted to determine the detection rates of neoplastic lesions in IBD patients with longstanding colitis. The authors concluded that neither VCE nor high-definition colonoscopy was inferior to dye-spray colonoscopy for the detection of colonic neoplastic lesions during surveillance. Data from a study performed in Valencia, Spain, revealed no differences between VCE with standard i-Scan chromoendoscopy and VCE with indigo carmine 0 .4 % in the detection of dysplasia in the colons of patients with longstanding IBD[37 ]. However, VCE with i-Scan was a less time-consuming alternative. A meta-analysis from 2020 that included 17 randomized clinical trials and almost 2500 patients showed the superiority of dyespray chromoendoscopy compared with standard-definition white-light endoscopy.No differences were detected when dye-spray chromoendoscopy was compared with high-definition white-light endoscopy or narrow-band imaging[38 ].
Therefore, it is very likely that we can use video chromoendoscopy as the technique of choice for the screening and follow-up of affected patients (Table 3 ).
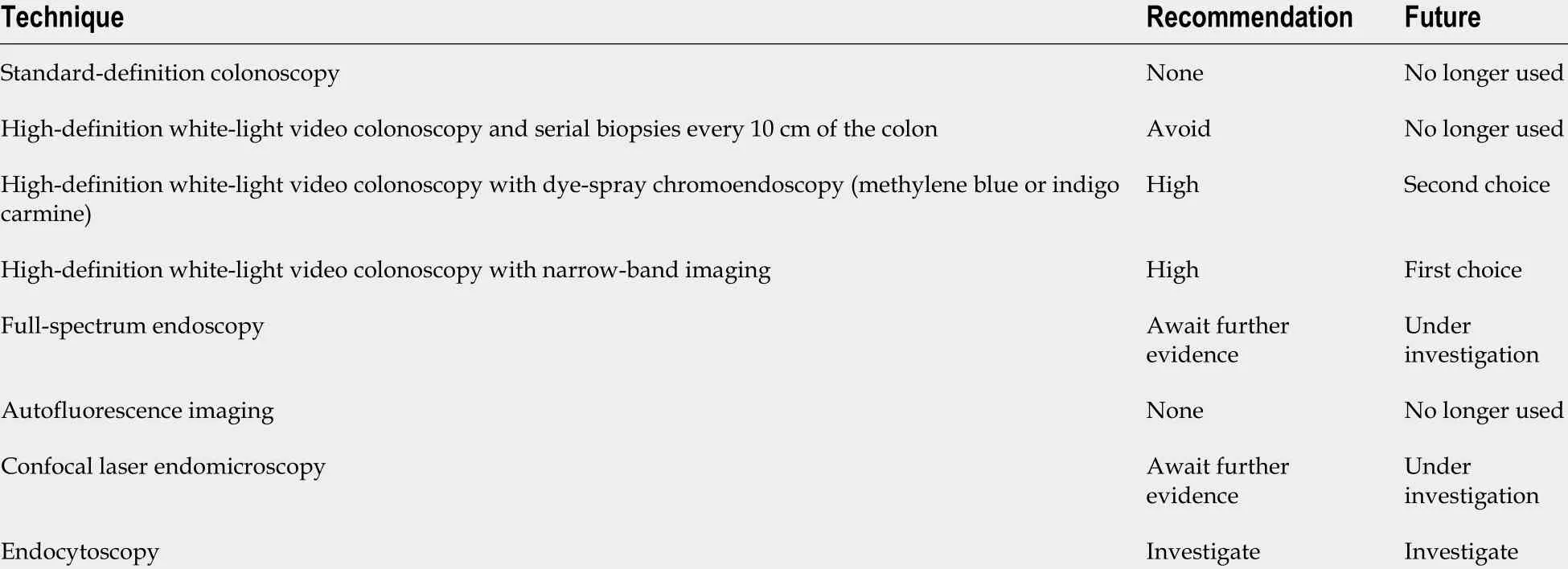
Table 3 Summary of endoscopic detection techniques
METHOD FOR TAKING BIOPSY SPECIMENS
The methods for taking targeted and serial biopsy specimens during chromoendoscopy might also be subject to change. This aspect was evaluated in a French randomized controlled trial[39 ], in which the authors evaluated whether taking serial biopsy specimens increased the detection rate for neoplasms in patients who had undergone screening for CRC and UC. They observed that while the yield was low,random biopsies for the detection of dysplasia should be combined with chromoendoscopy in patients with IBD and concomitant PSC, a personal history of neoplasm or the lead pipe sign. Furthermore, the rate of detection of additional neoplasms was 15 %in this subgroup of patients. Along the same lines, Huet al[40 ] recently published the results of a retrospective study of 300 patients with IBD in which they analysed the detection of dysplasia with targeted and random biopsy in 422 colonoscopies. The authors found that in up to 18 % of the colonoscopies, dysplasia was identified using random biopsy. Risk factors such as concomitant PSC, a longer duration of disease,and endoscopically active disease increased the likelihood of a dysplastic lesion being detected in random biopsy, suggesting that specific high-risk patients could benefit from this strategy for the detection of dysplasia.
Previous reviews have suggested that additional biopsy specimens should be taken from the area of flat mucosa surrounding dysplastic polypoid lesions resected in IBD to confirm the absence of residual neoplasmin situ[28 ]. Nevertheless, recent studies consider these biopsies to be of low and even insignificant diagnostic yield and not predictive of findings in subsequent follow-up colonoscopy[41 ]. The findings reported cast doubt on the usefulness and yield of this procedure. New, high-definition techniques and chromoendoscopy may obviate the need for the biopsy of the adjacent mucosa to detect invisible dysplasia in many patients[42 ,43 ]. A recent retrospective cohort study compared the long-term effectiveness of targeted biopsy of suspected lesions with that of random biopsy and found robust evidence for targeted biopsy in the prevention of death from colon cancer. However, since panchromoendoscopy was used in only 4 .6 % of patients, the findings cannot be extrapolated[44 ].
Today, doubt remains as to which surveillance technique is best for patients with IBD and the involvement of the colon but no other risk factors for CRC: high-definition colonoscopy with random biopsy, VCE and targeted biopsy, or high-definition colonoscopy with targeted biopsy.
ENDOSCOPIC-HISTOLOGIC EVALUATION
The Paddington International Virtual ChromoendoScopy ScOre (PICaSSO) is a recently reported VCE scoring system in UC to redefine endoscopic findings of mucosal and vascular healing developed by international experts in optical diagnosis.Interobserver agreement on the pretest and the post-test evaluation was very good for the Mayo endoscopic score, Ulcerative Colitis Endoscopic Index of Severity, Robarts Histological Index, and a full spectrum of histological changes[45 ] (Table 4 ).Furthermore, a recent real-life study revealed that the PICaSSO score correlatedstrongly with multiple histological indices and that, similar to histology, it predicted specified clinical outcomes at 6 and 12 mo. The authors concluded that PICaSSO can be a useful endoscopic tool in the therapeutic management of UC[46 ].
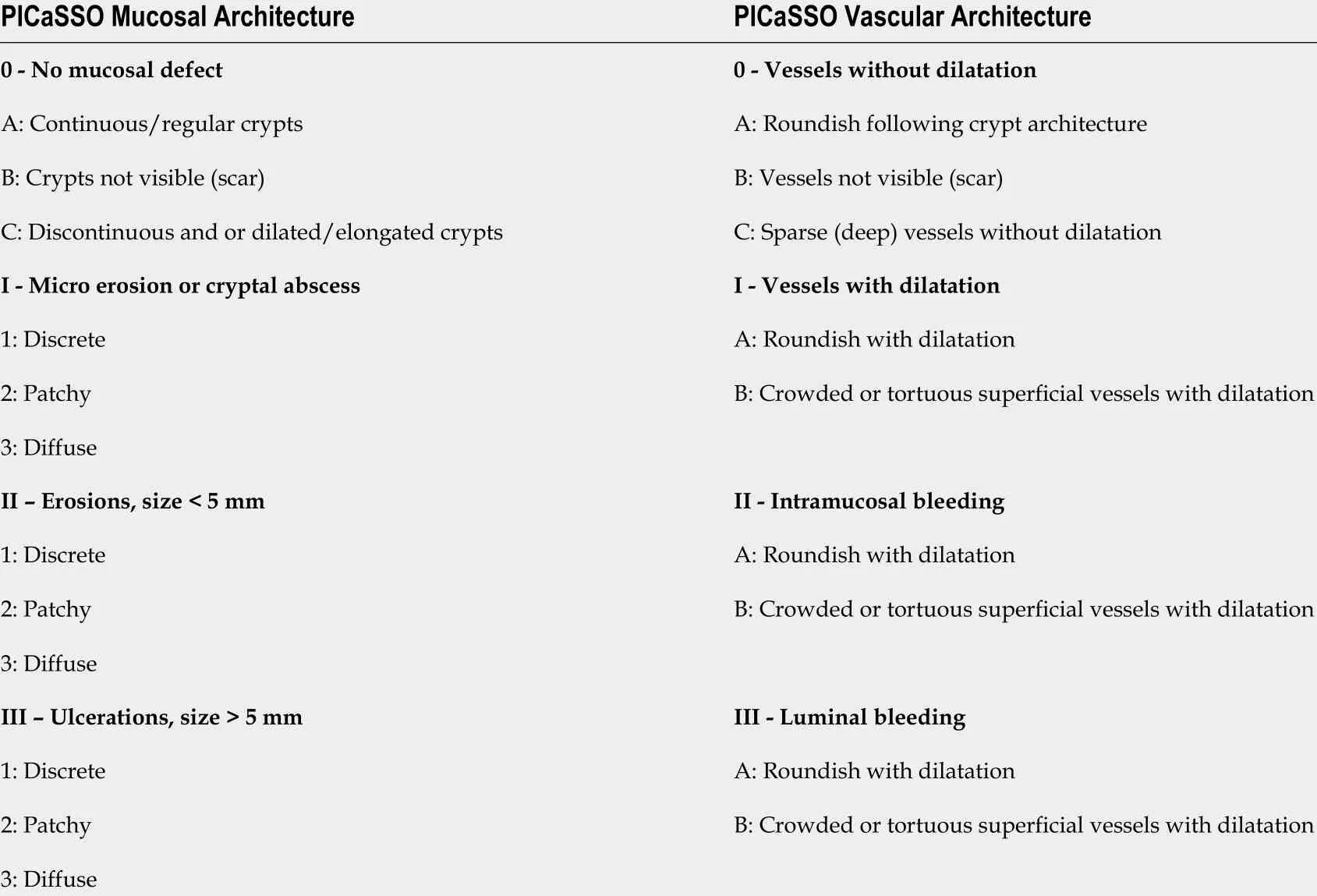
Table 4 The Paddington International Virtual ChromoendoScopy ScOre in ulcerative colitis
SERRATED EPITHELIAL CHANGE
In recent years, several studies have investigated the involvement of serrated epithelial changes in patients with IBD. This histopathological finding, which appears in patients with a long history of colitis in areas of nodular mucosa, is characterized by crypt distortion with diffuse striae and an epithelium rich in goblet cells. Parianet alrecently performed a case-control study and a systematic review with a meta-analysis of 196 patients with UC in which they found higher rates of synchronous or metachronous tumours in patients with IBD and serrated epithelial change, thus leading us to believe that these patients require closer monitoring, possibly with yearly endoscopy[47 ].
PATIENTS WITH A LARGE NUMBER OF POLYPS IN SURVEILLANCE ENDOSCOPY
When pseudopolyps are found along an extensive area of the colon and it is impossible to remove them all appropriately to evaluate dysplasia, possible options should be discussed with the patient. Given the risk of nonidentified neoplasms,prophylactic proctocolectomy should be considered. In specific cases (patients with advanced age, high surgical risk, and refusal to undergo proctocolectomy), closer follow-up should be considered as an alternative[1 ,23 ]. With respect to this clinical situation, there have been no changes in the recommendations. This aspect should be evaluated in future studies, mainly with emerging endoscopic techniques.
INTEROBSERVER AGREEMENT IN THE HISTOLOGY ANALYSIS
The difficulties involved in interpreting histology specimens are well known with respect to the presence/absence and grade of dysplasia[48 ].
A recent study analysing interobserver agreement on histology findings in inflammatory bowel disease found that, with respect to the presence of dysplasia, interobserver agreement was moderate, with greater agreement for high-grade dysplasia. In addition, when endoscopic data and histological data were combined, dysplasiaassociated lesions or masses were more common than adenoma-like masses.Therefore, the authors proposed using immunohistochemistry to increase the capacity for detecting these lesions, as well as a review of samples by a pathologist specializing in digestive diseases[49 ].
NEW ENDOSCOPIC TECHNIQUES
Full-spectrum endoscopy
Full-spectrum endoscopy (FUSE) comprises 2 Lateral cameras in addition to the traditional front camera, and this configuration makes it possible to see behind the folds and blind spots, thus providing a panoramic view.
Leonget al[50 ] performed a prospective, randomized, crossover tandem colonoscopy study of 52 patients to compare standard forward-viewing colonoscopy(FVC) with FUSE for the detection of dysplasia in patients with IBD. FUSE revealed significantly more dysplastic lesions than FVC, although the withdrawal time was significantly greater. Targeted biopsy revealed significantly more dysplastic lesions than random biopsy (P< 0 .0001 ).
Autofluorescence imaging
Autofluorescence imaging (AFI) is based on the detection of natural tissue fluorescence emitted by endogenous molecules (fluorophores) such as collagen,flavins, and porphyrins. After excitation by a short-wavelength light source, these fluorophores emit light of longer wavelengths (fluorescence). The overall fluorescence emission differs between the various tissue types owing to the corresponding differences in fluorophore concentration, metabolic state, and/or spatial distribution.These colour differences in fluorescence emission can be captured in real time during endoscopy and used for the detection or characterization of lesions[51 ]. A multicentre international prospective randomized controlled trial compared images taken with AFI with chromoendoscopy for the detection of dysplasia in 210 patients with UC. The relative detection rate for dysplasia had to be greater than 0 .67 (based on an 80 %confidence interval) to justify a subsequent noninferiority trial. Dysplasia was detected in 20 patients (19 %) using chromoendoscopy and in 13 (12 %) using AFI. Therefore, AFI proved to be inferior to chromoendoscopy, and the criteria for performing a large-scale noninferiority trial were not fulfilled. The authors concluded that AFI should not be investigated as an alternative approach for monitoring the presence of dysplasia[52 ].
Confocal laser endomicroscopy
Confocal laser endomicroscopy (CLE) is a new method used for obtainingin vivoimages of abnormalities of the mucosa at the subcellular level. The technique uses intravenous fluorescent agents, contrast, and a specialized probe that can be passed through the working channel of an endoscope, thus enabling real-time 1000 -fold magnification of the mucosa of the colon. CLE has been shown to help differentiate among neoplasms, solitary adenomas, and benign regenerative changes (which can be seen in much the same way as dysplasia), with 97 .8 % accuracy[53 ].
Pilot trials have been performed with variations of this technique. One study evaluated the potential role of CLE combined with a fluorescein-labelled peptide to stain and detect dysplasia associated with UC. A heptapeptide derived from phages with marked affinity for dysplastic tissue was synthetized and labelled with fluorescein (VRPMPLQ peptide). The study included 9 patients who underwent the resection of 11 Lesions. The different affinities of fluorescein for nondysplastic tissue,inflammatory polyps, and dysplastic tissue enabled better characterization. The authors concluded that VRPMPLQ is a promising approach for the detection of dysplasia in patients with IBD. Morein vivostudies in larger populations are required to evaluate the effective contribution of this molecular probe in the management of lesions detected during the surveillance of patients with UC[54 ]. However, the results of these studies should be confirmed in larger series. CLE is currently restricted to research.
Endocytoscopy
Endocytoscopy is a novel ultra-high magnification endoscopic technique designed to provide excellentin vivoassessment of lesions found in the gastrointestinal tract. When used with intraprocedural stains, endocytoscopy enables microscopic visualization of the gastrointestinal mucosal surface[55 ,56 ].
Nevertheless, the application of endocytoscopy in the diagnosis of colitis-associated CRC has received little attention. A recently published case report revealed that endocytoscopy can be used to obtain information on the nuclei and lumen of the glands in colitis-associated CRC. Furthermore, colitis-associated CRC is often difficult to diagnose owing to the effects of inflammation, and the use of endocytoscopy can reduce the frequency of unnecessary biopsies[57 ].
DEVICES FOR IMPROVING ENDOSCOPIC VISION
Endocuff Vision (ARC Medical Design Ltd) is a distal colonoscopic accessory with smooth projections in the form of fingers that aims to flatten mucosal folds, and it has been shown to improve the rate of the detection of adenomas in patients with IBD undergoing screening for CRC[58 ]. The device is not currently recommended in patients with severe colitis because of concerns over mucosal injury[59 ], although it has not been previously studied in clinically active patients with IBD undergoing surveillance colonoscopy for the detection of dysplasia. A study of 25 patients evaluated the safety and viability of Endocuff Vision-assisted high-definition chromoendoscopy in patients with clinically active UC undergoing surveillance for dysplasia. The authors concluded that the technique is feasible and safe in patients with UC undergoing surveillance colonoscopy to rule out dysplasia[60 ]. Other studies reported that Endocuff could facilitate polypectomy, especially in the flexible folds of the sigmoid colon, thus enabling greater stabilization of the endoscope when facing the polyp[61 ]. In the future, it will be necessary to determine whether these devices can increase the rate of detection of polyps and facilitate their extraction without increasing the rate of complications in patients with UC.
COLON CAPSULE ENDOSCOPY
A priori, capsule endoscopy is an attractive option for screening CRC in patients with IBD because it is noninvasive and has proven useful in certain situations, namely, after incomplete colonoscopy, when the patient refuses colonoscopy, or when sedatives are contraindicated.
Regarding its yield, second-generation capsule endoscopy (CE-2 ) is almost at the same level as colonoscopy, with 80 %-95 % sensitivity for the detection of polyps ≥ 6 mm. The limitations of CE-2 in CRC are that it cannot be used for biopsy, for obtaining samples of the intestinal mucosa, or for resecting any lesions detected[62 ].
This is a field for future research, which will undoubtedly provide huge surprises in the coming years. Prototypes with steerable and self-propelling technology have already been designed[63 ].
COMPUTER-AIDED DETECTION
Nonblinded trials have shown that colonoscopy with computer-aided detection(CADe) improves the detection of polyps and adenomas in the colon by providing visual alarms during the procedure[64 ]. The technique was developed in China in a randomized, double-blind clinical trial aimed at evaluating the efficacy of a CADe system. The study excluded patients with IBD. The rate of the detection of adenomas was significantly greater in the CADe group than in the control group[65 ]. In the future, it will be necessary to evaluate whether computational devices that facilitate detection are valid for patients with IBD.
COSTS ASSOCIATED WITH SCREENING
Few studies have evaluated the costs—and more especially the cost-effectiveness—of screening in patients with UC. One of the first studies to do so was published by Provenzaleet al[66 ] in 1998 , who analysed the cost-effectiveness of CRC screening programmes and found a favourable association with screening. However, endoscopic technology has changed considerably since then.
The study by Konijetiet al[67 ] in 2014 evaluated 3 strategies with different surveillance intervals—chromoendoscopy with targeted biopsy, white-light endoscopy with random biopsy, and no surveillance—taking into account the financial costs and the characteristics of the United States health system. However, compared with no surveillance, chromoendoscopy was only cost-effective at intervals of at least 7 years, with an incremental cost-effectiveness of $77176 . Chromoendoscopy was the most cost-effective strategy, with a sensitivity > 0 .23 for the detection of dysplasia and a cost < $2200 , regardless of the sensitivity of WLE for the detection of dysplasia. The estimated population lifetime risk of developing CRC ranged from 2 .5 % (annual chromoendoscopy) to 5 .9 % (chromoendoscopy every 10 years).
This aspect should be evaluated in the different health systems, given the large potential differences in the cost of screening programmes between countries.
CHEMOPREVENTION
Cancer chemoprevention involves the chronic administration of a synthetic, natural, or biological agent to reduce or delay the occurrence of malignancy[68 ]. In addition, the agent administered must be effective, safe, acceptable to patients, and inexpensive.
Chronic inflammation of the mucosa in patients with UC is the main risk factor for the development of CRC[69 ].
No medical treatment has proven able to sufficiently prevent dysplasia or CRC and thus obviate the need for colonoscopic surveillance in UC[23 ].
Chemoprevention is considerably controversial owing to the diversity of studies and varying reports on adherence to treatment, and available evidence supports the role of 5 -ASA as chemopreventive therapy[70 ]. Immunomodulators could play a role owing to their control of mucosal inflammation, at least in a subgroup of patients[71 ].The control of inflammation achieved with anti-TNFa agents would probably reduce the risk of CRC in patients with UC. Even in more recent observational studies, the number of patients exposed to tumour necrosis factor-alpha inhibitor agents is too low to adequately evaluate the potential chemopreventive effects of these agents[71 ]. In UC and concomitant PSC, low-dose ursodeoxycholic acid could reduce the risk of CRC, although evidence for this hypothesis is weak[72 ,73 ].
While much remains to be done in the field of the chemoprevention of CRC in patients with UC, the main barrier in the coming years will be the difficulty in performing clinical trials that provide more robust evidence.
CONCLUSION
Despite the advances made in the field, the following areas warrant further study: (1 )The tailoring of surveillance intervals to the individual patient; (2 ) Continuous updating of recommendations based on the best available evidence; (3 ) Greater adherence by physicians to the recommendations of scientific societies; (4 ) The development of noninvasive biomarkers that could support or act as a screening approach before endoscopy; and (5 ) Efforts to reduce barriers to surveillance,including safe extension of intervals in patients with a lower risk.
The challenge in the coming years will be to match the individual patient with the best option for endoscopic surveillance. We must bear in mind the large number of newly diagnosed patients, in addition to those currently under surveillance and the fact that they are ageing, together with the increasing price of new technology and surveillance modalities. The maintenance of an adequate and efficient physicianpatient relationship in decision making will be the greatest challenge we have to face in the coming years.
 World Journal of Gastroenterology2022年5期
World Journal of Gastroenterology2022年5期
- World Journal of Gastroenterology的其它文章
- Machine learning models and over-fitting considerations
- Artificial intelligence model validation before its application in clinical diagnosis assistance
- Abnormal liver chemistries as a predictor of COVID-19 severity and clinical outcomes in hospitalized patients
- Connective tissue growth factor expression hints at aggressive nature of colorectal cancer
- Effect of Bacillus subtilis, Enterococcus faecium, and Enterococcus faecalis supernatants on serotonin transporter expression in cells and tissues
- Viral hepatitis: Innovations and expectations