
Fatal rhabdomyolysis and disseminated intravascular coagulation after total knee arthroplasty under spinal anesthesia:A case report
2022-03-15 07:12:22DaeHunYunEunHaSukWanJuEunHyoungSeoHyunKang
World Journal of Clinical Cases 2022年4期
INTRODUCTION
Rhabdomyolysis is a clinical syndrome caused by the destruction of skeletal muscle fibers,which leads to the leakage of intracellular contents into circulation.Various toxic materials,such as creatine kinase (CK),lactate dehydrogenase,myoglobin,aspartate transaminase (AST),and electrolytes,are released to the bloodstream,causing systemic symptoms,including hyperkalemia,hypovolemia,acute kidney injury (AKI),metabolic acidosis,compartment syndrome,cardiac dysrhythmia,and disseminated intravascular coagulation (DIC) in severe cases[1].Rhabdomyolysis can be classified according to the mechanism of injury,such as hypoxic,physical,chemical,or biological,or classified as acquired or inherited.Trauma is the most common cause,with less common causes being toxins,drugs,alcohol,infection,sepsis,excessive workouts,myopathies,endocrinopathies,thermal injury,and electrolyte abnormalities[2].
As a form of trauma,surgery can induce rhabdomyolysis due to ischemic muscle injury from long-term immobilization or excessive tissue compression during the surgery.Recently,there have been increasing numbers of descriptions of rhabdomyolysis which developed in the perioperative period.The use of a pneumatic tourniquet,which is widespread in extremity orthopedic surgery to create a bloodless operation field,is rarely associated with morbidity and mortality but can induce rhabdomyolysis.In this report,we present an unusual case of tourniquet-induced rhabdomyolysis after total knee arthroplasty (TKA) under spinal anesthesia,which was ultimately fatal.
And when she had done this, she went up to the feast, and everyone stepped out of her way, for nobody knew her, and they thought she must be a King s daughter
Then he got up to leave her, and said in his gruff voice: Do you love me, Beauty? Will you marry me? Oh! what shall I say? cried Beauty, for she was afraid to make the Beast angry by refusing
CASE PRESENTATION
Chief complaints
A 77-year-old male (weight:51 kg,height:170 cm) exhibited a drowsy mental state about 24 h after TKA.
As the patient persisted in the drowsy mental state,additional tests found that serum myoglobin was 1027 ng/mL (normal:28-72 ng/mL),and random urine analysis revealed that urine myoglobin was 25.3 ng/mL and red blood cell count was 100/high powered field (HPF) (normal:0-4/HPF).
After 40 years, he passed away, left her a letter which said, My dearest, please forgive me, forgive my whole life s lie. This was the only lie I said to you -- the salty coffee. Remember the first time we dated? I was so nervous at that time, actually I wanted some sugar, but I said salt. It was hard for me to change so I just went ahead. I never thought that could be the start of our communication! I tried to tell you the truth many times in my life, but I was too afraid to do that, as I have promised not to lie to you for anything... Now I m dying9, I m afraid of nothing so I tell you the truth, I don t like the salty coffee, what a strange bad taste... But I have had the salty coffee for my whole life! Since I knew you, I never feel sorry for anything I do for you. Having you with me is my biggest happiness for my whole life. If I can live for the second time, still want to know you and have you for my whole life, even though I have to drink the salty coffee again.
When the mental change was identified,the patient’s mental state was assessed with a Glasgow coma scale score of 8/15 (M5/V2/E1).At that time,vital signs were BP of 110/70 mmHg,HR of 122 beats/min,body temperature of 37.9 °C,and SpOof 86%-90%.Electrocardiogram was normal.
History of past illness
Excessive or prolonged compression by a pneumatic tourniquet during a lower extremity surgery can bring about tissue ischemia,both beneath the cuff and in the distal tissue,which can therefore lead to rhabdomyolysis.However,this is a rare outcome,as only a few cases of rhabdomyolysis after tourniquet application in lower extremity surgery have been reported[7-12].Tourniquet-induced rhabdomyolysis occurs regardless of the anesthetic type and is generally related to longer tourniquet application times and unusually high tourniquet pressures.Therefore,it is important to control the tourniquet application time and pressure to prevent rhabdomyolysis.
Perioperative management for TKA
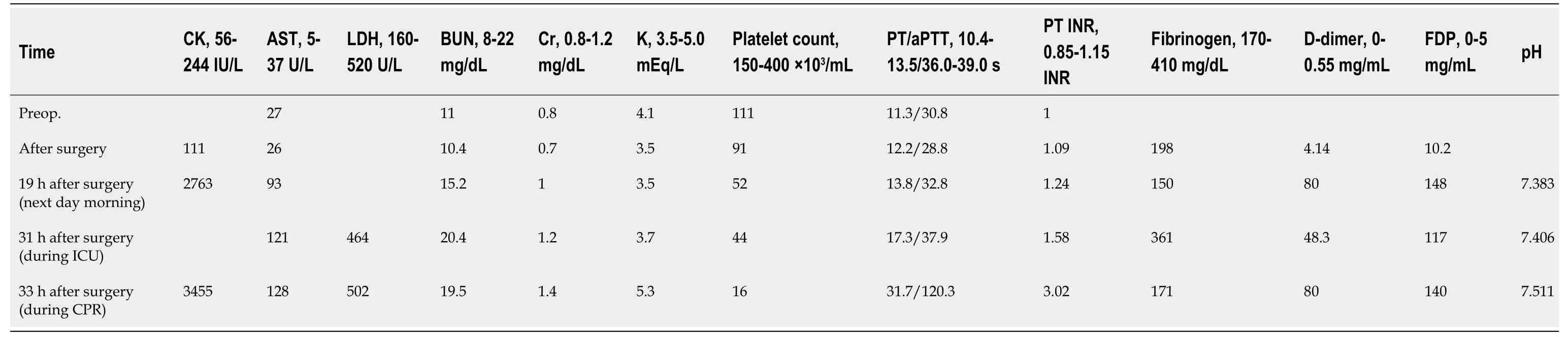
Immediately after surgery in the recovery room,laboratory results were within the normal range,with the exception for some derangement in the coagulation panel.About 19 h after surgery,CK was markedly increased to 2763 IU/L (normal:56-244 IU/L),creatine kinase-myocardial band (CK-MB) was elevated to 13.26 ng/mL (normal:<4.87 ng/mL),and AST and BUN/Cr were also elevated.However,troponin-I was normal at 0.100 ng/mL (normal:<0.16 ng/mL).Prolonged coagulation battery,thrombocytopenia,and high levels of fibrinogen degradation product and Ddimer were detected in the early postoperative phase,and serial tests demonstrated progressive deterioration of DIC.Additional laboratory tests performed during the intensive care unit (ICU) stay showed continued deterioration of the parameters.Serial changes in the parameters are summarized in Table 1.
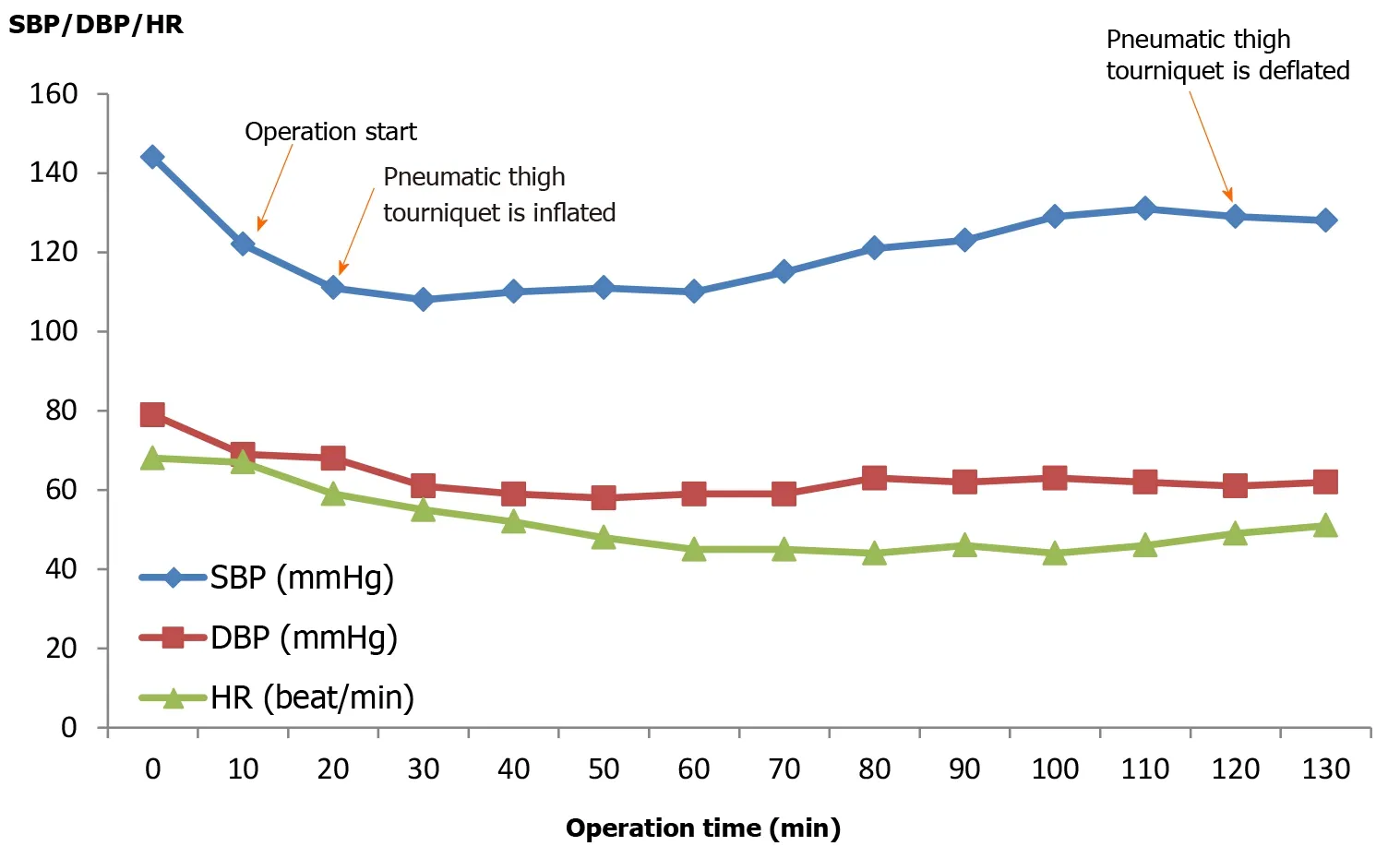
Aspirin was stopped 7 d before surgery,and no medication was administered on the morning of surgery.After arriving at the operating room,initial vital signs were blood pressure (BP) of 144/79 mmHg,heart rate (HR) of 68 beats/min,and SpOof 97%.Bupivacaine (0.5%,10 mg) was injected into the subarachnoid space at T10 for the spinal block.Intravenous dexmedetomidine was infused (0.5 μg/kg/min for first 10 min,then at 0.4-0.6 μg/kg/min) for sedation.A pneumatic thigh tourniquet was applied intraoperatively at an inflation pressure of 300 mmHg for 100 min.Total anesthesia time was 2 h and 10 min.During surgery,600 mL of crystalloid was administered and 150 mL of urine were collected.Estimated blood loss was 90 mL.Intraoperative vital signs showed BP of 100-130/50-70 mmHg,HR of 45-55 beats/min,and SpOof 97%-99% (Figure 1).
On arrival in the recovery room,initial vital signs were BP of 97/55 mmHg,HR of 41 beats/min and SpOof 100%.During the first hour of recovery,vital signs were maintained as follows:BP of 95-100/55-60 mmHg,HR of 40-45 beats/min,and SpOof 98%-100%.About 90 mL of urine and 70 mL of blood were drained,and 400 mL of crystalloid was administered.
Postoperative management for TKA
After surgery,post-operative pain was managed with an intravenous patientcontrolled analgesia (AutoFuser;ACE Medical,Beverly Hills,CA,United States),including 1 mg fentanyl (Hana Pharm,Seoul,South Korea),of which the baseline infusion rate,bolus demand dose,and lock-out time were 2 mL/h,2 mL,15 min.Antibiotics (Refosporen,1 g and cefazedone sodium 1 g;both from Hanall Biopharma,Seoul,Korea) were also injected bid.The morning following surgery,the patient complained of severe pain on the right thigh and overnight shivering.Tridol Injection (tramadol hydrochloride 50 mg/mL;Yuhan Pharm,Seoul,South Korea) was injected for pain control.
When my oldest son was in high school, he planned to attend a Christian1 contemporary concert with the youth group from our church. To my amazement2, Aaron invited me to go along; he knew I enjoyed the music of one of the performers. I readily accepted; however, by the time the date of the concert arrived, I had questions about going. My youngest son, who has Down syndrome3 and progressive heart disease, had been ill, and I was concerned about him. My husband encouraged me to attend the concert, assuring me he was quite capable of taking care of our youngest. I wavered.
Physical examination
The startled boy started to sob8 and sob, and he couldn t stop crying. His whole body shook. He looked up at his father and said through his tears, I was planning on committing suicide tomorrow, Dad, because I didn t think you loved me. Now I don t need to.
On physical examination,the patient’s right thigh,which had been cuffed with tourniquet during the operation,was stiff and had turned a dark brown,without swelling,whereas the surgical site and distal extremity were unaffected.Urine collected in a Foley bag was dark colored,and the urine output every 8 h after operation was 100 mL,220 mL,and 250 mL,respectively,for a total of 570 mL/d,which indicated oliguria.
Laboratory examinations
Prior to surgery,chest X-ray was normal.Echocardiogram showed a left ventricular ejection fraction of 61%,grade 2 diastolic dysfunction,mild aortic regurgitation,trivial mitral regurgitation and tricuspid regurgitation.All hematological parameters were unremarkable,with normal blood urea nitrogen/creatinine (BUN/Cr) of 11.0/0.8 mg/dL and low hemoglobin of 11.9 g/dL.
Imaging examination
Tourniquet-induced rhabdomyolysis was diagnosed based on the serum CK level (5 times the upper limit of normal range),myoglobinuria,and physical examination.Laboratory findings revealed that AKI (AKIN criteria stage 1,urine output<0.5 mL/kg/h for 6-12 h and serum Cr increase 0.3 mg/dL within 48 h) and DIC accompanied the rhabdomyolysis.
Further diagnostic work-up
George, calm on the outside but frantic5 on the inside, re-entered the store with long steps. He followed the same route he had walked before, starting at the bread counter, to the dairy section, the aisle6 where salt and sugar were placed, then the rest of the store. They were all open aisles7 and it did not take long to be convinced that the gloves were not in sight. After checking the forty-foot-long bread section, he quickened his pace through the two-hundred-foot aisle leading to the dairy products. There he even turned over egg boxes to see if the gloves had fallen in between. Several minutes of anxious searching turned out to be in vain. His heart grew heavier and he started to sweat as he entered aisle six. The salt and sugar were packed in white bags, and anything black could be spotted8 easily. No. His black gloves were gone. His sharp eyes could not have missed them.
FINAL DIAGNOSIS
Immediately after the mental change was identified,brain magnetic resonance imaging (MRI) was performed for differential diagnosis.Mild small vessel disease was identified,but no notable hemorrhage or infarction was evident.
TREATMENT
About 1 h after the change in the patient’s mental status,BP dropped to 88/62 mmHg,and norepinephrine (0.5-1 μg/kg/min) was infused to maintain systolic BP above 100 mmHg.After brain MRI examination,the patient was admitted to the ICU.An arterial line was placed in the left radial artery for continuous monitoring of blood pressure,and a central line was secured in the right internal jugular vein for adequate fluid supply and cardiovascular monitoring.A nephrologist was consulted,and fluid treatment of 5 L/d was prescribed.Dialysis was scheduled due to progressive renal impairment.Fluid loading was initiated with normal saline at 400 mL/h for 2 h,and then decreased to 250 mL/h.For renoprotection,Lasix (furosemide,20 mg injection;Handok,Seoul,South Korea) and sodium bicarbonate (40 mL injection of 8.4%;Jeil Pharmaceutical,Daegu,South Korea) were administered for diuresis and urine alkalization,respectively.The urine output was 110 mL for the first 3 h and 600 mL for next 4 h.Denogan (propacetamol hydrochloride 1 g injection;Yungjin Pharmaceutical,Seoul,South Korea) was administered to control fever.About 2 h after fluid administration,the patient’s mental status was restored to alert.His vital signs were as follows:BP of 90-110/60-70 mmHg,HR of 104 beats/min,body temperature of 36.2 °C,and SpOof 98% on room air.However,after 2 h,the patient’s body temperature elevated again to 38.0 °C.Serial vital signs were summarized in Table 2.
A rustle10 at the front door told me Holly had arrived home from school. Susan invited me to come over to her house after school tomorrow, she announced as she plunked her books down on the kitchen table. Although her voice carried a so-what attitude, I sensed she was pleased by the invitation.

OUTCOME AND FOLLOW-UP
Approximately 5 h after the patient’s mental state was restored,his BP and HR dropped suddenly,followed by cardiac arrest.Cardiopulmonary resuscitation was performed for about 1 h;however,the patient was not resuscitated.At the will of the guardian,we stopped further resuscitation,and he expired.
DISCUSSION
Rhabdomyolysis has been described during the perioperative period after various types of surgeries,including urologic,spinal,coronary bypass graft,bariatric,and head and neck.Risk factors for developing rhabdomyolysis during surgery and subsequent post-operative period are:prolonged surgical duration,improper positioning,male sex,obesity,age<10 or>60 years,diabetes,hypertension,kidney disease,endocrine disease,chronic drug users,and sepsis[3-6].
The patient had been diagnosed with unstable angina 8 years prior,which was treated with a coronary stent insertion.He had been subsequently treated with Sigmart (nicorandil 5 mg;JW Pharmaceutical,Seoul,South Korea),aspirin (enteric coated tab,100 mg),Almarl (arotinolol 5 mg;HK inno.N,Seoul,South Korea),and Herben (diltiazem 30 mg;HK inno.N).
Although optimal tourniquet pressure and inflation time for prevention of muscle injury have not been clearly defined,several methods are used to determine the optimal inflation pressure for lower extremity.The first is determined by adding 100-150 mmHg above the arm systolic blood pressure[13],and a second is by adding 50-75 mmHg to the pressure required to obliterate the peripheral pulse on Doppler probe[14].Additionally,Horlocker[15] recommended the tourniquet inflation time<120 min to prevent nerve injury during TKA not pertaining to muscle injury.In TKA,tourniquet is usually used at 300 mmHg of pressure until completion of cementing and total inflation time is limited to 120 min.If the operation is expected to be longer,the tourniquet should be deflated for a minimum of 20 min every 60-90 min[16].
Besides the optimal use of tourniquet,the safe inflation pressure and time seem to be dependent on several variables.For example,underlying conditions of a patient are also important in predicting the development of rhabdomyolysis after tourniquet application.Additionally,factors,including age,blood pressure,co-morbidities and the condition of the extremity,should also be considered when assessing the risks of developing rhabdomyolysis after using a tourniquet during surgery.To our knowledge,only two descriptions of rhabdomyolysis after TKA have been reported[8,9].Karcher[8] reported rhabdomyolysis,AKI,and liver dysfunction in an obese patient after TKA using a short period (50 min) of tourniquet application at 350 mmHg and Palmer[9] described a case of rhabdomyolysis and AKI after TKA in an elderly patient with chronic obstructive airway disease,hypertension,coronary artery disease,and heart failure,in which the tourniquet application time was 92 min at 350 mmHg.Both cases had relatively high tourniquet pressure and underlying risk factors,including advanced age,obesity,and cardiovascular disease.
Rhabdomyolysis can be precipitated by hypotension or hypovolemia due to the distortion of perfusion to the affected muscles.Glassman[17] suggested that permissive hypertension would prevent the development of rhabdomyolysis by improving perfusion to compressed muscles.In TKA,tourniquet use significantly decreases intraoperative blood loss but cannot decrease total blood loss[18],therefore sufficient fluid should be supplied postoperatively after tourniquet deflation when persistent bleeding is ongoing.In our patient,the tourniquet pressure and duration did not exceed the recommended guidelines,with 300 mmHg of pressure applied for 100 min.The patient had two known risk factors of male sex and old age.Additionally,preoperative dehydration,sustained postoperative hypotension,and his history of ischemic heart disease are thought to be contributing factors of the rhabdomyolysis development,as together these conditions contributed to peripheral vascular insufficiency.Moreover,postoperative shivering and fever may have limited tissue perfusion and oxygen supply,and overlapping AKI and DIC cascade further led to the rapid progression of the disease.
TKA is usually performed on older patients,many with various underlying diseases,and spinal anesthesia is preferred in lower extremity surgery for elderly patients to avoid risks of general anesthesia.However,hypotension induced by spinal block and dexmedetomidine infusion for sedation might have contributed to rhabdomyolysis by lowering perfusion pressure.Therefore,meticulous care in tourniquet use and maintaining adequate perfusion pressure are required to prevent muscle injury.We recommend the lowest effective inflation pressure with minimal inflation time in TKA because the tourniquet inflation time and pressure have additive effects.
The diagnosis of rhabdomyolysis in our patient was confirmed by elevated serum CK levels of>1000 U/L,which is 5-times the normal upper limit.The patient also had dark urine and severe pain in the area the tourniquet was applied.Clinical suspicion is important to make a timely decision for diagnosis,so physicians should pay attention to the clinical presentations.The symptoms of this syndrome vary,from minor and subclinical to severe and even fatal,according to the degree of skeletal muscle injury.Musculoskeletal signs are inappropriate severe pain,occasional tenderness or swelling in the affected muscle,and skin changes,indicating muscle necrosis can be present.Simple myalgia,fatigue,weakness,fever,tachycardia,nausea,and vomiting are common general manifestations,and pigmenturia can be observed in some cases.Non-specific symptoms,such as hypotension,shock and changes in mental status,might be present,requiring differential diagnosis.Complications of rhabdomyolysis are hyperkalemia,hypocalcemia,elevated AST,cardiac dysrhythmias,and cardiac arrest in early phase.AKI and DIC can develop,usually 12-72 h after insult,as late complications in serious cases.
In our patient,clotting studies detected an early DIC cascade in the postoperative period.Although fibrinolysis is activated transiently after tourniquet use itself,myocyte components can activate the coagulation pathway leading to DIC in severe rhabdomyolysis[1].Persistent oliguria and progressive increase in creatine levels showed ongoing kidney injury.AKI is the most common serious complication of rhabdomyolysis,occurring in approximately 10%-67%.The mortality rate of rhabdomyolysis is known to about 10%,which increases with the degree of kidney injury up to 50%[19].AKI is an independent predictor of higher mortality and more likely to develop in elderly patients and in patients with chronic comorbid disease,such as congestive heart failure,coronary artery disease,diabetes mellitus,atrial fibrillation,hyperlipidemia,and chronic kidney disease[20].
Although clear guidelines for the management of rhabdomyolysis have not yet been developed,the goals of rhabdomyolysis treatment are the same as maintaining adequate tissue perfusion and oxygenation to prevent hypoxic tissue injury and preserving renal function by maintaining urine output.Prompt fluid replacement is the keystone of treatment.Aggressive hydration should be initiated as soon as possible to control hypovolemia and maintain adequate urine output (>200-300 mL/h in adult).High volume fluid replacement,up to 1.5 L/h or more than 6 L/d,may be needed to obtain satisfactory urine output[21,22].Mannitol,loop diuretics,and sodium bicarbonate have been used for renal protection,but the additional benefit beyond fluid resuscitation is not known.Renal replacement therapy can be considered in deteriorating kidney function,uncontrolled hyperkalemia,metabolic acidosis,and fluid overload.In the present case,early mental changes prompted a brain MRI to rule out intracranial accident.Unfortunately,the treatment of rhabdomyolysis,such as early hydration,was delayed during the radiological study.After radiological work up,the patient was transferred to the ICU,and urine output was found to be inadequate,despite fluid replacement and pharmacological renoprotection.Higher volume expansion should have been performed in order to achieve satisfactory urine output.We thought that the unresolved dehydration and overlapping DIC cascade resulted in the devastating outcome.
CONCLUSION
Rhabdomyolysis induced by tourniquet application is very rare,but can lead to potentially lethal results if it develops.Physicians should be aware of the possibility of tourniquet-induced rhabdomyolysis after TKA,regardless of the type of anesthesia.Tourniquets should be used carefully in elderly patients with risk factors,and maintaining hemodynamic stability with adequate fluid replacement is important during the perioperative period.Regular monitoring of CK level and sufficient attention are necessary to detect this syndrome early.Once rhabdomyolysis is diagnosed,prompt aggressive treatments,including vigorous hydration,are required to save the patient,especially when accompanied by AKI or DIC.
 World Journal of Clinical Cases2022年4期
World Journal of Clinical Cases2022年4期
- World Journal of Clinical Cases的其它文章
- Surgical treatment of acute cholecystitis in patients with confirmed COVID-19:Ten case reports and review of literature
- Rituximab as a treatment for human immunodeficiency virusassociated nemaline myopathy:What does the literature have to tell us?
- Eustachian tube involvement in a patient with relapsing polychondritis detected by magnetic resonance imaging:A case report
- Endoscopic clipping for the secondary prophylaxis of bleeding gastric varices in a patient with cirrhosis:A case report
- Inflammatory myofibroblastic tumor after breast prosthesis:A case report and literature review
- Langerhans cell histiocytosis presenting as an isolated brain tumour:A case report