
Predictors of recurrent bile duct stone after clearance by endoscopic retrograde cholangiopancreatography: A case-control study
2022-03-02 06:51:52WismSbeitAnsKdhMttSimnAmirShhinTwfikKhoury
Wism Sbeit , b , Ans Kdh , b , Mtt Simn , b , Amir Shhin , b , Twfik Khoury , b,*
a Department of Gastroenterology, Galilee Medical Center, Nahariya, Israel
b Faculty of Medicine in the Galilee, Bar-Ilan University, Safed, Israel
Keywords:Endoscopic retrograde cholangiopancreatography Common bile duct Stone Recurrence
ABSTRACT
Background: Recurrent common bile duct (CBD) stone is a long-term sequalae among patients who underwent endoscopic retrograde cholangiopancreatography (ERCP) with CBD stone extraction. Data regarding risk factors for recurrent CBD stone are scarce. We aimed to identify predictors of recurrent CBD stone.
Methods: We performed a retrospective case-controlled study from January 2010 to December 2019. Inclusion criteria included patients who had recurrent CBD stone at least 6 months after the index ERCP,in which complete stone extraction was performed and normal cholangiogram was obtained. Overall, 457 patients were included. Forty-two patients (9.2%) had recurrent CBD stone, and 415 patients (90.8%) did not have recurrent CBD stone .
Results: In univariate analysis, male sex [odds ratio (OR) = 0.49, P = 0.033] was a protective factor,while endoscopic stone extraction by basket vs. balloon (OR = 2.55, P = 0.005), older age (OR = 1.03,P = 0.003), number of CBD stones (OR = 1.99, P = 0.037), size of CBD stone (OR = 4.06, P = 0.003) and mechanical lithotripsy (OR = 9.22, P = 0.004) were risk factors for recurrent CBD stone. In multivariate logistic regression analysis, mechanical lithotripsy [OR = 9.73, 95% confidence interval (CI): 1.69-55.89,P = 0.010], basket clearance vs. combined basket and balloon (OR = 18.25, 95% CI: 1.05-318.35, P = 0.046)and older age (OR = 1.02, 95% CI: 1.00-1.05, P = 0.023) were risk factors, and male sex (OR = 0.39, 95%CI: 0.19-0.81, P = 0.012) was a protective factor.
Conclusions: We identified modifiable and non-modifiable risk factors for recurrent CBD stone. Taking into consideration those factors might aid in minimizing the CBD stone recurrence risk.
Introduction
The prevalence of common bile duct stones ranges from 11%to 25% in patients with gallbladder stones [1] and approximately 10% of patients undergoing cholecystectomy will have concomitant common bile duct (CBD) stones [2] . Gallstone diseases represent a prominent cause for gastrointestinal related hospital admission [3] .CBD stones may result in severe and life-threatening conditions including pancreatitis, cholangitis and sepsis which can deteriorate to death [4] . Endoscopic retrograde cholangiopancreatography(ERCP) is currently the most commonly used and preferred method for definitive treatment of CBD stones, as endoscopic sphincterotomy (EST) followed by stone extraction with balloon or basket has been used traditionally as a standard technique [5] . However, laparoscopic surgical exploration of the bile duct is highly successful and presents similar morbidity [6] . Although ERCP is a wellestablished and highly efficacious modality for definitive bile duct stones removal, with complete stones clearance rate reaching 92%-100% [7] , recurrent CBD stones after endoscopic clearance by the standard techniques is a well-known sequel of ERCP, which is defined by stones detected more than 6 months following the index ERCP [8 , 9] , encountered in almost 10% of patients [10] . Other study reported a recurrence rate ranging from 4% to 24%, when the recurrence interval was up to 15 years period [11] .
To date, proposed predictors of recurrent CBD stone after endoscopic stone extraction include dilated bile ducts, large stones,multiple stones, and periampullary diverticulum (PAD) [10] , and a recent study has shown that acute angulation of the distal CBD was a strong predictor of recurrent CBD stone [12] . However, data regarding these associations are still scarce. Therefore, we aimed to explore parameters that may be associated with recurrent CBD stone (diagnosed>6 months after the index ERCP) among patients who underwent ERCP and definitive stone extraction.
Methods
A retrospective case control study was conducted on patients who underwent ERCP for documented CBD stone at Galilee Medical Centre, Nahariya, Israel from January 2010 to December 2019.Inclusion criteria were: 1) patients who were older than 18 years of age, 2) diagnosed with CBD stone by radiological modalities, and 3) underwent ERCP procedure including EST plus stone extraction by balloon, basket or both, with definitive stone extraction as defined by normal cholangiogram performed after stone extraction.Our common practice is to use balloon for CBD stone extraction,however, in stones larger than 1 cm we use basket and in cases of uncertainty about complete stone clearance with the balloon, we add basket cleaning. Moreover, in cases of inability to extract the stone through the papilla we perform mechanical lithotripsy. Exclusion criteria included patients suffering from biliary malignancy,biliary strictures and patients with incomplete stone clearance at the index ERCP procedure.
All procedures were carried out via Duodenoscope (Pentax,Tokyo, Japan). All ERCP examinations throughout the study were performed by an experienced endoscopist with high volume examinations and an over than 20 years’ experience (over 50 0 0 ERCP examinations) in the field of advanced endoscopy. Patients were placed in the prone position and were sedated with intravenous midazolam, fentanyl and propofol according to the decision of the endoscopist. In our study we used MSB-2 × 4 memory soft wire basket (COOK MEDICAL, Bloomington, Indiana, USA), multi-stage stone extraction balloon (Medi-Globe, Rohrdorf, Germany) and mechanical lithotripsy (BML-110A-1, Tokyo, Japan).
All medical records of eligible patients were reviewed and the following parameters were collected: demographic data (age, sex and medical history), ERCP indication (biliary pancreatitis, cholangitis or abnormal cholestatic liver enzymes), the presence of PAD,recurrence rate and the time interval of recurrence, size and number of CBD stones, ERCP interventions for stone extraction (balloon,basket, mechanical lithotripsy, biliary stent and precut technique).Statistical comparison was performed between patients with recurrent CBD stone defined by confirmed stone within the CBD more than 6 months after the index ERCP and patients without recurrence of CBD. The parameters included in the univariate and multivariate analysis were demographic data, clinical and endoscopic characteristics. The CBD stone recurrence was diagnosed according to European Society of Gastrointestinal Endoscopy (ESGE)guidelines using clinical typical presentation, abnormal cholestatic liver function tests with or without radiological evidence of CBD stone [13] . Notably, the policy of our institution includes clinical and laboratory follow-up post ERCP and stone clearance until symptomatic resolution and laboratory tests normalization, but we do not perform extended scheduled follow-up thereafter. All recurrent CBD stones were cleared by second ERCP.
The study protocol conformed to the ethical guidelines ofthe 1975DeclarationofHelsinkiand was approved by the Institution Human Research Committee (0140-18-NHR). Written informed consent was waived by the local Ethical Committee due to the retrospective non-interventional nature of the study.
Statistical analysis
The main aim of the study was to assess demographics, clinical and endoscopic factors that were associated with recurrent CBD stone. Univariate descriptive statistic was used to compare patients with and without recurrent CBD stone. Data were reported as means ± standard deviations for quantitative continuous variables, and frequencies (percentages) for categorical variables. All the assessed parameters that showed statistical significance in univariate analysis model were included in the multivariate logistic regression analysis. Backward selection was used to select the final parameters that were associated with recurrent CBD stone. Regarding the endoscopic characteristics that were significant in univariate analysis (modality of stone extraction model), further multivariate analysis was performed to compare balloon and combined basket and balloon extraction methods to basket extraction by reporting the odds ratio (OR) and the confidence interval (CI). A threshold for statistical significance was set at aPvalue<0.05. All analyses were performed by an experienced statistician using the statistical analysis software (SAS Vs 9.4, SAS Institute Inc., Cary, NC,USA).
Results
Baseline demographics, clinical and endoscopic characteristics
Overall, 949 patients were enrolled, among whom 492 were excluded due to several causes: 17 patients with failed ERCP,63 patients with repeated ERCP due to retained stone, 202 patients with pancreato-biliary malignancies, 57 patients with postoperative leak, 53 patients with stent exchange, and 100 patients lack of data. A total of 457 patients were included in the final analysis ( Fig. 1 ). Forty-two patients (9.2%) had recurrent CBD stone(group A), and 415 patients (90.8%) did not have recurrent CBD stone (group B). The mean ages of patients in groups A and B were 74.4 ± 12.3 and 64.4 ± 20.2 years, respectively. Female was more common in group A (66.7%) than in group B. Similarly, there was no significant difference in medical history between the two groups. Notably, the most common clinical presentation for CBD was abnormal cholestatic liver enzymes in groups A and B (83.3%and 88.2%, respectively; Table 1 ). With regard to cholangiographic findings, 19 patients (45.2%) in group A and 115 patients (27.7%) in group B had multiple CBD stones. Gallbladderinsituwas present in 66.7% and 75.2% of patients in groups A and B respectively at the index ERCP (P= 0.201). Notably, all patients with gallbladderinsituhad gallbladder stones. Moreover, among patients in group A, 14 had resected gallbladder before the index CBD stone presentation, while 15 patients (53.6%) underwent gallbladder resection and 13 patients (46.4%) hadinsitugallbladder between the index and the recurrent CBD stone presentation. The most common endoscopic intervention for stone removal was balloon extraction(54.8% in group A and 63.6% in group B). Interestingly, mechanical lithotripsy was significantly more frequently performed in group A than in group B (11.9% vs. 1.4%,P= 0.001), while there was no difference in biliary stenting and papillary precut technique in both groups. Table 2 demonstrates the endoscopic and cholangiographic characteristics of the study cohort.
Univariate and multivariate regression analysis
In univariate analysis, male sex (OR = 0.49,P= 0.033) was a protective factor for recurrent CBD stone, while endoscopic stone extraction by basket vs. balloon (OR = 2.55,P= 0.005), older age (OR = 1.03,P= 0.003), number of CBD stones (OR = 1.99,P= 0.037), size of CBD stone (OR = 4.06,P= 0.003), and mechanical lithotripsy (OR = 9.22,P= 0.004) were risk factors for recurrent CBD stones. Notably, there was no difference regarding biliary stenting and papillary precut technique (P= 0.325 andP= 0.544,respectively). In multivariate logistic regression analysis, mechanical lithotripsy (OR = 9.73, 95% CI: 1.69-55.89,P= 0.010), basket vs. combined basket and balloon (OR = 18.25, 95% CI: 1.05-318.35,P= 0.046) and older age (OR = 1.02, 95% CI: 1.00-1.05,P= 0.023) were significantly correlated with recurrent CBD stones,while male sex was a protective factor (OR = 0.39, 95% CI: 0.19-0.81,P= 0.012) ( Table 3 ).

Fig. 1. The flow chart of the study cohort. ERCP: endoscopic retrograde cholangiopancreatography; CBD: common bile duct.
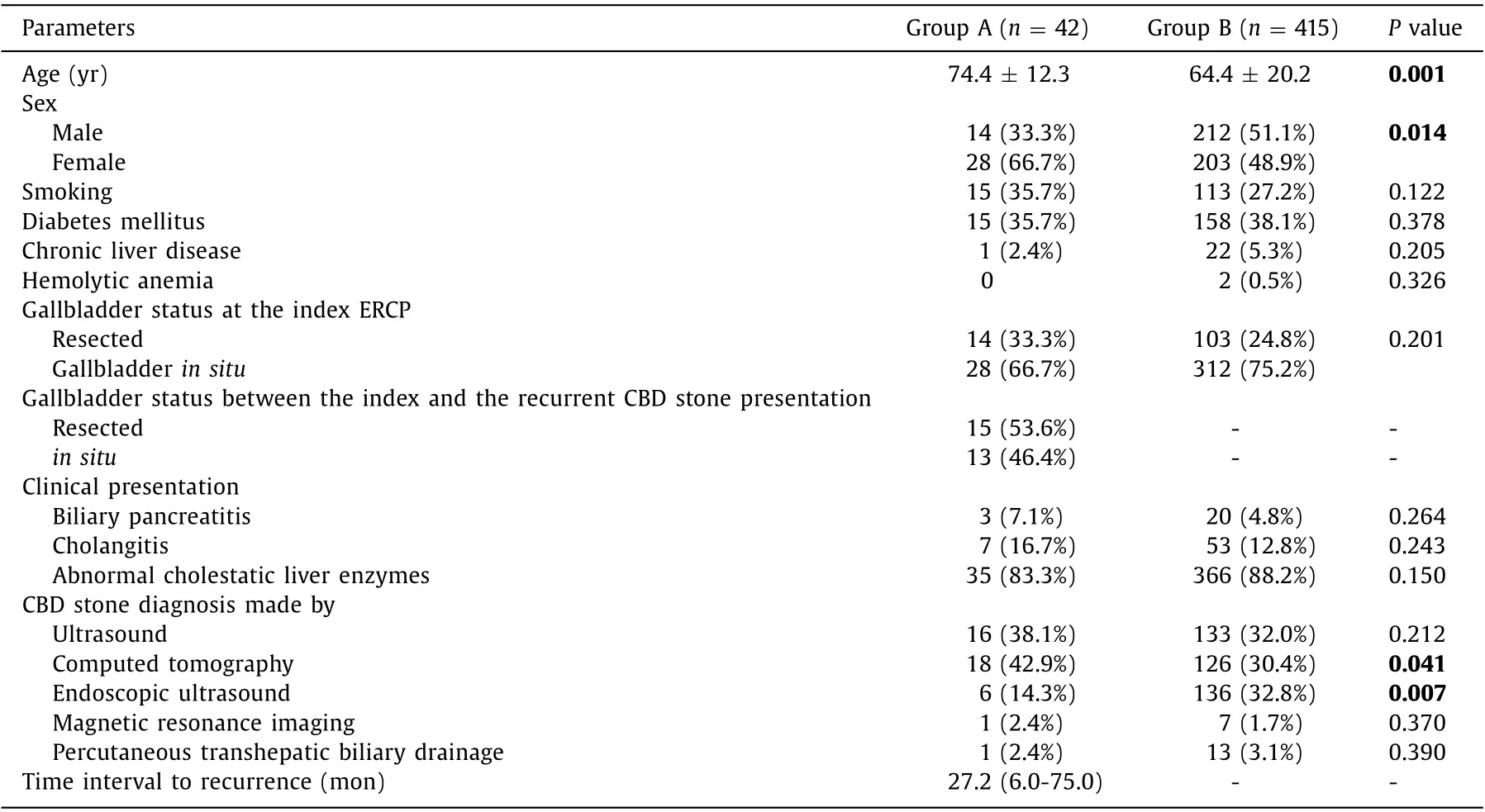
Table 1 Demographics and clinical characteristics of the study cohort.
Discussion
Although most patients with gallstones remain asymptomatic,about 10%-25% do become symptomatic, mostly as a result of stone migration into the CBD [14] . Of these, 1%-2% develop major complications [15] . ERCP represents the treatment modality of choice for CBD stone removal despite its potential complications.One of the major concerns of stone removal is a retained or recurrent stone with its own potential for complications, especially in the elderly comorbid patient, necessitating a repeat ERCP with its risk of sedation and the procedure itself. The recurrence rate of CBD stones in our study was 9.2%, similar to previous retrospective studies reporting CBD stone recurrence rate of 11.1%[16] and 11.97% in patients after EST [17] . Although several studies that aimed to prevent CBD stone recurrence have been reported, a clear strategy to prevent CBD stone recurrence has not yet been confirmed. Our study identified that age was a nonmodifiable risk factor for recurrent CBD stones, and mechanical lithotripsy and basket vs. combined basket and balloon were modifiable procedural-related risk factors, while male sex was a pro-tective factor. Several studies have reported advanced age as a risk factor for recurrent CBD stones after endoscopic therapy [18 , 19] .This association is mainly related to the increase in gallstone formation with increasing age [4] and to the higher rate (2-3 times)of gallstone formation among women [20] .

Table 2 Endoscopic and cholangiographic characteristics of the study cohort.
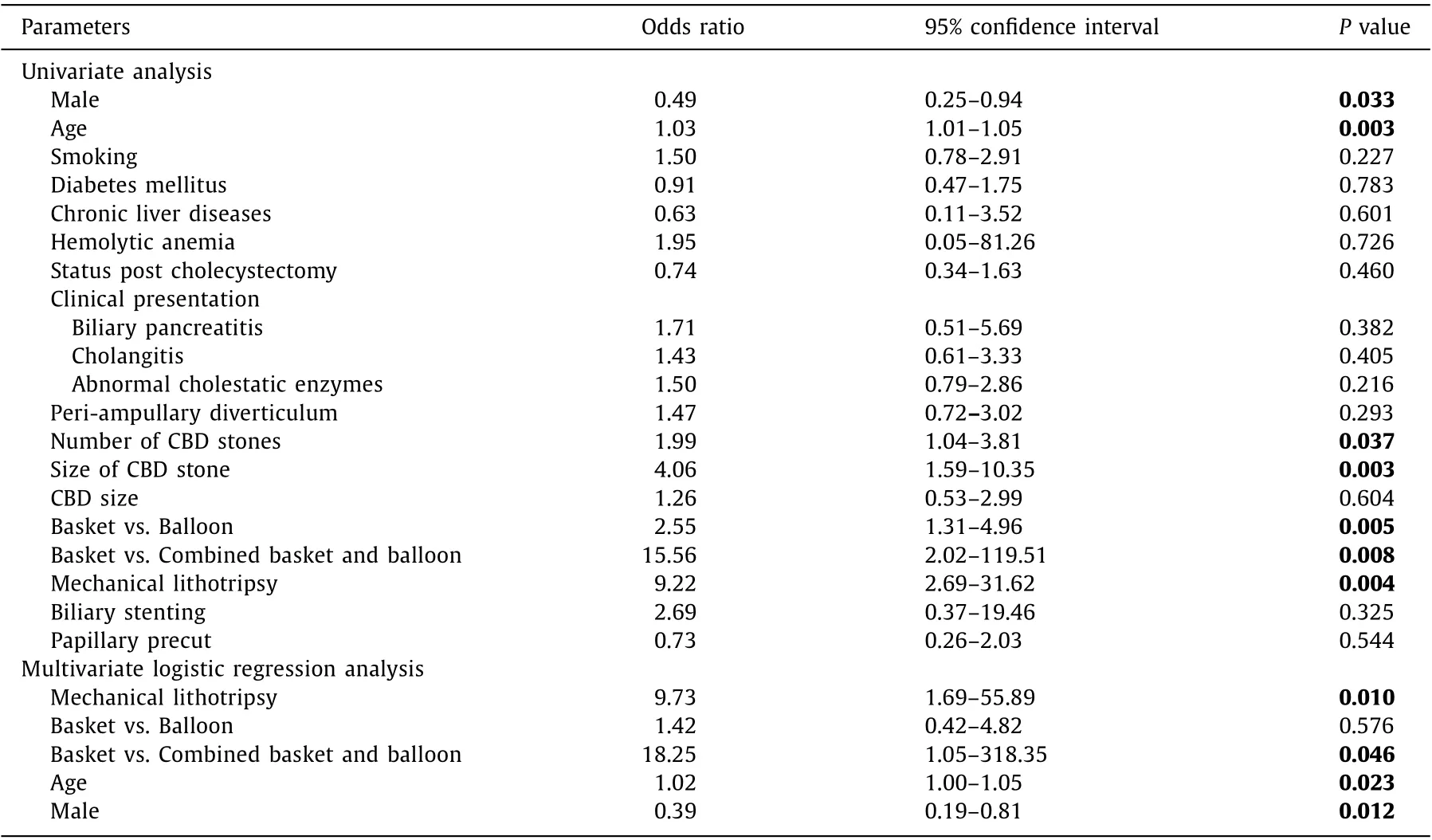
Table 3 Univariate and multivariate analyses of parameters associated with recurrent CBD stone.
Regarding modifiable procedural-related risk factors, a retrospective study investigating risk factors of recurrence after endoscopic treatment of CBD stone and cholecystectomy, reported mechanical lithotripsy as the only modifiable risk factor in addition to unmodifiable risk factors related to stone composition, number and size [21] . Another retrospective study investigating CBD stone recurrence identified mechanical lithotripsy as the only risk factor probably due to residual small fragments, while saline solution irrigation reduced recurrence rate by clearing those fragments [22] . Lu et al. also reported similar results [17] . The possible underlying mechanism for the high recurrence rate after mechanical lithotripsy in our study could be related to retained residual fragments of the crushed stones not extracted at the index ERCP and that did not cause symptoms until they nucleated over time,increased in size and became symptomatic. Our study included patients up to December 2019. Choosing mechanical lithotripsy as the modality for treating large CBD stones was in accordance with the American Society of Gastrointestinal Endoscopy (ASGE) guidelines at that time, where mechanical lithotripsy was the preferred modality; however, our practice changed with the publishing of the new guidelines. Actually, the ASGE guidelines from 2011 [23] recommended considering mechanical lithotripsy or endoscopic papillary balloon dilatation (EPBD) after EST for large, nonimpacted CBD stones refractory to initial extraction efforts, given their effectiveness, ease of use, and acceptable safety profiles. However,the recent ASGE guidelines from 2019 [24] suggest performing EST followed by large balloon dilation rather than EST alone, not mechanical lithotripsy for large bile duct stones [23] .
In its latest version, the ESGE recommends that “an adequate exit for the stone to be removed should be provided according to the papilla, CBD anatomy and stone size” [13] , by EST alone, EPBD alone or a combination of both. However, in difficult stones, “l(fā)imited sphincterotomy combined with endoscopic papillary large balloon dilatation should be considered as the first line approach to remove difficult CBD stones” [13] .
As for CBD stone clearance by basket vs. balloon, we found a trend for stone recurrence using basket extraction and a significant correlation when basket was compared to combined balloon and basket extraction. A previous multicenter randomized controlled trial showed superiority of balloon over basket in extracting CBD stones up to 10 mm [25] , while another multicenter randomized controlled trial showed similar efficacies of both in stones up to 11 mm [26] . However, the ESGE guidelines state that balloon and basket are equally effective and safe for CBD stone removal [13] .The underlying mechanism of the high recurrence rate in the basket extraction group might be related to the reported limitation of basket in complete retrieval of small CBD stones, which leads to the persistence of residual small stones that enlarge over time to cause symptomatic biliary obstruction [27] .
In our study, one might postulate that the size of EST could affect the efficacy of balloon and basket in complete stone extraction. However, as ERCP examinations were performed by an experienced gastroenterologist with a high procedure volume, it can be assumed that EST is uniform in the patient cohort (including patients with balloon or basket stone clearance), and that variation in EST size was negligible. However, further studies are needed to address this issue. Previous study showed that gallbladder leftinsituwith stones and large bile duct size were a significant risk factor for recurrent CBD stone [28] . In our study, the effect of impaired sphincter function on CBD stone recurrence rate was negligible owing to the fact that patients in both groups underwent EST. In addition, the rate of patients who had gallbladderinsituand CBD size were similar in both groups, leading us to conclude that the effect of these factors in CBD stone recurrence is not significant, especially because of the EST. Still, our results regarding gallbladderin situshould be taken with caution since we did not have enough data regarding the presence of gallbladder stones. Therefore, our results might underestimate this parameter as a risk factor for recurrence.
Our study has several limitations. The first is the single-center population and the retrospective nature of data collection. The second is the relatively small number of patients who underwent mechanical lithotripsy which might underestimate the results. The third is that we may have overlooked asymptomatic CBD stone recurrence since we included symptomatic cases only. The fourth is that although we included a large number of patients in the entire cohort, the sample size of patients with recurrent CBD stone is relatively small. Lastly, the inability to calculate hazard ratio applying Cox regression model due to the lack of follow-up for patients without CBD stone recurrence is also a limitation. As we are the only tertiary center in our region performing ERCP, most patients with recurrent CBD stone would probably have been referred to us,therefore, the statistical bias of not having extended follow-up is likely to be minor. On the other hand, the strength is the relatively large cohort of patients included in our study.
In conclusion, in our cohort the prevalence of CBD stone recurrence after ERCP and stone removal was 9.2%, similar to previous studies exploring this topic. Interestingly, we could, by multivariate analysis, identify both risk and protective factors for CBD stone recurrence. Further studies on larger cohort of patients are warranted to confirm our results.
Acknowledgments
None.
CRediT authorship contribution statement
Wisam Sbeit : Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision,Validation, Visualization, Writing - original draft, Writing - review& editing. Anas Kadah : Data curation, Formal analysis, Resources.Matta Simaan : Data curation, Formal analysis. Amir Shahin : Data curation, Formal analysis, Resources. Tawfik Khoury : Conceptualization, Data curation, Formal analysis, Investigation, Methodology,Project administration, Supervision, Validation, Visualization, Writing - original draft, Writing - review & editing.
Funding
None.
Ethical approval
The study protocol conforms to the ethical guidelines ofthe 1975DeclarationofHelsinkiand was approved by the Institution Human Research Committee (0140-18-NHR).
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
 Hepatobiliary & Pancreatic Diseases International2022年1期
Hepatobiliary & Pancreatic Diseases International2022年1期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Targeting pancreatic ductal adenocarcinoma: New therapeutic options for the ongoing battle
- How open is the therapeutic horizon for pancreatic cancer patients?
- Terlipressin versus placebo in living donor liver transplantation
- Fas -670 A/G polymorphism predicts prognosis of hepatocellular carcinoma after curative resection in Chinese Han population
- Meso-Rex bypass for the management of extrahepatic portal vein obstruction in adults (with video)
- The effect of SphK1/S1P signaling pathway on hepatic sinus microcirculation in rats with hepatic ischemia-reperfusion injury