
Overview of point-of-care ultrasound in diagnosing intestinal obstruction
2022-03-02 06:46:28RuitingLiYueZhaoXiaojingZouHuaqingShuTingZhouShangwenPanXuehuiGaoHaiyanHuangHongLiuYouShang
World Journal of Emergency Medicine 2022年2期
Rui-ting Li, Yue Zhao, Xiao-jing Zou, Hua-qing Shu, Ting Zhou, Shang-wen Pan, Xue-hui Gao, Hai-yan Huang,Hong Liu, You Shang
1 Department of Critical Care Medicine, Institute of Anesthesia and Critical Care Medicine, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430022, China
2 Department of Critical Care Medicine, Jin Yin-tan Hospital, Wuhan 430048, China
Intestinal obstruction (IO), which refers to a partial or complete blockage of the intestine, is an emergency gastrointestinal disorder commonly seen in the intensive care unit (ICU) and emergency department and associated with high morbidity and mortality.Common etiologies of IO include adhesions, hernias,intussusception, foreign bodies, ischemia, tumors,etc. Delay in the diagnosis and management of IO is associated with higher mortality due to complications such as bowel necrosis, perforation, sepsis, and septic shock.IO can be divided into small bowel obstruction(SBO) and colonic obstruction (CO). In SBO, 74%of cases are caused by adhesions, which may respond to conservative management. It is critical to identify which of those cases may progress and require emergent surgical intervention with the help of the diagnostic and assessment tools. In contrast to SBO, most cases of CO demand surgery. In this instance, appropriate assessment tools are required to define the location of the obstruction, which will assist in the proper surgical procedure.
Point-of-care ultrasound (POCUS), as a noninvasive and radiation-free bedside diagnostic tool,has the desirable characteristics of speediness,repeatability, accuracy, and convenience. It is beneficial in critical decision-making and rapidly guiding further interventions.In addition, POCUS can be easily acquainted by clinicians, especially the physicians of emergency department and critical care medicine after professional training. As a result,POCUS has become a life-saving assessment and diagnostic tool in the early diagnosis and timely management of patients with IO.
At recent study has shown that POCUS can accurately diagnose and determine the pathogenesis of IO, with results comparable to computed tomography(CT).The use of POCUS in patients with suspected IO reduces the cost and avoids the inconvenience and radiation exposure from CT scans and X-rays.Growing interest in POCUS as a first-line imaging modality for IO has been seen recently.However,to date, there remains no standard practice guideline for POCUS in diagnosing IO. Here, we provided an overview of the use of abdominal POCUS in the diagnosis and assessment of IO.
IO ultrasound technique
Abdominal ultrasound examination of the gastrointestinal tract is performed in the supine position, using a low frequency(3-5 MHz) convex abdominal transducer. A high frequency(> 10 MHz) linear transducer is used in thin patients or for obtaining high-resolution imaging or assessment of delicate structures.The examination is conducted in a clockwise direction from the epigastrium to the pelvis, and then the dilated intestine is followed to look for the site of IO. Appropriate abdominal compression may be applied to displace gas and bowel contents during the examination, making the ultrasound image clearer. The main observations are as follows: intestinal morphology,peristalsis, intestinal diameter, and intraluminal contents,intestinal vascularity, thickness and location of the intestinal wall, characteristics of obstructed mass,ascites, and enlarged lymph nodes. In the absence of particular circumstances, such as significant abdominal abnormalities, we will start with the abnormal site, and a three-step examination technique is suggested. Step 1:upper abdominal stomach assessment; step 2: left midabdominal jejunum and descending colon assessment;step 3: right lower abdominal terminal ileum and ascending colon assessment (Figure 1).
Accuracy of POCUS in diagnosing IO
Conventionally, the abdominal X-ray and abdominal CT examination are used to diagnose IO. Abdominal plain radiography is mainly used as an initial imaging tool. It has an accuracy of more than 50% in diagnosing IO. At present, abdominal CT remains the gold standard of imaging modality in confirming IO, which has the advantage of determining the cause and level of obstruction.In patients with IO, the upright views of abdominal X-ray and CT scanner demonstrate air-fluid levels in a stepladder distribution with multiple loops of bowel dilatation. Coupled with a non-dilated distal colon and rectum, IO would be highly suspicious. However,these imaging modalities are costly, induce radiation exposure, and take longer time to perform, which may lead to potential delay in diagnosing IO.
POCUS is fast, repeatable, without radiation exposure, and has a sensitivity of 90.0%-92.4% and specificity of 96.0%-96.7% in IO diagnosis.It can also be used to evaluate patients' volume and hemodynamic status. But, it is operator-dependent and limited by gastrointestinal gas and physical conditions of the patient (e.g., obesity, pregnancy).However, with adequate training and experience, POCUS can be readily performed by clinicians of the emergency medicine and critical care department. The reported accuracy of diagnosing IO by emergency physicians was comparable to that of professional radiologists.Jang et alhave reported that the sensitivity and specificity of ultrasound are far superior to that of X-ray in diagnosing IO. Furthermore, when compared with abdominal CT, no difference has been observed in the sensitivity and specificity with ultrasound, while the sensitivity of POCUS is dependent of patient's characteristics and the experience of the performing physician.When ultrasound findings are negative or clinically inconclusive, CT may be better at guiding further management.
Transabdominal ultrasound also has advantages when determining the etiology of IO. The most frequent cause of SBO is postoperative intestinal adhesions.In diagnosing adhesive SBO, ultrasound examination has higher sensitivity when compared to the plain X-ray. A recent study has reported that transabdominal ultrasonography is superior in the establishment of adhesive SBO during hospitalization and allows the dynamic examination, which guides the management and decision for surgical intervention.In IO, due to acute arterial mesenteric ischemia, ultrasound provides information on arterial blood flow. In CO, tumors are the main pathogen, which are sonographically characterized by segmental hypoechoic thickening bowel wall with irregular margins or as a mass.On the other hand, in intussusception, the typical sonographic findings are the doughnut sign or multiple-concentric-rings sign in the transverse scan, and the sandwich or fork sign in the longitudinal scan.
Due to its high accuracy and specificity, POCUS has been recommended as the primary assessment tool for diagnosing and managing patients with suspected IO,especially among pregnant women and in emergency circumstances where CT is not available. When coupled with a CT scan, the accuracy of POCUS on the location,etiology and severity of obstruction is enhanced.
Diagnostic criteria of IO by POCUS

Figure 1. The sequence of ultrasonographic examination in patients suspected to intestinal obstruction.
Although mounting evidence has shown high sensitivity and specificity of POCUS in diagnosing IO, there is little uniformity in the diagnostic criteria to date. Diagnosing IO with POCUS relies on finding intestinal morphology and function changes.However,sonographic features of SBO and CO have been variably reported, as outlined in Figure 2.
Commonly, there are five characteristics or signs on POCUS that diagnose and stage SBO: the presence of dilated bowel (> 2.5 cm) (Figure 3A, B); abdominal A-lines (gastrointestinal intraluminal air) (Figure 4A);abnormal bowel peristalsis (Supplementary Video 1);interloop free fluids (Figure 4C); and thickened bowel wall (> 3 mm) (Figure 3A, B).Of these, the presence of dilated bowel provides high sensitivity (>90%) and specificity (> 80%) in diagnosing SBO, which is defined as a small bowel diameter of > 2.5 cm (from the outer wall to outer wall).On the other hand,the gastrointestinal tract is also a gas-bearing organ caused by gastrointestinal paralysis during SBO. The presence of the abdominal A-lines, which represents the gas filling of the intestine, is often accompanied by signs of dilated and fluid-filled loops. Although clinical data are limited, the presence of the abdominal A-lines is thought to provide average sensitivity but very high specificity for the diagnosis of SBO.When identifying abnormal bowel peristalsis on ultrasound,the sensitivity and specificity for SBO have been reported as 100% and 67.4%, respectively.On the contrary, the presence of interloop free fluids provides the lowest sensitivity of 4.5% but a high specificity of 88.4%.All in all, for the diagnosis of SBO, POCUS findings of dilated bowel loops with or without abdominal A-lines are essential, which indicates the obstacle for the progression of intestinal contents and hence a pathognomonic sign of bowel obstruction.Combined with abnormal intestinal peristalsis,intraperitoneal fluid or parietal and valvulae conniventes modification, the diagnostic accuracy of bowel obstruction based on ultrasound is increased(Figure 2).
Previous clinical studies have also reported that POCUS offers accurate etiology and location of CO.In particular, ultrasound is valuable in diagnosing proximal CO but less accurate when the obstruction is at the low recto-sigmoid region, given that the tumors in this region may manifest with other symptoms than obstruction.Nevertheless, the diagnostic criteria for CO on ultrasound remain ill-defined. In adults,the average diameters of the left and right hemicolon measure approximately 4 cm and 5 cm, respectively.Typically in CO, the dilated large intestine (> 4.5 cm) with echogenic contents is seen (Figure 3C, D),usually with an abrupt transition from the dilated colon to the undilated segment of the colon. The thickened plicae circulares of the colon typically measure up to 2 mm (Figure 3C, D). Peristalsis is often absent or subtle (Supplementary Video 2). Due to the abundance of gas in the obstructed colon, it is often impossible to obtain a complete overview and accurately measure the diameter of the dilated colon. Still, the presence of abdominal A-lines (Figure 4B) may indicate the range and location of colonic flatulence, in addition to stagnated liquid and solid stools in the colon.Therefore, to diagnose CO based on ultrasound, dilated large intestine (> 4.5 cm) (Figure 3C, D) in addition to abdominal A-lines(Figure 4B) is essential. However, the abdominal A-lines resulting from flatulence may significantly disturb the ultrasound examination. Moreover, in CO,abnormal intestinal peristalsis (Supplementary Video 2) or thickened plicae circulares (> 2 mm) (Figure 3C,D) may also be observed (Figure 2).
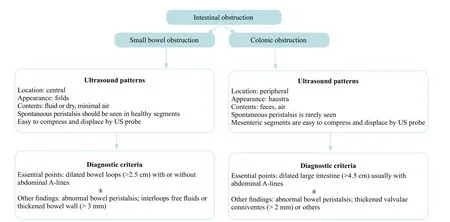
Figure 2. The ultrasound criteria for the diagnosis of small bowel obstruction and colonic obstruction.
Location of obstruction and etiology
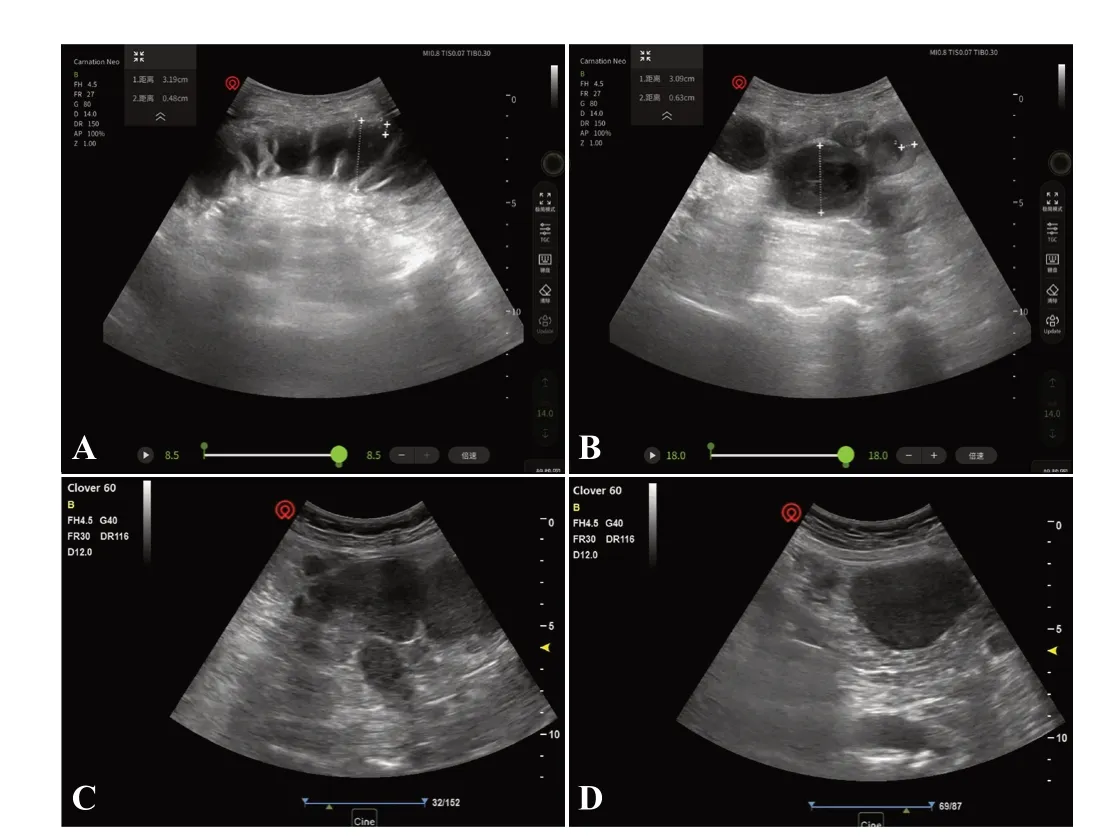
Figure 3. A 65-year-old male patient with previous abdominal surgery.Ultrasound image long (A) and axial (B) evaluation of the dilated small bowel (the distance 1) and thickened bowel wall (the distance 2). A 69-year-old female patient with coronavirus disease 2019.Ultrasound image long (C) and axial (D) evaluation of the dilated colon. These images suggested intestinal obstruction.
The location of IO can be determined by the transition point using ultrasound. Through scanning distally along the dilated intestine, the junction of the distended distal bowel and the collapsed proximal bowel represents the transition point. However, this is only a rough assessment of the approximate location of IO but does not indicate the specific area of the obstruction.For instance, if the transition point is in the right iliac fossa and the lower abdomen, the location of obstruction is mainly in the distal and terminal ileum. If the transition point is located at the left upper quadrant of the abdomen, the location of obstruction is likely in the jejunum and the proximal ileum. Furthermore, the location of obstruction can also be determined by evaluating the characteristics of plicae circulares, given that there are more plicae circulares in the dilated jejunum than that in the dilated ileum.
Colon cancer is the most common cause of CO.When a transition point or tumor mass is identified on a systematic scan of the colon (from the cecum to the rectum), it often indicates the location of CO.Volvulus represents another main cause of acute CO,typically characterized by a long sigmoid colon or mobile cecum. In the circumstance, CT is superior to ultrasound in diagnosing CO.
Limitations of POCUS in obstruction evaluation
Although POCUS has considerable advantages in diagnosing IO with an accuracy of more than 50%, it has some limitations. Firstly, POCUS is more accurate in diagnosing complete IO rather than incomplete IO.Secondly, the transition point can be challenging to locate accurately between the dilated and compact loops of the intestine by ultrasound. Also, the etiology of IO may not be correctly determined by ultrasound alone.
Discussion
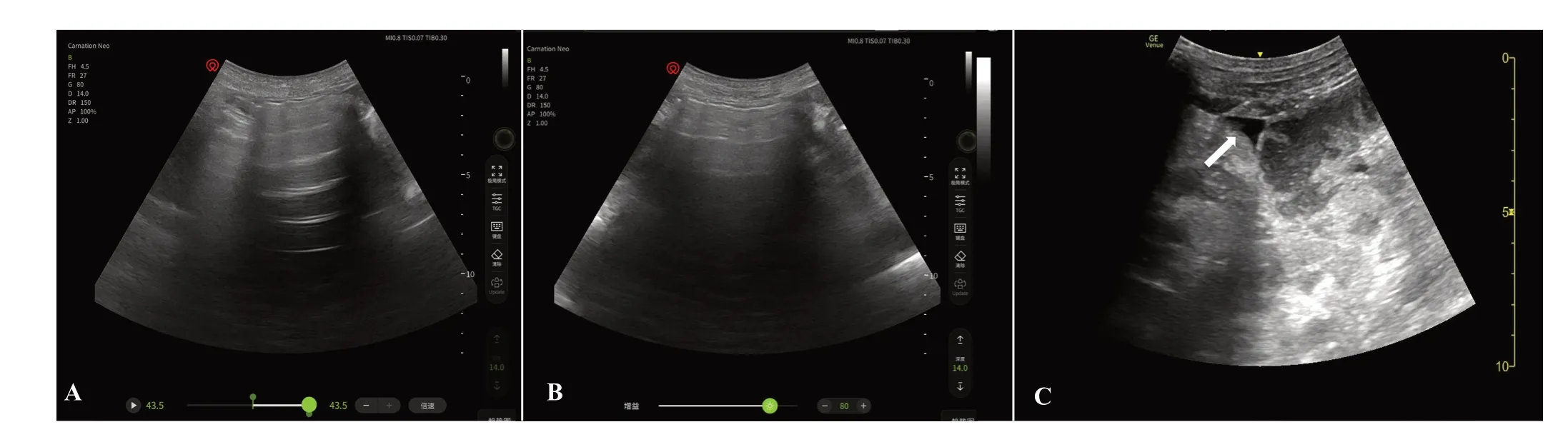
Figure 4. Ultrasound images (A, B) of intestinal flatulence of the patients in Figure 3. The horizontal lines above the abdominal wall are abdominal A-lines. A 60-year-old male patient with diffuse peritonitis. Ultrasound images (C) of interloop free fluids (white arrow) of the patient.
The POCUS approach has been commonly applied in a variety of emergent conditions, including the identification of shock and respiratory failure, and the management of circulatory volume status. Moreover,POCUS has been used to diagnose patients with suspected IO and found to have high specificity and accuracy.
Although CT remains the gold standard for the diagnosis of IO, it is associated with radiation exposure, increased risk of outside inspections,increased cost, and delayed diagnosis. In addition,CT may be limited in locating the transition point between the dilated and collapsed proximal bowel loops of IO.Comparatively, POCUS is advantageous given that it is cheaper, can be performed at the bedside with easy accessibility,allows rapid diagnosis, and guides the management of IO.Recent studies have also demonstrated no significant difference between ultrasound and CT in the accuracy of detecting IO. Furthermore, POCUS allows regular dynamic evaluation of IO, which appraises the progress or deterioration of IO in realtime. Nevertheless, CT allows for a better systematic overview and is an ideal complement to POCUS.Other imaging modalities (X-ray and magnetic resonance imaging [MRI]) have also been proposed to identify, stage, and define the cause of IO. Given its easy access, plain X-ray is often the first choice in patients suspected to IO. However, it has poor sensitivity and specificity.On the other hand, MRI is not universally and readily available in clinical practice. Furthermore, ultrasound appears superior to MRI for diagnosing IO.
The roles of POCUS in clinical practice and its accuracy in the evaluation of IO have been well described in the literature.In this paper, we summarized the diagnostic criteria of ultrasound for SBO and CO, pertaining to the morphological and functional characteristics of bowels. Having clear criteria would help further in making systematic and accurate clinical judgments. Although POCUS can determine the diagnosis, the site, and etiology of IO, excessive intestinal gas, obesity, or pregnancy may compromise the ultrasonographic imaging, which can be overcome by graded compression and examination in the coronal plane and decubitus positions.
For the assessment and diagnosis of IO, POCUS is a valuable tool with high sensitivity and specificity comparable to CT, X-ray and MRI. In addition, POCUS can be performed by non-radiological clinicians that help to provide fast, convenient, and repeatable assessments in a complicated clinical setting. These characteristics of POCUS are beneficial in critical decision-making and guide emergent surgical interventions.
None.
Not needed.
The authors declare that they have no conflicts of interests.
RTL, YZ wrote the manuscript; RTL produced the figures; RTL, XJZ, HQS, TZ, SWP, XHG gathered information;HYH, HL, YS revised the manuscript. RTL and YZ are co-frist authors.
All the supplementary files in this paper are available at http://wjem.com.cn.