
Layperson’s performance on an unconversant type of AED device: A prospective crossover simulation experimental study
2022-03-02 06:46:28ChaoyuLeiHengweiQinXuejieDongJialinYouLinZhang
World Journal of Emergency Medicine 2022年2期
Chao-yu Lei, Heng-wei Qin, Xue-jie Dong, Jia-lin You, Lin Zhang
1 Shanghai Jiao Tong University School of Medicine, Shanghai 200025, China
2 Department of Global Health, School of Public Health, Peking University, Beijing 100191, China
3 School of Public Health, Shanghai Jiao Tong University School of Medicine, Shanghai 200025, China
4 School of Nursing, Shanghai Jiao Tong University, Shanghai 200025, China
KEYWORDS: Automated external defibrillator; Layperson; Cardiac arrest; Simulation
INTRODUCTION
For patients with out-of-hospital cardiac arrest(OHCA), each minute of delay in defibrillation leads to a 10% reduction in survival.The wide dissemination of automated external defibrillators (AEDs) has enabled bystanders to save OHCA patients.Furthermore,it was reported that a 70% survival rate and favorable neurological outcome could be achieved with the use of an AED.
The AED was designed with colloquial and distinct instructions to ensure that the public could operate it without any previous training. Of note, some studies have shown that the laypersons’ ability to understand the instructions and efficiently operate AEDs still need to be enhanced.It has been reported that laypersons are likely to disregard operation steps such as removing clothes,placing the electrodes, and resuming cardiopulmonary resuscitation (CPR) after the shock.AED training is a good way to cope with improper operation, especially for the reduction of operation time.However, laypersons usually operate only one type of AED in training but encounter distinctive ones in reality.
Although various models of AED devices are based on consistent basic principles, discrepancies have been presented in several aspects, including poweron mechanism, pad design, visual prompts, and voice instructions.Many researchers have found that distinctive AED device features impact the performance of laypersons; different AED voice prompts bring about a longer time to resume CPR.Therefore, it is of vital significance to investigate whether people trained with one type of AED can effectively operate other types of AEDs.This begs the question whether they perform differently using a new type of AED and if it is necessary to provide training for different types of AEDs.
Thus, we carried out this crossover simulation experimental study to explore whether the general public participants who have trained with one type of AED could effectively operate another AED with different features.
METHODS
Study design
This was a prospective, crossover simulation study conducted from September 10, 2018 to May 20,2019. Ethical approval for this study was given by the Joint Research Ethics Board of the Shanghai Jiao Tong University School of Public Health and Nursing(SJUPN-201714). All participants were informed about the aim of this study, both verbally and through written informed consent.
Study population
Participants were undergraduate students aged 18-24 years from Shanghai Jiao Tong University with prior experience of the “WeCan CPR” training.This training is a Chinese program aimed at offering practical and basic CPR training for potential bystanders.During the training, participants were randomly assigned to operate one type of AED (AED1,LaerdalPhilips AED Trainer 2, Norway; AED2, ZOLLAED Plus Trainer 2, USA). The details of the AED training were described in a previous study.
Discrepancy of the two types of AED devices
With diverse features, AED1 and AED2 represent the two main AED device models. They varied mainly in the power-on mechanism, pad design, visual prompts,and voice instructions (Table 1). The on/off button was inside the zippered box in AED1, while it was outside of the clamshell box in AED2. The electrode pad was a two-piece type packed in plastic bags inside the zippered box in AED1 with a power plug requiring manual connection. On the other hand, a one-piece electrode pad in a clamshell box without an individual package with a pre-connected power plug was seen in AED2. As for voice instructions, AED1 emphasized the existence of a schematic diagram of the electrode placement while AED2 did not. Also, AED1 clearly commanded resuming CPR and sounded alert tone after shock delivery, while AED2 required the operator’s own decision.
Study procedures
The students’ performance on two types of AEDs was evaluated in two phase tests: (1) phase I test, at the end of the “WeCan CPR” training; and (2) phase II test,at the 6-month follow-up. Participants were randomly assigned to operate one type of AED in both two phases by means of random number method. In the phase I test,subjects were randomly divided into two groups (AED1 group and AED2 group) according to the AED type used in training. In the phase II test, subjects were further randomly divided into four groups and formed two switched subgroups according to the sequence of AED use in the phase I and phase II tests (Switch A: AED1-1 group vs. AED2-1 group; Switch B: AED2-2 group vs.AED1-2 group). For example, participants in the AED1-2 group operated AED1 in the phase I test and AED2 in the phase II test.
AED devices operation performance evaluation
The performance evaluation of the AED devices was conducted among the participants individually in an experimental room. A manikin (Resusci AnneQCPR,Laerdal Medical, Norway) was placed on the floor to simulate an OHCA patient. The students were told that they needed to operate the AED device besides of the manikin’s feet to perform defibrillation as the way they believed to be correct. To better simulate a realistic OHCA patient, a T-shirt and a zippered jacket were dressed on the manikin and provided barriers to electrode placement. Setting the AED near the feet of the manikin was done to examine whether participants were able to set the AED on the shoulder as the correct placement in the test. During the simulation process,no additional prompts were delivered other than the AED device’s instructions. The evaluation was started when participants were ready to operate the AED and terminated when CPR was performed after the first AED shock delivery or when the subject expressed a desire to stop.
Data collection and outcome measures
The AED operation performance of the participants was recorded using a camera. Participants’ behaviors were documented based on eight key actions, including: (1)power on (on/off button was pressed and voice instructions were provided); (2) full chest baring (the jacket and T-shirt were both removed from manikin to ensure that electrodes were not covered by clothes during electrodes placement);(3) correct electrodes placement (both electrodes attached within 5 cm from the recommended electrode positions,at the basis of full chest baring); (4) clear during rhythm analysis (participants didn’t touch the manikin during rhythm analysis); (5) defibrillation prompt (button lighting or the defibrillation signal was provided); (6) shock delivery(shock button was pressed and the voice confirmation of shock delivery was provided); (7) clear during shock delivery (participants didn’t touch the manikin during shock delivery); and (8) resuming CPR after shock (participants conducted at least one compression on the manikin’s chest after shock delivery). Operation fulfilling steps (1)-(7)simultaneously was defined as successful defibrillation.
Critical time parameters recorded among participants achieving successful defibrillation were as follows: (1)time to power on (evaluation start to power on); (2)time to defibrillation prompt (from evaluation start to defibrillation prompt); (3) time to shock delivery (from evaluation start to shock delivery); (4) time to resume CPR (from evaluation start to resuming CPR); (5) time expense of baring the chest (from the start of clothing removal to achievement of full chest baring); (6) time expense of electrode placement (from attachment of electrodes to completion of electrode placement); (7)time interval from defibrillation prompt to shock delivery(from defibrillation prompt to defibrillation button pressed); and (8) time interval from shock delivery to resume CPR (from defibrillation button pressed to first chest compression initiated).
Primary outcomes included the proportion of successful defibrillation and shock delivery time within participants achieving successful defibrillations.Secondary outcomes were the proportion of CPR resumption, the proportion of baring the chest, the proportion of correct electrode placement, the proportion of clear during rhythm analysis, the proportion of clear during shock delivery, time expense of baring the chest,time expense of electrode placement, and time interval from shock delivery to resume CPR.
Statistical analysis
Data are presented as frequencies with percentages for categorical variables and mean ± standard deviation or median (interquartile range) for continuous variables.Normal distribution was confirmed using the Kolmogorov-Smirnov test. Dichotomous data were compared using the Chi-square or Fisher’s exact test and continuous data with ANOVA. Comparisons of continuous variables between groups were analyzed using the Mann-Whitney-test or Student’s-test, depending on the data distribution. Finally,comparisons of rates were conducted using the Chi-square analysis. Statistical significance was set at<0.05, and all data analyses were conducted using SPSS for Mac(version 25.0, IBM). Photographs recording the conditions of manikins and electrode placement were processed using ImageJ for Mac (version 1.47, NIH).
RESULTS
Participant characteristics
A total of 224 students were recruited for this study(Figure 1). Sixty-five participants were excluded due toloss to follow-up (=61) and document error (=4). The age of participants was 19.89±1.50 years and 44.7% were male. No significant differences were found between the AED1 and AED2 groups in terms of age and sex (both>0.05).
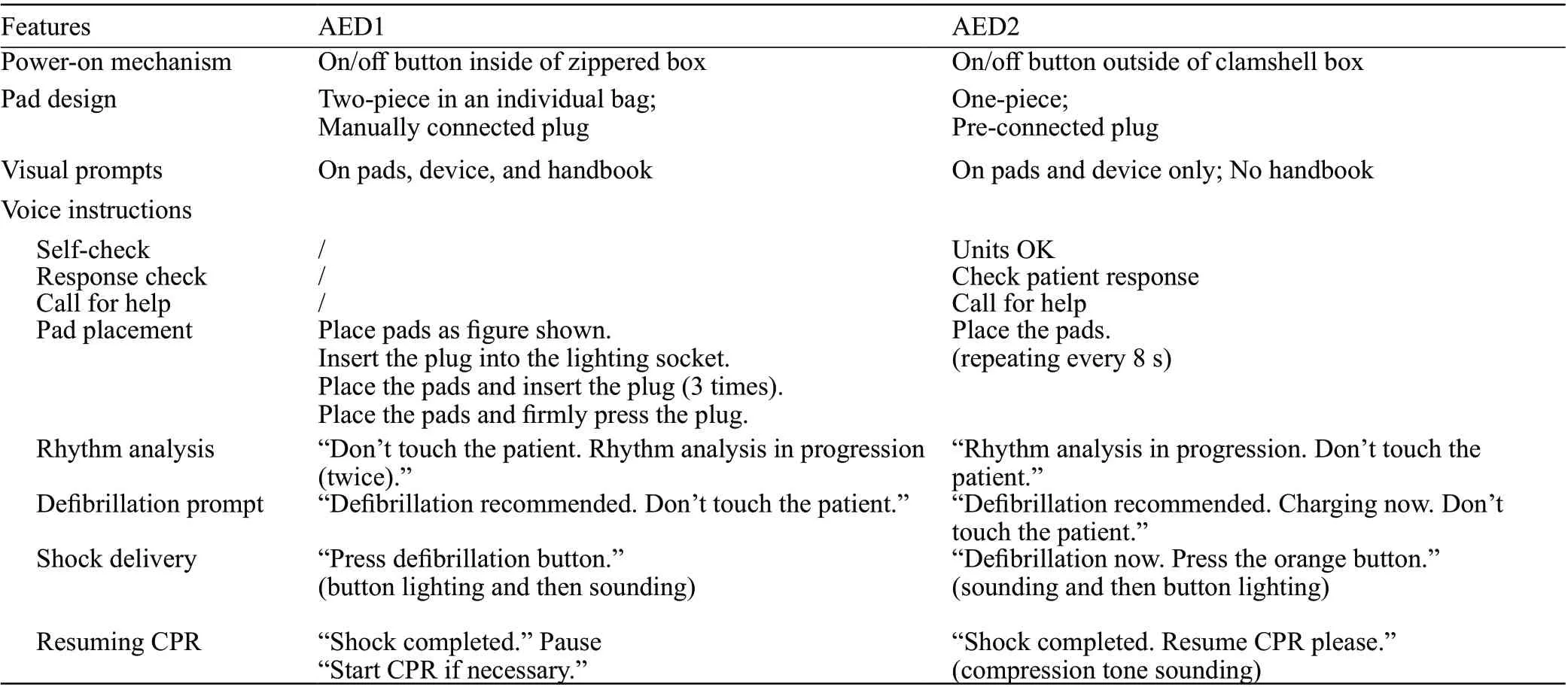
Table1. Features of AED1 (Laerdal? Philips AED Trainer 2) and AED2 (ZOLL? AED Plus Trainer 2)
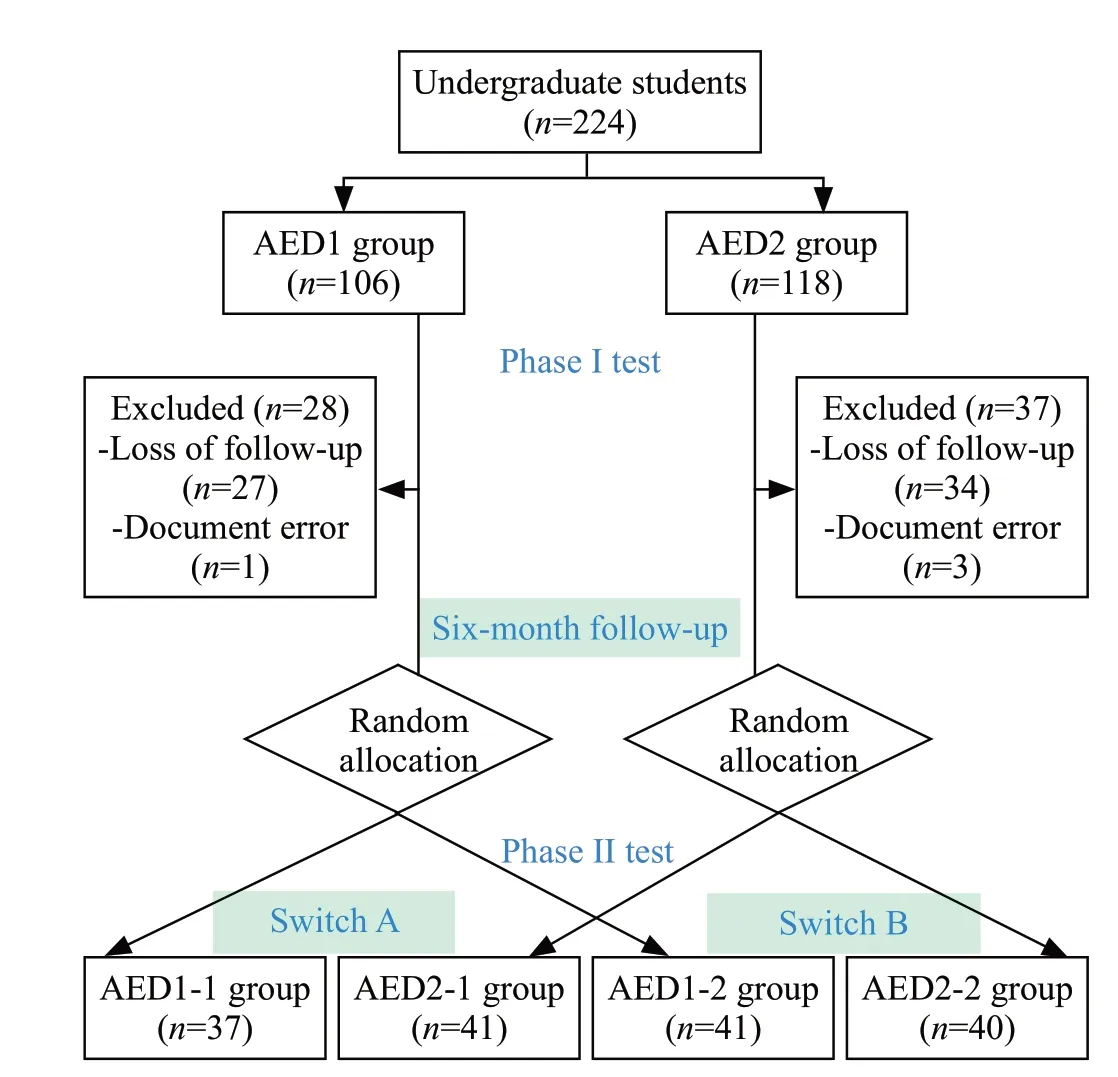
Figure 1. Flow diagram of the participants. AED1-1: operating AED1 in phase I test and AED1 in phase II test; AED2-1: operating AED2 in phase I test and AED1 in phase II test; AED1-2: operating AED1 in phase I test and AED2 in phase II test; AED2-2: operating AED2 in phase I test and AED2 in phase II test; Switch A: comparison between AED1-1 group and AED2-1 group; Switch B: comparison between AED1-2 group and AED2-2 group; AED: automated external defibrillator.
Correct key actions in AED operation
In the phase I test, a significantly higher proportion of successful defibrillations was found in the AED2 group than in the AED1 group (AED1 group 62.8% vs.AED2 group 90.1%,<0.001). However, the rate of clear during rhythm analysis in the AED1 group was statistically lower than that in the AED2 group (79.5%vs. 98.8%,<0.05). The rate of chest barring (98.7% vs.100%,=0.31), correct electrode placement (80.8% vs.91.4%,=0.05), and clear when defibrillation (97.4% vs.98.8%,=0.54) did not statistically differ between the two groups.
In the phase II test, there was no statistical difference in the rate of successful defibrillation in Switch A(AED1-1 group 51.4% vs. AED2-1 group 36.6%,=0.19) or Switch B (AED2-2 group 72.5% vs. AED1-2 group 53.7%,=0.08) (Figure 2A). Moreover, the rate of chest barring, correct electrode placement, clear during rhythm analysis, and clear when defibrillation between the two switches was not statistically significant (Figure 2B-E).
Critical time parameters in successful defibrillations
In the phase I test, it took a longer time to deliver successful shock for participants in the AED1 group than in the AED2 group (73 [64-80] s vs. 60 [54-70]s,<0.001). Three key time parameters of the critical actions were remarkably shorter in the AED2 group than in the AED1 group, including time to power opening(38 [18.5-52.5] s vs. 23 [10-33.5] s,=0.02), time to defibrillation prompt (71 [61.5-77.5] s vs. 59 [53-69] s,=0.03), and time to resuming CPR (83 [74-93] s vs. 66[59-75] s,=0.03).
In the phase II test, the median shock delivery time within participants achieving successful defibrillation statistically differed both in Switch A (89 [81-107] s vs.124 [95-135] s,=0.01) and Switch B (68 [61.5-81.5]s vs. 95.5 [55-131] s,<0.001) (Figure 3A). In the two switched subgroups, a significantly shorter time was noted in the AED operation time, including time to power opening(Switch A: 62 [53-81] s vs. 98 [65-111] s,=0.02; Switch B: 29 [11-37.5] s vs. 53 [22-98.8] s,<0.01), time to defibrillation prompt (Switch A: 87 [78-102] s vs. 120[90-131] s,=0.01; Switch B: 65 [58.5-79.5] s vs. 94 [72-123.3] s,<0.001), and time to resuming CPR (Switch A:98 [90-120] s vs. 137 [105-150] s,=0.02; Switch B: 72[67-86.5] s vs. 119.5 [80.8-143.5] s,<0.001) (Figure 3BD). There were no statistical differences in the other time measures between the two switched subgroups (Figure 3EH) except Switch B in Figure 3F.
DISCUSSION
It has been confirmed that commercially available AEDs with different features have an impact on the performance of laypersons.Since laypersons would not always encounter AEDs in real life that are the same as the ones they used in the training process,whether training with one type of AED can enable them to use other AEDs efficiently should be investigated.To our knowledge, this crossover experimental study was the first study targeting college students trying to determine whether the performance of the people trained with one type of AED would be affected when using another AED with varying features. Our study suggested that people who were trained with one type of AED could operate a new type of AED effectively, although the operation time would be prolonged.

Figure 2. Participants’ AED operation behaviors (n=159). A: percentage of successful defibrillation; B: percentage of fully baring the chest;C: percentage of correct electrodes placement; D: percentage of clear during rhythm analysis; E: percentage of clear during defibrillation; F:percentage of resuming CPR after shock. *P<0.05; **P<0.01.
Our study showed that the variety of AEDs could affect laypersons’ performance according to the two groups in the phase I test. When they manipulated a hard-to-use type of AED, successful defibrillation could be more time-consuming and less likely to be achieved,and this finding agrees with those of previous studies.As demonstrated by Percival et aldefibrillation completion rates in laypersons would differ by AED types. Eames et alalso found that their performance with different AEDs showed differences in time parameters, including time to power on and time to first shock. Later, Mosesso et alconfirmed this time parameter divergence and further concluded that device features had a strong impact on the time to power on device and initiated CPR.
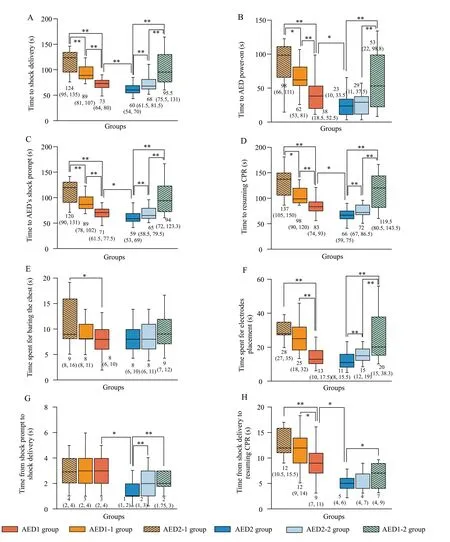
Figure 3. Time measures within participants achieving successful defibrillation (n=159). A: time to shock delivery; B: time to AED power-on; C:time to AED’s shock prompt; D: time to resuming CPR; E: time spent for baring the chest; F: time spent for electrodes placement; G: time from shock prompt to shock delivery; H: time from shock delivery to resuming CPR. Data were presented as median (interquartile range). *P<0.05;**P<0.01.
Voice prompts are critical for AED operations.Different voice prompts in AEDs have a significant effect on the operation time, which was supported by the results of our study (Figure 3H) and by previous research.Voice prompts instructing to resume CPR with longer pause time and less specific instructions led to a longer time to resume CPR. Therefore, AED voice prompt design should target the creation of more specific instructions with shorter pause time for lay rescuers,which can eventually improve AED operation and survival from cardiac arrest.
It should be highlighted that once people are trained with one type of AED, they can operate any other AED with accurate key actions. The reason lies in the simplicity of the AED. Since AEDs were inherently designed for laypersons, subjects were able to master most of the AED operation points and operating procedures after training. Consequently, subjects were able to operate the AED correctly, even when they were unfamiliar with the specific type. This was the reason why the behavioral indicators compared in the two switched subgroups did not show significant differences.
However, people needed more time to operate on AEDs different from the one they were trained with. The prolonged time was observed in three time parameters,namely time to power opening, time to defibrillation prompt, and time to resuming CPR. The two AEDs utilized in the present study had evident differences in three features, specifically in the power-on mechanism and the two voice instructions, which were directly related to the three differential secondary time indicators.Therefore, we determined that the differences in the parameters could be explained by the device feature diversity. For example, the power opening time was significantly shorter in the AED2 group than in AED1 group. Because the button of AED1 was inside the machine, subjects needed more time to open the outer zipper of the machine to find it, while the button of AED2 could be seen directly outside the machine and could be pressed directly. Consequently, subjects who had used AED1 for training in the phase I test were more familiar with the button being inside the package. Therefore,when encountering the same AED in the phase II test,they could find the button and press it more quickly. In contrast, for subjects who used AED2 in the phase I test,the power-on button was directly displayed outside of the package. Accordingly, when they encountered the AED1 whose power-on button was inside the package, it would take them more time to find the location of the button,which prolonged the AED boot time.
As such, current teaching program suggests that training laypersons with a single type of AED is feasible because people can operate all kinds of AEDs correctly once they are trained with one of them. If we want to improve their performance in time to achieve the optimal prognosis of the OHCA patients, some aspects of the AEDs still need to be improved.
To overcome the limitations of the current AED training wherein only one type of AED is employed,better training for laypersons and technological improvements of the AEDs are probably needed. We recommend that in future basic life support (BLS)courses, different AED devices should be used, if possible, or the main differences of major AEDs should be displayed and explained in the form of videos or pictures as substitution. Moreover, in terms of device design characteristics, future AEDs could combine all the “good” features of previous AEDs that have been verified by our research and previous research as well.For example, devices with open lids, pull handles, more detailed voice prompts for pad placement, and step-bystep CPR instructions can enable users to achieve shorter power-on time, greater adequacy of pad position, and better CPR performance after shock delivery. In addition,voice instruction for resuming CPR could be more compact and urgent with a shorter pause time.
Limitations
Several limitations of our study merit attention when interpreting our results. First, only two AEDs were selected in this experiment, which did not cover every AED currently available. Nevertheless, the two AEDs utilized in this study represent two main types. Thus,the conclusion of this study has at least some degree of wider applicability and generalizability. Second, in terms of experimental design, this simulation study may not reflect real-life scenarios. Third, the participants recruited in this study were college students who attended the“WeCan CPR” training project, which may be a source of selection bias. Future studies should use a more diverse sample population.
CONCLUSIONS
In conclusion, using different AEDs with distinctive features during training and in the future does not significantly affect the AED operation performance of laypersons, although it may increase the time to shock delivery. Updating the CPR training method and optimizing the AED features should be considered to improve AED operation performance.
ACKNOWLEDGEMENTS
The authors express their appreciation to Shuang Tian, Yue-lin Yu, Shu-xiao Shi, Xiao-chen Yang,and Xiao-qian Zhang for conducting the participants enrollment and on-site data collection which ensure the high quality of study data. We sincerely thank participants from Shanghai Jiao Tong University for their time and active involvement in this study.
National Natural Science Foundation of China(72074144; 81703303) and Innovative Research Team of High-level Local Universities in Shanghai (No. SHSMUZDCX20212801).
This study was approved by the Joint Research Ethics Board of the Shanghai Jiao Tong University School of Public Health and Nursing (SJUPN-201714).
None.
LZ and JLY contributed to the conception of the study; HWQ and XJD contributed significantly to data collection and data analysis; CYL, HWQ and XJD performed the drafting of the manuscript; CYL and LZ finalized the manuscript; LZ and JLY provided administrative advices and consultations. All authors contributed substantially to its revision. CYL, HWQ, and XJD contributed equally to this work.