
Traditional herbal medicine as adjunctive therapy for colorectal cancer: a scoping review
2022-02-26 03:15:52SitiRohaniNurumalNurSuhadaRamliZulkefleyMohammadShamsulAzharShah
Traditional Medicine Research 2022年2期
Siti Rohani Nurumal,Nur Suhada Ramli,Zulkefley Mohammad,Shamsul Azhar Shah*
1Department of Community Health,Faculty of Medicine,National University of Malaysia,Kuala Lumpur 56000,Malaysia.
Abstract Background: A variety of therapy options are available for colorectal cancer, ranging from traditional medicine to complementary and alternative medicine.There is a growing body of evidence supporting the efficacy of complementary and alternative medicine.Therefore, the main aim of this study is to conduct a scoping evaluation of traditional and herbal medicine’s effectiveness as an additional therapy for colorectal cancer patients in clinical settings.Methods:A systematic search was conducted for all articles pertaining to clinical trials related to traditional herbal medicine (THM) with or without other treatments, such as chemotherapy,placebos, or other types of treatment, published from 2010 to November 13, 2020, using four search engines, namely Medline, Web of Science, Cochrane Library, and Scopus.Results: The number of colorectal cancer patients in five trials ranged from 89 to 565 people.The THMs stated in these studies were catalpol (Rehmannia glutinosa extract), the traditional Japanese medicine Daikenchuto (mixture of herbal extracts) and Goshajinkigan, Chinese patent herbal medicine Aidi injection, and the traditional Chinese medicine Simo decoction.Positive results were reported in term of reduction of colorectal cancer tumour marker (by catalpol),improvement of gastrointestinal function following gastrointestinal surgery (by Daikenchuto and Simo decoction), better disease control rate and quality of life score(by combination of Aidi injection and chemotherapy), and a decrease in the incidence of oxaliplatin-induced peripheral neurotoxicity (Goshajinkigan).Conclusion: All studies demonstrated fewer adverse effects found in THM intervention groups, however, evidence pointing to THMs’ favourable effects on colorectal cancer patients is still required.Therefore, researchers and clinicians are encouraged to perform more research in this area so that more evidence of THM’s efficacy and safety in clinical settings can be obtained.
Keywords: traditional and herbal medicine; colorectal cancer; catalpol; Daikenchuto; Aidi;Simo decoction; Goshajinkigan
Background
Colorectal cancer(CRC) is the third most commonly diagnosed cancer,accounting for 1.8 million new cases with 862,000 deaths worldwide in 2018 [1].The incidence rate is consistently increasing and common in men as compared to women.In terms of diagnosis of CRC, the median age for colon cancer is 68 in men and 72 in women, while it is 63 for rectal cancer [2].The five-year survival rate for an early stage of CRC is 90%, while 13% of those diagnosed at a late stage [3].“Environmental” factors associated with the risk of developing CRC comprise modifiable and non-modifiable components [4].Those risk factors are obesity, greater height, red and processed meat intake,smoking, alcohol intake, and diabetes.On the other hand, the protective factors were physical activity, use of aspirin or other non-steroidal anti-inflammatory drugs, use of postmenopausal hormone [5] in women and the intake of vegetables, fruits, calcium,folate, and fibre [6].Furthermore, the advancement of screening,diagnosis, and treatment of CRC showed 30% of improvements in the survival rate from 1990-2010 [7].
The standard conventional treatments of CRC mainly are surgery,radiofrequency ablation, cryosurgery, chemotherapy, radiation therapy, targeted therapy and immunotherapy, including monoclonal antibody therapy for metastatic CRC [8].Interestingly,complementary and alternative medicine practice is common among cancer patients as a combination treatment with conventional medicine[9].
The prevalence practice in complementary and alternative medicine among cancer patients worldwide ranged between 16.5% to 93.4%[10].This shows the high interest in complementary and alternative medicine among them.Types of complementary and alternative medicine practice also varies among the countries.For example, in a study conducted at Trinidad and Tobago, more than 90% patients practise the use of herbs [11].While in Malaysia, most cancer patients practice the consumption of nutritional supplements (41.8%), herbal products (40.2%) and multivitamins (33.6%) [12].These evidences proved on complementary and alternative medicine’s well-acceptance by these population groups.Reasons for using complementary and alternative medicine included to alleviate symptoms, especially pain,improve physical and psychological well-being, treat toxicity from the conventional medical therapies, and improve immunity [13].
Specifically for CRC patients, popular choices of alternative medical system or better known as traditional herbal medicine (THM),included catalpol (Rehmannia glutinosaextract), the traditional Japanese medicine Daikenchuto (mixture of herbal extracts) and Goshajinkigan, Chinese patent herbal medicine Aidi injection, and the traditional Chinese medicine Simo decoction (SMD).Mylabrisis the main herb of Aidi injection.As early as about 206 B.C.E.to 220 C.E.,Shennong Bencao Jing(Shen-nong’s Herbal Classics), a Chinese book on agriculture and medicinal plants, traditionally attributed to Shennong,has recorded this herb can be used to treat Echuang, a disease in Chinese medicine theory that has the similar symptoms with skin cancer in Western medicine, such as the skin is ulcerated, pus and blood, and the wound is difficult to heal [14].SMD is recorded in theJisheng Fang(Formulas to Promote Well-Being), a book of formulas written in 1253 by Yan Yonghe and it is used to treat intestinal disease[15].Recently, a randomized trial with 590 participants showed that the combination of SMD and acupuncture may reduce the incidence of postoperative ileus (POI) for patients with CRC after resection [16].To date, although many clinical research has been conducted to determine the effects of THM on cancer patients, its review especially on CRC patients remains scarce.Thus,in this study,we aim to perform a scoping review on the effectiveness of THM as adjunctive therapy for CRC patients in clinical settings.
Methods
Search strategy
The search for this study was performed in November 2020, including articles published from 2010 until up to 13 November 2020.Four search engines that covered the international content of healthcare;Medline, Web of Science, Cochrane Library, and Scopus were used.The search strategy included combined terms using the Boolean operators “AND” and “OR” with medical subject headings terms used,which are as follow: (“colorectal cancer” OR “colorectal neoplas*” OR“colon cancer” OR “l(fā)arge bowel cancer” OR “rectal cancer”) AND(“traditional herbal medicine” OR “THM” OR “herb*” OR“complementary medicine”) AND (“effectiveness” OR “efficacy”).The retrieval strategy using the above databases revealed 277 articles.The search strategy is shown in Supplementary Table S1.
Study selection
The eligibility criteria for our study were limited to human studies,open accessed empirical articles, and written in English.All selected empirical articles were quantitatively assessed on the effectiveness of THM.Inclusion criteria were based on the population/intervention/comparison/outcome framework: (1)population - CRC patients; (2) intervention - THM with or without other treatment; (3) comparison - conventional chemotherapy,placebo or other types of treatment; (4) outcomes - regarding the four effectiveness dimensions (Table 1).We excluded animal studies,non-trials, non-empirical, protocols, and review articles analyzing THM effectiveness.The best diagnostic criterion for CRC is biopsy of the lesion following colonoscopy, biomarker testing and genomic profiling.This will enable to determine the molecular characterization of sporadic and hereditary diseases and enabling personalised care[17].However, we do not examine the specific diagnostic criteria for CRC in each article in this study.The fact that each article states that the respondents were selected from among CRC patients is sufficient information.
Search results were imported into EndNote, and duplicates were removed.Basic information from the remaining articles was exported to a Microsoft Excel sheet.Three authors (NSR, SRN and ZM)independently reviewed all the titles, references and abstracts generated by the original search in order to identify articles for potential inclusion.The three authors independently conducted a full article assessment in the next stage, following the pre-specified inclusion criteria, and the results were compared.In order to increase the reliability of the process selection, the differences were all reconciled by consensus.Quality assessment was performed according to the Newcastle-Ottawa guidelines [18] (Supplementary Table S2).Data extraction was performed by one author and revised by a second,using a standardized Excel spreadsheet, in which columns represent the categories of analysis.The included studies were classified according to several descriptive aspects, including authors; year;country; study design; study objective; participants; sample size;control group therapy; THM intervention; herb species; outcomes measured; and results.
Results
This study is reported in accordance with the preferred reporting items for systematic reviews and meta-analyses guidelines published by Moher et al.(2009) [19] (Supplementary Table S3).The initial search retrieved 277 articles, with 14 duplicated.The title and abstract analysis resulted in the exclusion of 24 articles.In the full assessment of the 18 articles, 13 articles were excluded for falling outside the scope of this review, resulting in a final list of 5 articles(Figure 1).
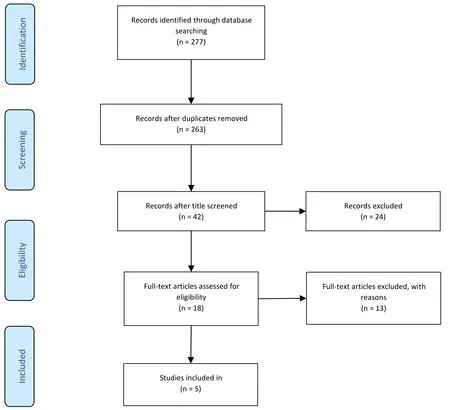
Figure 1 Study selection flowchart according to the preferred reporting items for systematic reviews and meta-analyses guidelines
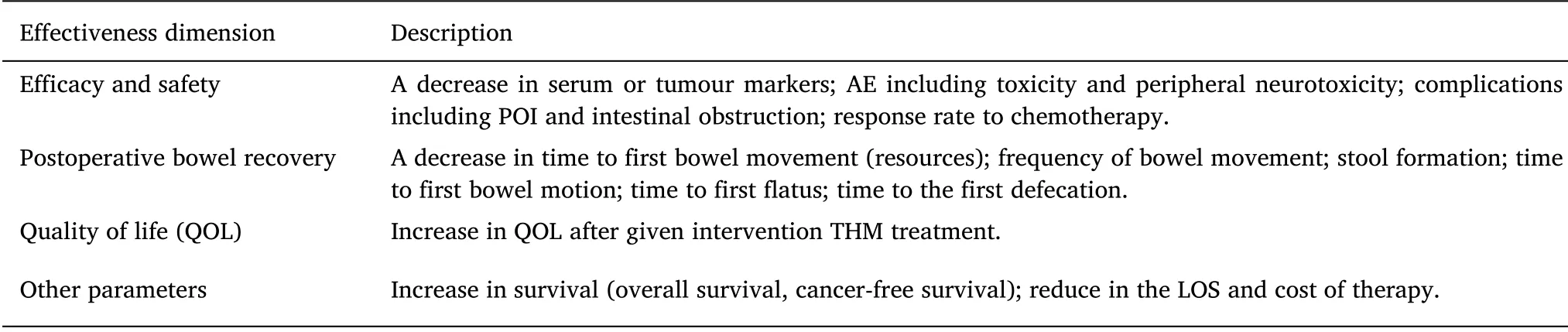
Table 1 Effectiveness dimensions studied and their description
Studies characteristics
Among all five studies, four (4/5; 80%) were randomized [20-23],and the remaining one (1/5; 20%) was non-randomized [24].Throughout the ten years search period, only one study was published per year; Xu HX et al.[24], in 2011, Kono T et al.[20], in 2013,Katsuno H et al.[21],in 2015,Yang Y et al.[22],in 2017,and Fei B et al.[23], in 2018.Most (3/5; 60%) studies were conducted in China[22-24], and two (2/5; 40%) studies were conducted in Japan [20,21].
The majority of participants were postoperative patients [21-23],while the other participants were those going for CRC chemotherapy[20, 24].The number of participants ranges from 89 [20] to 565 [22].Control group therapies used by studies in this review were either placebo [20, 21, 23], conventional chemotherapy [23, 24], other therapy, i.e.commercially available chewing gum [22] or no therapy[22] (Figure 2).While for intervention therapies, five different THMs were used in each study; catalpol (Rehmannia glutinosaextract) [23],the traditional Japanese medicine Daikenchuto [21], Chinese patent herbal medicine Aidi injection [24], the traditional Chinese medicine SMD [22] and the traditional Japanese medicine Goshajinkigan [20].Each of the studies used different types of THM and each THM have a different combination of herbal species except for catalpol that consists of one herbal species.The composition and the function of these THMs are summarised in Table 2.
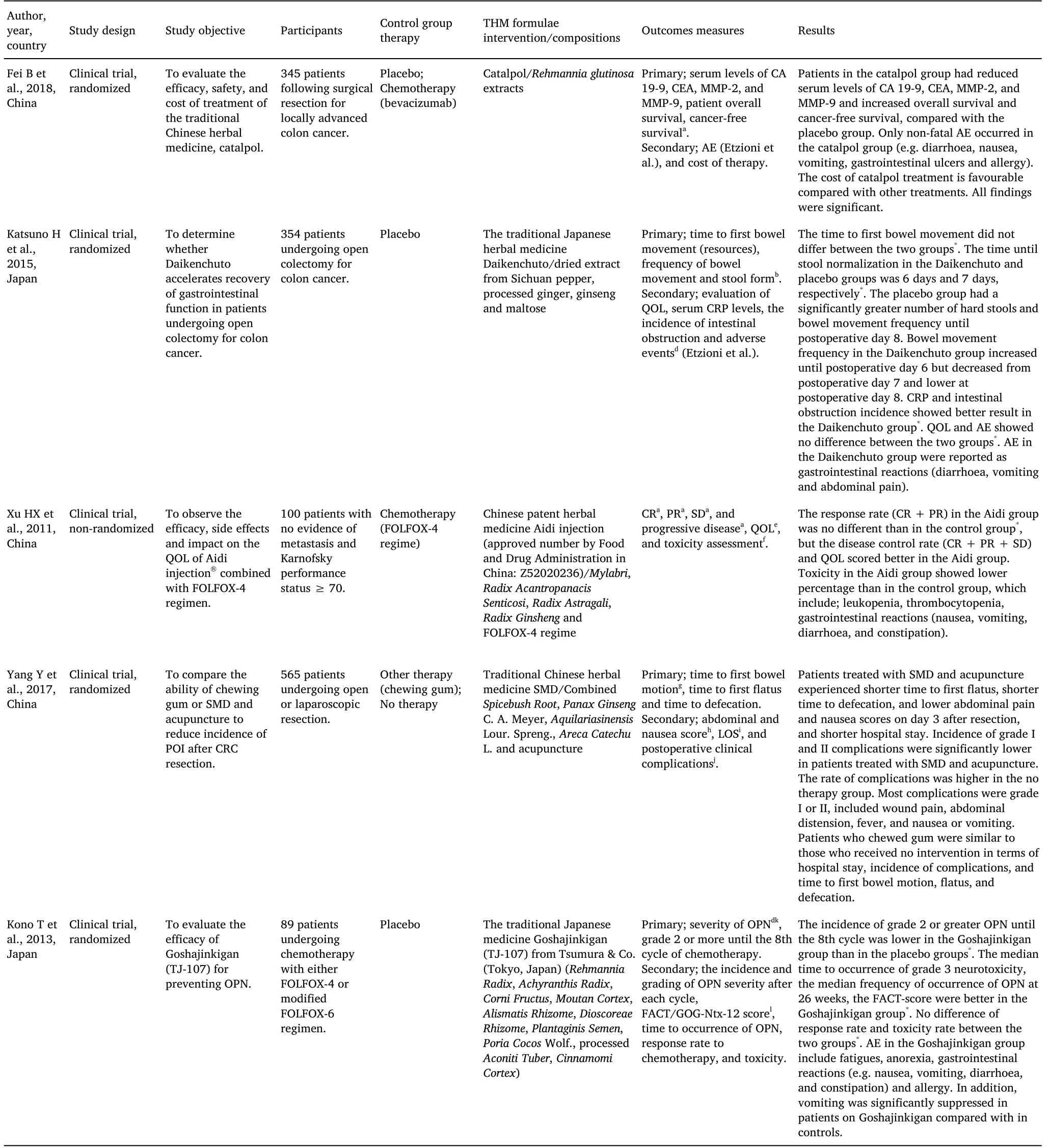
Table 2 Evidence for all five studies in this review

Figure 2 Type of control group therapy according to the study
Efficacy and safety
Serum tumour markers and anti-inflammatory marker.There were two studies in this review assessing THM effectiveness using serum tumour markers as their outcomes.First, a study conducted by Fei B et al.[23] reported on a significant reduction of serum tumour-marker levels of carbohydrate antigen 19-9 (CA 19-9),carcinoembryonic antigen (CEA), matrix metalloproteinases-2(MMP-2), and matrix metalloproteinases-9 (MMP-9) in postoperative patients who were treated with catalpol, compared with serum levels in those who received placebo.Secondly, Katsuno H et al.[21] found that the mean serum anti-inflammatory marker of C-reactive protein(CRP) levels was lower in postoperative patients treated with Daiketchuto, compared with that in those treated with placebo;nonetheless, the difference was not statistically significant.
Adverse effects (AE).AE, side effects or toxicity of THM related therapy were addressed in all five studies (Figure 3), where most studies showed better AE outcomes in THM intervention groups.According to Fei B et al.[23], non-fatal AE, mainly gastrointestinal reactions (e.g.diarrhoea, nausea, vomiting) and allergy, were significantly associated with catalpol treated group, compared with its control group of chemotherapy-only, where fatal AE were also reported.
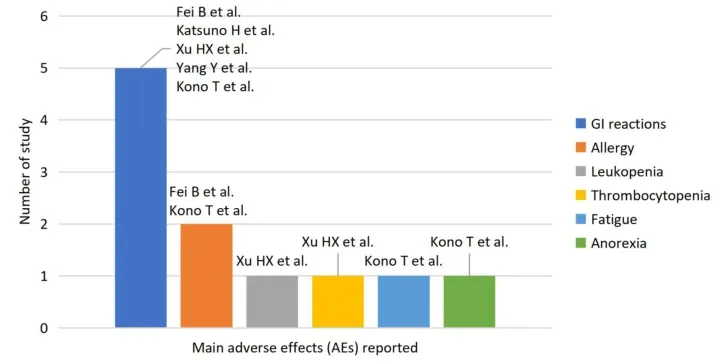
Figure 3 Main AE related to THM according to the study.
In the study of THM Aidi therapy, Xu HX et al.[24] reported that the toxicity of Aidi and the chemotherapy group showed a lower percentage than that in the chemotherapy-only control group.The main AE identified in the intervention group were leukopenia,thrombocytopenia, gastrointestinal reactions (nausea, vomiting,diarrhoea, and constipation).In terms of AE of abdominal pain and nausea, significantly lower scores (better scores) on day 3 post-operation were reported among patients who were treated with SMD compared to those treated with either of the other therapies(commercially available chewing gum) or no therapy, as described by Yang Y et al.[22].With regards to the severity of oxaliplatin-induced peripheral neurotoxicity (OPN), Kono T et al.[20] found that that the incidence of grade 2 or greater OPN until the 8th cycle is lower in the THM group of Goshajinkigan, compared to that in the placebo group,although it was statistically not significant.In the same manner, both the median time to the occurrence of grade 3 neurotoxicity and the median frequency of occurrence of OPN at 26 weeks were also found to be lower in the Goshanjikigan treated group.In addition, the median Functional Assessment of Cancer Therapy/Gynaecological Oncology Group-Neurotoxicity-12 (FACT/GOG-Ntx-12) scores of the Goshajinkigan treated group was lower than that in the placebo groups.Although the differences were statistically unremarkable,patients receiving Goshajinkigan tended to show milder symptoms of neurotoxicity than those who received a placebo.
The prince was not a little surprised, but he consented to hide himself with Asmund behind the panelling of the room, from where they could see all that went on through a little slit24
Most studies in this review reported less occurrence of AE in THM intervention groups.However, there were also indifferent findings.Such findings were shown in two studies, conducted by Katsuno H et al.[18] and Kono T et al.[20], where they found no different significant rates in the occurrence of AE (other than peripheral neurotoxicity) in Daikenchuto compared with its placebo control group, and in Goshajinkigan treated compared with its placebo control group, respectively.With regard to this matter, AE reported in the Daikenchuto group were gastrointestinal reactions (diarrhoea,vomiting and abdominal pain), while main AE in the Goshajinkigan group include fatigues, anorexia, gastrointestinal reactions (e.g.nausea, vomiting, diarrhoea, and constipation) and allergy.
Complications.Two complications found in this review were related to post-cancer-resection-operation: the incidence of intestinal obstruction and the incidence of POI.In the study conducted by Katsuno H et al.[21], no significant difference was observed between the rate of intestinal obstruction incidence between the Daikenchuto treated group and its placebo control group.On the other hand, Yang Y et al.[22] reported that the POI occurrence (presented in the form of grade I and II complications according to the Claviendo-Dindo classification) were significantly lower in patients treated with SMD and acupuncture, and higher complication rates were observed in no therapy group.
Response Rate to Chemotherapy.According to Xu HX et al.[24],there was no difference in the response rate to chemotherapy(complete remission (CR) + partial response (PR)) among those who received THM intervention of Aidi and chemotherapy, compared to those in the chemotherapy-only control group.However, there was a significant difference in the disease control rates (CR + PR + stable disease (SD)) between the two groups, where patients in the Aidi-chemotherapy group scored a higher percentage.In another study, Kono et al.[20] also described the non-significant difference of the overall response rates ((CR + PR) and (CR + PR + SD)) in both the THM Goshajinkigan treated group and its placebo control group.
Postoperative bowel recovery
Two studies were evaluating postoperative bowel recovery: first bowel motion, time to first flatus and time to defecation, frequency of bowel movement per day, and change in the Bristol Stool scale score after surgery.In the study conducted by Yang Y et al.[22], it was shown that time to first flatus and time to defecation was significantly shorter in those treated with THM oral SMD and acupuncture as compared to those treated with commercially available chewing gum or those received none of the therapies.These results were statistically significant.On the other hand, the finding by Katsuno H et al.[21]showed that bowel movement frequency postoperative on day eight in the Daikenchuto treated group was significantly lower than the placebo group.Subsequently, the time for the stool to be normalized in the formation (50thpercentile) in the Bristol Stool scale score of 1 and 2 took longer in the placebo group as compared to the Daikenchuto group on postoperative day 8.Furthermore, all the groups in both of the studies showed a similar time to first bowel motion.
Quality of life
Two studies explored the area of QOL.The study conducted by Xu HX et al.[24] used the Karnofsky performance scale to measure QOL before and after treatment.This functional status scale is a single dimension that provides a global measurement level of activity,mainly for cancer treatment patients [25].Karnofsky performance scale was evaluated with increasing and decreasing scores by ten or otherwise stable.The result showed that the experimental group(THM intervention of Aidi and chemotherapy) had a 60% increase in Karnofsky performance scale score while the control group(chemotherapy) was 24%.The difference between the groups was statistically significant.Meanwhile, in another study Katsuno et al.[21] the evaluation of QOL according to the Gastrointestinal Symptom Rating scale (Japanese version) and Functional Assessment of Cancer Therapy-Colorectal scale showed no significant difference in postoperative patients treated with Daiketchuto, compared with those treated with placebo.
Other parameters
There was one study that measured the survival rate.A study by Fei B et al.[23] showed that the percentage of cases of recurrence of colon cancer after surgical resection significantly increased in the placebo group (no chemotherapy) and catalpol treatment group when compared with the control group (with chemotherapy).There was a significant increase in overall survival in the catalpol treatment group compared with the placebo group (no chemotherapy).However, there were no significant differences between catalpol treatment and chemotherapy treatment.Fei B et al.[23] also measured the cost of catalpol treatment, which was more favourable than chemotherapy treatments for CRC.The cost of using catalpol treatment was significantly cheaper when compared with the cost of chemotherapy.The length of hospital stay(LOS) post colorectal surgical resection was measured by Yang Y et al.[22], whereby it was noted that LOS for patients receiving SMD with acupuncture (LOS = 8.9 days (SD 1.9))was significantly shorter than patients receiving chewing gum (LOS =10.5 days (SD 2.5)) and no intervention (LOS = 10.9 days (SD 2.4)).
Discussion
Study characteristics
To our knowledge, this is the first systematic review conducted to examine the effectiveness of THM in CRC patients, regardless of the stage, comparing the THM therapy modalities with other types of therapies.However, within the ten-year search period, only five studies suited our selection criteria, with the most recent study was published in 2018.Notably, all studies in this review were conducted in the two Far East countries; the Republic of China and Japan.This reflects on the prevalent use of THM in the treatment of CRC in these regions [26, 27] and the scarcity of THM clinical trials being conducted in other regions, despite mounting evidence suggesting the advantages of THM use as part of CRC treatment derived from in vitro and in vivo experiments [28].
Efficacy and safety
Our findings showed that there is a significant reduction in the serum levels of tumour markers (CA 19-9, CEA, MMP-2, and MMP-9) [23]and a non-significant reduction of serum anti-inflammatory marker(CRP) [21] in CRC patients who used THM therapy versus the controls(catalpol vs placebo and vs chemotherapy; and Daikenchuto vs placebo) post-cancer-resection.According to a study done by Zhu P and colleagues [29], catalpol inhibits the proliferation, growth, and invasion of cancerous CT26 cells in dose-dependent manners and reduces the secretion of several angiogenic markers.The immunohistochemical assay also showed that catalpol inhibits the expressions of angiogenic markers vascular endothelial growth factor,vascular endothelial growth factor receptor 2, hypoxia-inducible factor-1α and basic fibroblast growth factor in colon cancer tissues.It also inhibits the expressions of inflammatory factors interleukin(IL)-1β, IL-6, IL-8, cyclooxygenase and inducible nitric oxide synthase.Altogether, catalpol suppressed the growth and invasion of CT26 colon cancer cells mainly by inhibiting inflammation and tumour angiogenesis, viewed as a promising candidate compound for treating colon cancer [29, 30].With regards to the results in the Daikenchuto group in the mentioned study, a similar trend was reported by Yaegashi M et al.[31], where they found no significant intergroup differences in serum CRP levels.However, a significant CRP reduction was also evident among postoperative CRC patients treated with Daikenchuto [32].The physiological process was thoroughly described in a few in vitro studies, where it significantly inhibits the infiltration of neutrophils and CD68-positive macrophages and inhibits mRNA expressions of tumour necrosis factor-alpha and monocyte chemoattractant protein-1 hence leading to CRP reduction[33, 34].
A very similar study of SMD efficacy, as reported by Yang Y et al.[22],was also conducted by other researchers [38], with a similar aim to compare the efficacy between SMD combined with acupuncture and its two control groups (SMD vs chewing gum and SMD vs no intervention) for treating POI in patients with hepatocellular carcinoma after hepatectomy.There is evidence from the animal model that SMD able to reduce the serum level of the of proinflammatory of cytokines and white blood cells [39, 40] that can enhance the gastrointestinal motility proposed by the observation that it promotes the contraction of antral strips by activating muscarinic M3 receptors[41].To our interest,their results showed a similar trend,where the incidence of complications was significantly reduced in the SMD and acupuncture groups.
The other THM included in this review is Goshajinkigan.Interestingly, findings made by Kono T et al.[20] contradicted with results reported in another systematic review of Goshajinkigan’s role in the prevention of chemotherapy-induced peripheral neuropathy[42].In the later review, Kuriyama A and Endo K reported no beneficial association found for grade 2 or more of chemotherapy-induced peripheral neuropathy and Goshajinkigan was not associated with reduced incidence of chemotherapy-induced peripheral neuropathy or improved response to chemotherapy [42].What is more, one clinical trial also revealed the incidence of grade 2 or greater OPN was significantly associated with Goshajinkigan [43].In other aspects, we found no other studies analyzing the median time to the occurrence of grade 3 neurotoxicity, the median frequency of occurrence of OPN at 26 weeks, and the median FACT/GOG-Ntx-12 score found in our literature search.
The final THM being discussed for AE in this review is Daikenchuto.As its efficacy found in CRC patients is scarce, its efficacy in gastric cancer patients was described in other studies, where there was no significant intergroup difference in AE of grade 3 or more (according toNational Cancer Institute Common Terminology Criteria for Adverse Events(version 4.0)) [44].Besides the AE mentioned above,complications found in this review included intestinal obstruction and POI.In few other studies, findings, as presented by Katsuno H et al.[21], were also found in another clinical study and one meta-analysis.Both were studying the efficacy of Daikenchuto for postoperative gastrointestinal cancer on the occurrence of intestinal obstruction and POI, respectively, with the THM intervention showing no significant differences [45, 46].To our knowledge, studies describing the incidence of POI among CRC patients treated with SMD as presented by Yang Y and colleagues in this review, are still lacking [22].However, the use of SMD remains suggested, knowing the main therapeutic principles of TCM is to promote the recovery of gastrointestinal function after abdominal surgery, which involves purgation purgative method, Qi-regulating (vital energy) method,spleen-fortifying and stomach-harmonizing method [47].
Regarding THM response rate to chemotherapy, the use of Aidi injection and chemotherapy was extensively studied in lung cancer rather than in CRC.Compared with chemotherapy alone, Aidi injection plus chemotherapy was found to have a significant increased relative benefit of response rate and disease control rate [36, 48, 49].It has been mentioned in previous literature, the T lymphocytes subsets (CD3+, CD4+, and CD8+ cell subsets) and CD4+/CD8+ratio take an important roles as anti tumor immunity with Aidi injection [50, 51].The nature of the evidence reviewed here requires a rigorous and comprehensive understanding of AE.This evidence was relevant for assessing safety issues; however, it did not establish causality of effects.Thus, we ought to be cautious when interpreting such data and critically question causality on a case-by-case basis,despite the fact that most THMs evaluated were only associated with moderately severe or minor AE[52].
Postoperative bowel recovery
The outcome of this review stated that the Daikenchuto group postoperative did not show a positive finding on the bowel movement frequency.This was consistent with a study conducted in Japan among the 88 patients with a primary tumour located at the right-side colon [53].In this study, it was mentioned that those in the experimental and control group was seen to not differ in the intestinal motility postoperative on day 1 (P= 0.27), day 3 (P= 0.10) and as well as on day 5(P=0.09)in the small and large intestines.However,there was a significant difference among the patients ≥75 years old(P=0.049)at postoperative day five but not at day one and day three among the experimental group.On the other hand, Katsuno H et al.[21] found no significant finding to first bowel motion postoperative in the Daikenchuto group.A recent study in a subgroup analysis of three randomized controlled trials among 410 patients with no bowel movements after open abdominal surgery secondary to colon, liver, or gastric cancer was performed.Interestingly, the finding was contrast as the median time for a first bowel movement is 99.1 hours in the experimental group compared to 113.8 in the other group with (P=0.004; hazard ratio 1.337) [54].This finding was similar to another study as the first bowel movement in the Daikenchuto group is (82.9+/- 17.8h vs 99.5 +/- 18.9h,P<0.01) compared with the control group after patients undergoing laparoscopic-assisted colectomy for colon cancer [31].Furthermore, a comparable aim of the study by Yang Y et al.[22] was conducted among the hepatocellular carcinoma to explore the efficacy between SMD combined with acupuncture and its two control groups (SMD vs chewing gum and SMD vs no intervention)[38].The finding showed a similar trend of shorter time to flatus and defecation than the no-intervention group (allP<0.05).Nevertheless, the first time to peristalsis is also shorter,which was similar to the findings in all of the groups in the study done by Yang Y et al.[22].The stimulation of gastrointestinal mortality leading to shorter time of flatus, defecation and peristalsis[41].Thus,the finding can be seen as being varied from one study to another.
Quality of life
In terms of QOL, the combination of (THM intervention of Aidi and chemotherapy) was seen as beneficial in our review.The finding was also seen to be inline in 3,200 patients with multiple types of cancers as the QOL are significantly improved in performance status compared with chemotherapy alone across the stratification of gender, age,tumour type, tumor, nodes, metastases stage, body mass index, nodal metastasis, prior chemotherapy, chemotherapy regimens, other Chinese tradition medicines, and chemotherapy cycle [55].The decreased in the incidence rate of chemotherapy-related toxicity and improve performance status in patients will improve the QOL in patients received Aidi injection.At the same time, the findings are consistent in the meta-analysis in patients with advanced non-small-cell carcinoma as the Karnofsky performance scale score significantly increases and improve the QOL in a group that received Aidi injection plus chemotherapy [36, 56].Subsequently, the effect of Daiketchuto, compared with that in those treated with placebo on QOL is still limited.Thus, more study needs to be conducted to analyze clinical efficiency.Interestingly, a recent study conducted in Malaysia also shown to improve QOL among various type of THM and cancer patients using the European Organization for Research and Treatment of Cancer Quality of Life questionnaire scale[57].
The survival rate, length of stay and cost-effectiveness of THM
This review was unable to support the survivability of CRC with THMs used, as only one study measured the survival rate.Furthermore, the overall survival and cancer-free survival of CRC patients using THM,especially catalpol were not favourable compared with chemotherapy treatment.A study done by Johnson et al.[58] showed that patient with breast, prostate, lung, and CRC that declined chemotherapy treatments in favour of alternative medicine including THMs had a higher risk of death (hazard ratio = 2.50, 95% CI = 1.88 to 3.27).Another survival analysis of 258 cancer patients who used complementary medicine (including THM) showed poorer 5-year overall survival than 1,032 cancer patients who did not use complementary medicine and a greater risk of death [59].On the other hand, study among non-small-cell carcinoma without significant publication bias reported THM with chemotherapy improve survival rate [60].Nevertheless, the same study, suggested to conduct more randomized controlled trial to get more definite conclusion as limited methodological qualities of the included trials
In general, CRC patients had a greater probability of hospitalization with the highest average of LOS compared with other types of cancer[61].Our finding showed that using THM can reduce LOS for post colorectal surgical resection.This was contrary to a study done using THM (Daikenchuto) for oesophageal cancer patients [62].The postoperative bowel symptoms tended to be rare in the THM group,however,statistically,there was no significant and no difference in the LOS after surgery.In terms of cost, as generally, the THM is cheaper,as endorsed with our findings.The cost-effectiveness of some herbal medicine is encouraging in certain areas, especially in relation to postoperative surgery [63], however, further clinical research is needed to establish the cost benefits that may be achievable in other settings such as QOL and pain reduction, especially for colorectal patients.
THM used and composition of their species
Only catalpol has a single herbal species in this review, while other THMs consist of multiple herbal species.For the time being, the use of catalpol may be specific to a CRC patient.We could not find any study using catalpol for other types of cancers, as many studies of catalpol are still in vitro and in vivo stage.Apart from that, catalpol has a hypoglycaemic effect, and its role as a diabetic medication is also still unknown in an animal study [64].In the review by Yang Y et al.[22],the author did not mention the composition of SMD.However, from another study it was known that SMD contains ingredients fromFructus Aurantii,Radix Aucklandiae,Semen ArecaeandRadix Linderaethat is used for improving gastrointestinal function [65].When comparing the composition and herbal species for each THMs used in this review, we found out that some of the THMs share the herbal genus but not their species.In addition, some of THM with the same generic name have a slightly different composition.For example, a study by Akamaru Y et al.[45] used Daikenchuto in gastric cancer to improve intestinal motility after gastrectomy, composed of dried extracts from ginger root, ginseng, andZanthoxylumfruit that slightly defer from the article reviewed.Another example was a study of Aidi injection by Xie et al.[55], which was composed of extraction fromRadix Ginseng, Astragaloside,Eleutherococcus senticosus, and Cantharidin; that slightly defer with the article reviewed.The same study also showed that a similar composition of Aidi injection could be used for a different type of cancer.However, it is interesting to notice that the herbal species for CRC in this review can be different from the herbal species used for other cancer treatments such as breast,lung, prostate, liver, and pancreatic cancer [66].Meanwhile,Goshajinkigan is a mixture of aqueous extracts from 10 wild herbs, as Kono T et al.[20] mentioned.In the study by Yagi et al.[67], there are two herbs with similar genus but different species in the Goshajinkigan.As mention earlier, the main use of Goshajinkigan is for the reduction and prevention of chemotherapy-induced peripheral neuropathy.However, traditionally it is used to treat diabetic neuropathy [68] and overactive bladder [69].In term of, the diabetic neuropathy the action was by suppressing functional alteration of transient receptor potential channels, especially transient receptor potential ankyrin 1 and transient receptor potential melastatin 8 [70].Furthermore, on the overactive bladder are associated with the inhibition of the micturition reflex and decline of bladder sensation via the spinal kappa-opioid receptors [71].Both of this study was an animal study among rats.
Overall, the composition of THMs with differences in herbal species shows that herbal medicines' existence is diverse.This requires a careful distinction of formulary between herbal medicines to be used in cancer treatment and prevention.
Conclusion
In this review, there is a variation in the outcomes on the effectiveness of THM use in CRC patients.Although many evidence points towards it being safe and showing positive therapeutic effects, some studies prove that THM may have harmful effects.Thus, researchers and clinicians are encouraged to conduct further research in this field that can enable us to extract evidence based on the safety and efficacy of THM.This is necessary as the patient’s choice of treatments nowadays are widely varied, within the spectrum of longstanding modern and conventional type to complementary and alternative medicine, in this current modern era.
 Traditional Medicine Research2022年2期
Traditional Medicine Research2022年2期
- Traditional Medicine Research的其它文章
- Comment on “Breviscapine alleviates nonalcoholic steatohepatitis by inhibiting TGF-β-activated kinase 1-dependent signaling”
- Effects of pestle needle on nerve conduction velocity and inflammatory injury in patients with diabetic peripheral neuropathy
- Acupuncture:a new method to treat tic disorders in children
- Virtual screening of flavonoids from Jatropha gossypiifolia L.as potential drugs for diabetic complications
- Yangxin Dawayimixike honey paste inhibits atherosclerosis in ApoE-/- mice by attenuating blood lipids and exerting anti-inflammatory activity
- Study on technical efficiency of traditional Chinese medicine industry of the Belt and Road Initiative based on environmental complexity