
Comparison of perioperative parameters in one-handed rotational phacoemulsification versus conventional phacoemulsification and femtosecond laser-assisted cataract surgery
2021-12-17 02:43:22SamueleGigliolaGiancarloSborgiaAlfredoNiroCarmelaPalmisanoPasqualePuzoGianluigiGiulianiLuigiSborgiaDarioSistoValentinaPastoreClaudioFurinoRossellaDonghiaAlessandraSborgiaFrancescoBosciaGiovanniAlessio
Samuele Gigliola, Giancarlo Sborgia, Alfredo Niro, Carmela Palmisano, Pasquale Puzo,Gianluigi Giuliani, Luigi Sborgia, Dario Sisto, Valentina Pastore, Claudio Furino,Rossella Donghia, Alessandra Sborgia, Francesco Boscia, Giovanni Alessio
1Eye Clinic, Department of Medical Science, Neuroscience and Sense Organs, University of Bari, Bari 70124, Italy
2Eye Clinic, Hospital “SS. Annunziata”, ASL Taranto, Taranto 74121, Italy
3National Institute of Gastroenterology “S. de Bellis” Research Hospital, Castellana Grotte 70013, Italy
Abstract
● KEYWORDS: cataract surgery; phaco-rolling; onehanded phacoemulsification; Divide et Conquer;femtosecond laser-assisted cataract surgery
INTRODUCTION
Since the 1960s when phacoemulsification was invented[1],several modifications of small-incision cataract surgical technique were designed[2]including the “Divide et Conquer”[3], which made surgery safer and more efficient.Güellet al[4]and Jardineet al[5]described innovative bimanual approaches called “phaco-rolling technique” and endocapsular carousel technique, respectively, to reduce phacoemulsification time and energy during cataract extraction.
In the last years, the use of femtosecond laser has been expanding in cataract surgery with femtosecond laser-assisted cataract surgery (FLACS) which has automated different steps of surgery[6]reducing the phacoemulsification time and the magnitude of ultrasound energy delivery[7-9]thus leading to a safer surgery with lower corneal endothelial cell loss (ECL)and corneal edema in the early postoperative period when compared to standard technique[10-12].
However, some studies found comparable results in corneal ECL and corneal edema[13-15]macular thickness[16]and distance visual acuity[17-18]comparing conventional phacoemulsification technique with FLACS.
On the basis of previous experiences on phaco-roll techniques[4-5], we designed a surgical approach called “onehanded rotational phacoemulsification technique” (one-handed phaco-roll)[19]that potentially can improve the efficiency and safety of manual procedure, reducing technical parameters including ultrasound time and phacoemulsification power, as risk factors of damage on intraocular structures[20-21].
So, in this study we analyzed and compared safety and efficacy of one-handed phaco-roll with “Divide et Conquer”, as conventional approach, and FLACS.
SUBJECTS AND METHODS
Ethical Approval The study followed the tenets of the Declaration of Helsinki and was approved by the Institution’s Review Board of Eye Clinic, Department of Ophthalmology,University of Bari, Italy. Written informed consent was obtained from all patients before all invasive procedures.
We conducted a retrospective, comparative, cohort study on patients with uncomplicated cataract underwent cataract surgery between April 2019 and July 2019 in Eye Clinic,Department of Ophthalmology, University of Bari, Italy. All surgeries were performed by the same experienced surgeon(Alessio G). Inclusion criteria were: signed informed consent,age older than 50y, transparent cornea, cataract grade from 2-3 (nuclear opacity, NO2-NO3; nuclear color, NC2-NC3)according to the Lens Opacities Classification System III (LOCS III)[22]. Exclusion criteria were: a history of intraocular surgery or trauma; minimal and maximal K-values of the central 3 mm zone that differ by more than 5 D; a maximum K-value that exceeds 50 D; a minimum K-value of less than 37 D; corneal disease or pathology, such as corneal scaring or opacity;endothelial cell density (ECD) <1300 cells/mm2; poorly dilating pupils of less than 6 mm or any other defect of the pupil; manifest glaucoma and ocular hypertension; mature or complicated cataract (e.g., lens subluxation, traumatic cataract,pseudoexfoliation syndrome); any ocular comorbidities such as uveitis, severe non proliferative or proliferative diabetic retinopathy, macular degeneration, current infections.
Patient data (age, gender, medical history) were reviewed.Each eligible patient underwent a complete ophthalmologic examination including best corrected visual acuity (BCVA)assessed on standard Early Treatment Diabetic Retinopathy Study (ETDRS) charts[23], slit-lamp biomicroscopy, cataract density objective evaluation using Scheimpflug imaging(The Pentacam HR, Type 70900, Oculus, Germany), ocular biometry determined using partial coherence interferometry IOL Master 500 (Carl Zeiss Meditec, Jena, Germany), specular microscopy performed using a noncontact specular microscope SP-1P (Topcon Europe Medical B.V., the Netherlands),Goldman applanation tonometry, dilated fundus evaluation and optical coherence tomography (OCT) scans using 6×6 radial scans protocol by OCT AVANTI RTVUE XR (OPTOVUE,Fremont, CA, USA).
Patients were divided into three groups according to the surgical technique performed to treat cataract: one-handed phaco-roll technique (Group 1), “Divide et Conquer” technique(Group 2) or FLACS technique (Group 3).
Intraoperative parameters recorded by the phacoemulsification machine and subsequently evaluated were: ultrasound time (USt, s), effective phaco time (EPt, s), aspiration time (s), surgical time (min), phacoemulsification (phaco-)power (%), balanced salt solution (BSS?) used (mL) and cumulative dissipated energy (CDE). CDE, as a value for phaco energy, was calculated as [total phacoemulsification time (min)×average phacoemulsification power]+[torsional time (s)×0.4×average torsional amplitude (%)]. Torsional time and torsional amplitude were recorded to allow us to calculate CDE but they were not included in the intraoperative parameters. The factor 0.4 represents approximate reduction of heat dissipated at the incision as compared with non-torsional phaco[24-25].
Clinical outcomes including ECD (cell/mm2), ECL (%)calculated as (ECD preoperatively-ECD postoperatively/ECD preoperatively)×100, central corneal thickness (CCT, μm),and central macular thickness (CMT, μm) were assessed preand post-operatively at 1mo. ECD was analyzed using three photographs of each cornea taken and analysed automatically by the Image-Net imaging system (V.4.0; Topcon). A blinded observer chose the clearest photographs which was analyzed.The cell count was manually corrected according to the gold standard[26-27]. BCVA was measured at baseline and 1mo postoperatively. ETDRS values were converted into Snellen fraction and then in logMAR values for statistical analysis.Safety evaluation has also been performed as regards incidence of intra- and post-operative complications and intraocular pressure (IOP) changes.
Surgical Technique Preoperatively, all patients were treated with topical ofloxacin and bromfenac four and three times a day, respectively, for the two days preceding the surgery.Mydriasert ophthalmic insert [combination of phenylephrine hydrochlorid (5.4 mg) and tropicamide (0.28 mg)] was preoperatively positioned in the fornix to reach pupil dilation.Topical anesthesia was realized in all cases. Topical 5%povidone-iodine solution was instilled before and after surgery.The same ocular viscoelastic device (OVD; IAL-F?, Bausch& Lomb, NY, USA) was used for all three groups. The same phacoemulsification machine (INFINITI?Vision System Alcon Laboratories, Inc, Fort Worth, Tex, USA) was used for all surgery.
After the intraocular lens (IOL) implant into the capsular bag, the OVD was removed, a solution of 0.1 mL cefuroxime(Aprokam?) was introduced in the anterior chamber and finally a hydro-suture of the corneal incision was performed.Some parameters of phacoemulsification machine for different surgical phases were equally standardized for all groups: for cortical removal: vacuum, 350 mm Hg; aspiration, 30 mL/min; bottle height, 85 cm; for polish: vacuum, 20 mm Hg; aspiration,15 mL/min, bottle height, 80 cm; for OVD removal: vacuum,600 mm Hg; aspiration, 40 mL/min; bottle height, 80 cm. After surgery the therapy with corticosteroid-antibiotic combination eye drops and bromfenac eye drops with tapered frequency was administered to all patients.
One-Handed Phaco-Roll Technique A clear corneal sutureless 2.4 mm temporal incision was performed with a precalibrated knife. The anterior chamber was filled with OVD. No paracentesis was performed. A continuous curvilinear capsulorhexis (CCC) of 5.5 mm was performed.Then hydrodissection and hydrodelineation with BSS?were performed. A complete rotation of the lens within the capsular bag was performed. Subsequently a 15-degree phaco-tip was placed on the lens equator beside the capsulorhexis edge and in contact with the nucleus-epinucleus surface, so the nucleus was turned on its horizontal axis within the capsular bag.
Using high aspiration parameters including vacuum of 450 mm Hg and aspiration rate of 37 mL/min allowed to keep the probe tip occluded on the edge of the lens and to roll the nucleus as well as a spinning top. The tip was tilted to 45-degree toward the lens center. The nucleus aspiration moved from the periphery toward the center. The endo-nucleus was aspirated in the center of the bag and the epi-nucleus was aspirated. Then surgeon performed the irrigation/aspiration of residual cortex followed by the posterior capsule polishing[19].
“Divide et Conquer” Technique A 2.4 mm single temporal incision was performed using a precalibrated knife. After the CCC was created, hydrodissection, lens segmentation and other phases were performed using the “Divide et Conquer”approach[3].
FLACS Technique The Ziemer femtosecond laser (Ziemer Femto LVD Z8, Ziemer Ophthalmic Systems AG, Port,Switzerland) was used and the treatment was customized on each patient[28].
A 2.4 mm clear corneal tunnel (distance to limbus 0.2 mm,width 2.4 mm, entrance angle 40°, bend angle 56°, position angle 180° and 140°, posterior safety distance 0.7 mm, anterior corneal offset 300 microns, posterior corneal offset 440 microns, corneal depth of bend point 45%, velocity 3 mm/s,lens power 150%, spot density HD-10), anterior capsulotomy(diameter 5.5 mm, laser power 90%, velocity 50 mm/s,resection heigh 0.9 mm, later safety distance 0.5 mm, spot density HD-10) and lens fragmentation (diameter 5.8 mm,laser power 120%, segments 16, velocity 8 mm/s, later safety distance 0.5 mm, anterior safety distance 0.6 mm posterior safety distance 0.8 mm, spot density HD-5) were created under OCT image control. Then, the surgeon completed the procedure with a gentle hydrodissection, phacoemulsification of fragmentated lens, automated irrigation/aspiration to remove the cortex and IOL implant.
Statistical Analysis This study was designed to show the differences of intraoperative parameters and clinical outcomes between one-handed phaco-roll technique and each of the other two techniques, “Divide et Conquer” and FLACS. The calculation of the power (1-β) was post-hoc based on the observed value of the effect size. The most important technical parameter considering to calculate the power is the CDE.
Mean and standard deviation (mean±SD) for continuous variables and frequency (%) for categorical were used as indices of centrality and dispersion. To test the difference between two categories of surgical interventions, Wilcoxon rank-sum (Mann-Whitney) test was used for continuous scale, when not normally distributed and Chi-square test for categorical variables. When testing the null hypothesis of no association, the probability level ofαerror, at two tailed, was 0.05. All the statistical computations were made using STATA 16.0, StataCorp software 2019. Stata Statistical Software:Release 16. CollegeStation, TX: StataCorp LLC.
RESULTS
A total of 69 patients (46 females and 23 males) were enrolled and equally divided into the study groups according to our inclusion/exclusion criteria. The overall mean age of patients was 74.5±5.8y (range 56-84y). The mean age was significantly different among the Groups 1 and 2 (P=0.004). No significant difference in cataract grade was found among the groups. Axial length was slightly higher in FLACS Group than one-handed rotational Group (P=0.04). All eyes underwent a successful surgery with IOL implantation in the capsular bag. Table 1 summarizes patients’ demographic data.
Intraoperative Outcomes The USt in Group 1 (26.91±15.73s)was significantly shorter than Group 2 (41.25±25.72s,P=0.03)but significantly longer than Group 3 (17.99±9.41s,P=0.03).In Group 1 the EPt (0.66±0.70s) was significantly shorter than Group 2 (1.35±0.86s,P=0.004) and not significantlylonger than Group 3 (0.44±0.21s,P=0.44). In Group 1 the aspiration (1.37±0.56s) and surgical time (3.67±0.81min) were shorter (P≤0.001) than the same parameter in the other two groups. The phaco-power in Group 1 (75.86%±14.54%) was significantly lower than Group 2 (85.25%±3.77%,P=0.004).The CDE in Group 1 (9.75±6.85) was significantly lower compared to Group 2 (16.66±9.59,P=0.003). The quantitative of BSS?used in Group 1 (34.17±11.54 mL) was significantly lower (P≤0.01) than the other groups. Table 2 shows all intraoperative parameters recorded.
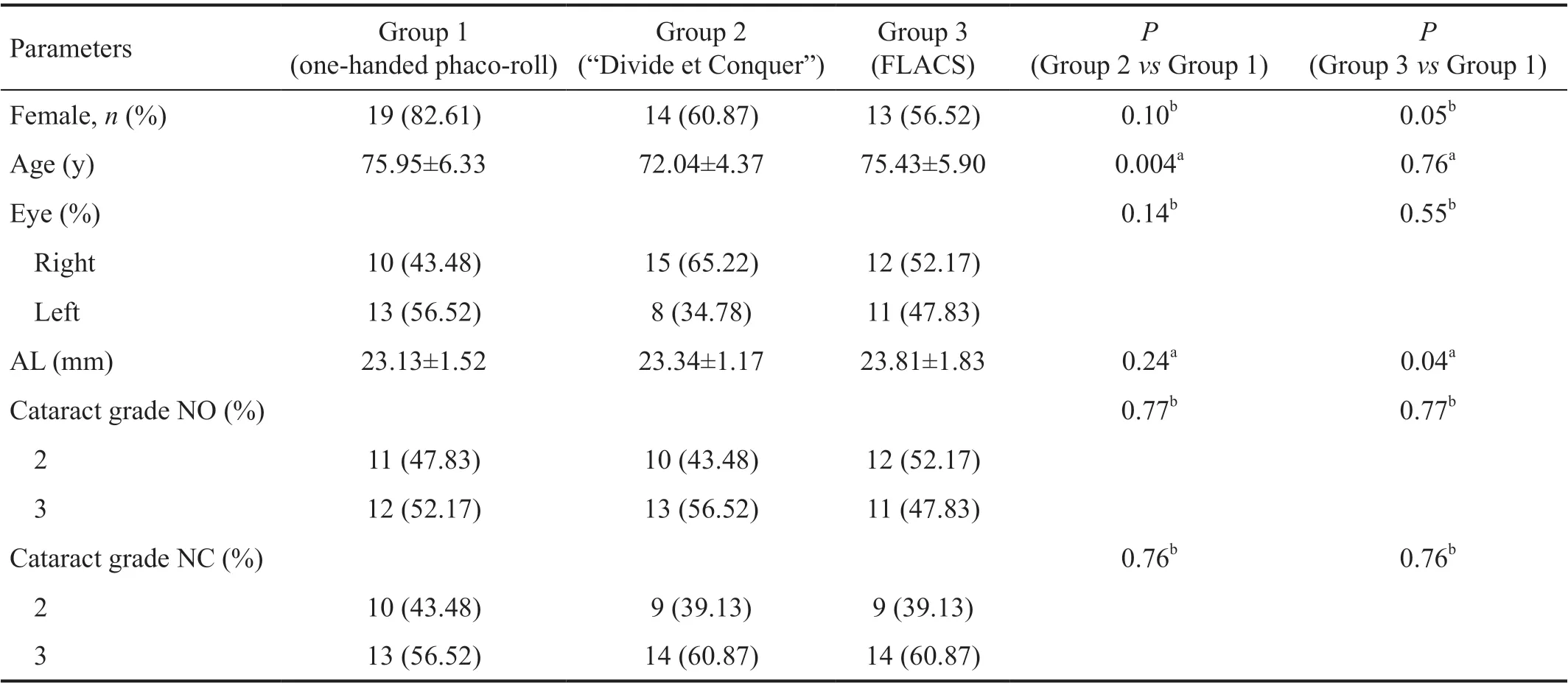
Table 1 Comparison of demographic variables among one-handed phaco-roll, “Divide et Conquer”, and FLACS surgical technique mean±SD
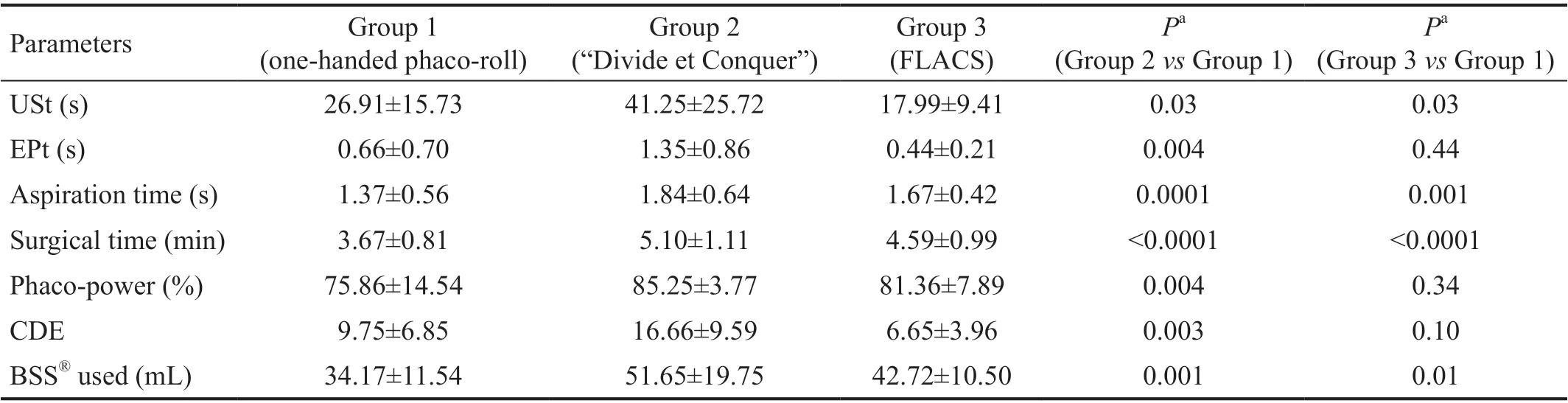
Table 2 Comparison of intraoperative variables among the groups mean±SD
Clinical Outcomes At baseline there was no statistically significant difference between the groups according to BCVA.The 1-month BCVA was not different between Group 1 and each other group (P>0.05). At baseline, a significant difference only in CCT (P=0.01) between Groups 1 and 2 was observed.After 1mo from surgery a significant difference in ECD between the Group 1 and each other group was not reported.We observed the highest ECL (11.35%±8.48%) in Group 2 without significant difference comparing to Group 1 (P=0.31).A significant difference of 1-month CCT between Groups 1 and 2 (P=0.009) was reported, though their mean percentage changes were not significantly different (P=0.97). In FLACS Group the highest percentage change of CCT (-0.94%±1.18%)from baseline value was observed. There was not significant difference regarding absolute value and percentage change of CMT. Table 3 shows all intraoperative parameters recorded.
Complications No adverse intraoperative events such as anterior capsule tear, posterior capsule tear, vitreous loss or Descemet membrane detachment occurred in either group. No postoperative complications occurred in either group.
DISCUSSION
In the present study, we compared intraoperative parameters and clinical outcomes over 1-month follow-up between one-handed phaco-roll, conventional “Divide et Conquer”technique, and FLACS to treat soft and medium-hard uncomplicated cataracts.Phaco-roll techniques were designed to reduce the surgical manipulations in the anterior chamber and the effects of ultrasound energy on endothelial corneal cells[4-5]. However,these techniques use a bimanual approach through a sideport incision[4-5]which could influence the value and the axis of post-surgical astigmatism[29-30], and increase the risk of endophthalmitis related to the potential leakage from the incision[31-33]. Furthermore, one of these techniques is dependent on a tip with a 3-port irrigation system[5].In a recent paper, we described a one-handed rotational phacoemulsification, as a modified phaco-roll technique, that uses a single corneal incision, high fluidics and low ultrasound power. The correct position and inclination of the tip, and the high aspiration allow to perform surgery with a single hand through a single incision. Performing phacosuction and emulsification with the continuous occlusion of the phaco-tip,and the rotational movement with the high vacuum and flow rate allow the aspiration of the nucleus in a short time[19].
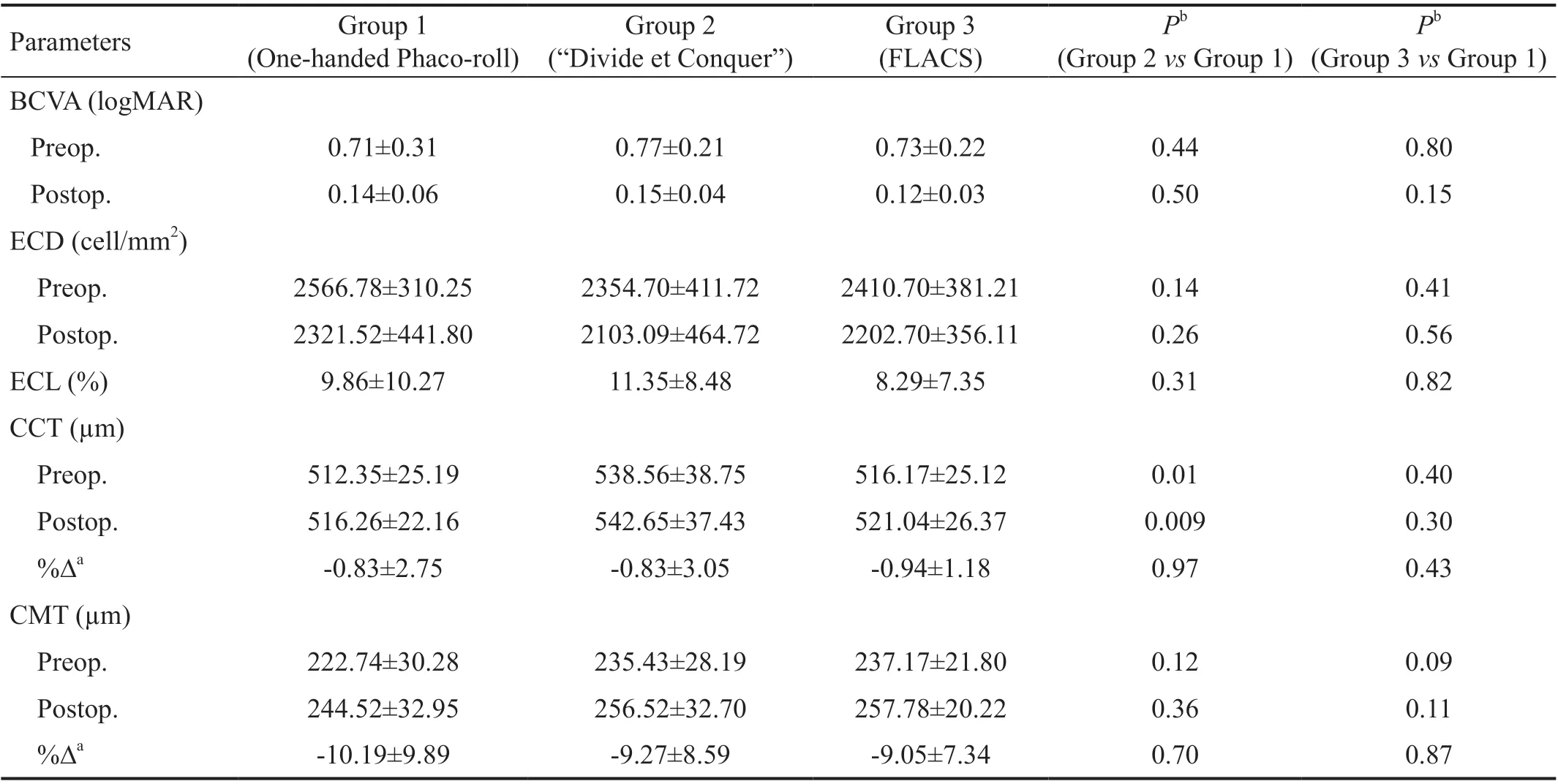
Table 3 Comparison of clinical outcomes among the groups mean±SD
In this study, younger patients, having a potential lower risk for endothelium susceptibility to surgical injury[20], underwent conventional phacoemulsification technique as potentially less safe approach for corneal endothelium[34]. This aspect of study sample could increase the significance of the results.
A Meta-analysis of 14 567 eyes from 15 randomized controlled trials and 22 observational studies comparing manual surgery and FLACS detected no statistically significant differences in terms of surgery time, revealing a considerable heterogeneity of data (manual surgery, ranged from 6 to 53.6min; FLACS ranged from 6.2 to 50.4min) probably due to the differences in surgical equipment, surgeon skill and patient selection[34].We recorded not only a shorter surgery time in conventional technique and FLACS than aforementioned data of Metaanalysis but also significantly lower parameters as total surgical time and aspiration time in one-handed phaco-roll than other surgical approaches. Indeed, if “Divide et Conquer”takes longer surgical time due to the deep central sculpting of the nucleus, manual cracking and subsequent fragmentation,FLACS technique involves a longer time since in addition to the purely surgical phase there is also the docking/suction phase which lengthens its overall timing. The same Metaanalysis, including longitudinal and torsional ultrasound machines, revealed that EPt was longer for conventional approach than FLACS without difference on CDE[34]. Recently,two prospective studies reported a significant lower EPt with FLACS than conventional surgery[35-36], while a retrospective case-control study including 506 consecutive eyes revealed that CDE was lower for FLACS than conventional approach[37].Our rotational technique takes shorter EPt and lower phacopower, and therefore lower CDE than conventional surgery,but seems not different to FLACS regarding EPt and CDE.It is also necessary to remember that we used for all groups a torsional ultrasound machine in which the formula for calculating CDE assigns only 40% of the torsional EPt to the sum, whereas the EPt for longitudinal ultrasound machine remains the same[38]. One-handed phaco-roll had shorter USt than conventional surgery but longer than FLACS. Güellet al[4]has already highlighted that phaco-roll technique allows to reduce phacoemulsification time by 30% to 50% and phacoemulsificaton energy by 20% to 40% compared with conventional technique. FLACS, for its part, has automated different steps of surgery[6]reducing the phacoemulsification time and the magnitude of ultrasound energy used[7-9]. Also the quantitative of BSS?used in rotational approach was the lowest. It is well known that the ultrasound time and power[39], the increased CDE, the aspiration time and the volume of BSS?[21], are important risk factors for ECL after phacoemulsification.
In the large Meta-analysis by Popovicet al[34], no statistically significant difference between conventional surgery and FLACS regarding visual outcomes was reported. Another Meta-analysis of 989 eyes from 9 randomized controlled trials reported that the difference of visual improvement between FLACS and conventional surgery was not significant at postoperative 1-3mo[12]. Recently, a randomised controlled non-inferiority trial reported that FLACS is not inferior to manual phacoemulsification in terms of vision after 3mo follow-up, and there were no significant differences in patientreported health and safety outcomes after 12mo follow-up[18].We were unable to find any significant difference between surgical groups regarding visual outcome. Therefore, there is an evidence to support the hypothesis that one-handed phaco-roll is equally effective on early visual outcome when compared to other two techniques.
The analysis of outcomes on corneal integrity revealed that post-surgical CCT was significant lower in Group 1 (onehanded phaco-roll) than Group 2 (“Divide et Conquer”).However, the significance of this results is limited because CCT was significantly different between Groups 1 and 2 also at baseline and the percentage changes of CCT in both groups were similar. Comparing CCT values between Groups 1 and 3 (FLACS) no difference in absolute value or percentage change was found. As previously observed, an early significant difference on CCT between conventional surgery and FLACS after 1wk disappeared after 1mo[36].
The ECL in Groups 2 and 3 was in line with previuos papers on conventional phacoemulsification (4.01%-12.9%)[2,36,40-41]and FLACS (4.22%-13.7%), respectively[36,41-42]. Previous papers suggested that the “Divide et Conquer” technique provokes more corneal endothelial damage than other conventional techniques[2]and FLACS[10,25,34]because it uses more phaco energy to crack the nucleus. In one-hande phaco-roll group,ECL was lower than conventional phacoemulsification group but higher than FLACS group, though in a not significant way.This result could further confirm that one-handed rotational approach is equally safe for corneal integrity when compared to “Divide et Conqer” and FLACS. In all groups, an increase of 1-month macular thickness was recorded, although without difference among rotational approach and other techniques.
The thickening of macular site may be due to the release of cytokines and growth factor from the blood-ocular barrier after cataract surgery[43]. In the only prospective randomized study on macular changes in eyes underwent different surgical techniques for cataract, authors concluded that FLACS does not increase the occurrence of macular edema when compared to standard phacoemulsification[16], as confirmed by recent studies[44-45]and by our results.
Overall, no complications were reported, probably due to well standardized techniques used and surgeon experience in all surgical techniques performed.
The small sample size and short follow-up may have limited the significance of the results. Furthermore, refractive parameters as surgically induced astigmatism, refractive spherical equivalent and higher-order aberrations were not analysed.
As first in literature, we highlighted that one-handed rotational phacoemulsification technique seems to be less timeconsuming than “Divide et Conquer” and FLACS and less energy-consuming than “Divide et Conquer” in treating elected and uncomplicated cataracts. Furthermore, one-handed phacoroll seems to have an equal safety profile compared to the other two techniques. A randomized, controlled trial with a larger number of patients and a longer follow-up is needed to confirm the results obtained in this study.
ACKNOWLEDGEMENTS
Authors’ contributions: Study design and concept (Gigliola S, Sborgia G, Niro A); Manuscript preparation (Niro A);Data collection (Gigliola S, Sborgia G, Palmisano C, Puzo P,Giuliani G, Sborgia L, Sisto D, Pastore V, Furino C, Sborgia A,Boscia F, Alessio G); Data evaluation (all the authors).
Conflicts of Interest:Gigliola S, None; Sborgia G, None;Niro A, None; Palmisano C, None; Puzo P, None; Giuliani G, None; Sborgia L, None; Sisto D, None; Pastore V, None;Furino C, None; Donghia R, None; Sborgia A, None; Boscia F, None; Alessio G, None.
 International Journal of Ophthalmology2021年12期
International Journal of Ophthalmology2021年12期
- International Journal of Ophthalmology的其它文章
- Comparison of trifocal toric and bifocal toric intraocular lens implantation in patients with cataract and high corneal astigmatism
- Decreased retinal microvasculature densities in pterygium
- Fourier analysis of corneal Scheimpflug imaging: clinical use in keratoconus
- Establishment of a prediction tool for ocular trauma patients with machine learning algorithm
- Role of orthoptics and scoring system for orbital floor blowout fracture: surgical or conservative treatment
- Outcomes of half-width vertical rectus transposition augmented with posterior fixation sutures for sixth cranial nerve palsy