
Acupuncture in preventing postoperative nausea and vomiting:a systematic review and Bayesian network meta-analysis
2021-06-23 07:55:00ChengWeiFuQingShuYangJiaoTongWuAiQunSongQiaoChuZhuWeiPingZhang
TMR Non-Drug Therapy 2021年2期
Cheng-Wei Fu,Qing Shu,Yang Jiao,Tong Wu,Ai-Qun Song,Qiao-Chu Zhu,Wei-Ping Zhang
1The Second Clinical Medical School,Guangzhou University of Chinese Medicine,Guangzhou 510080,China.2Rehabilitation Department,Zhongnan Hospital of Wuhan University,Wuhan 430071,China.3Acupuncture and Moxibustion Department,Hubei Provincial Hospital of Traditional Chinese Medicine,Wuhan 430061,China.4Acupuncture and Moxibustion Department,Hubei Province Academy of Traditional Chinese Medicine,Wuhan 430074,China.5College of Acupuncture and Orthopedics,Hubei University of Traditional Chinese Medicine,Wuhan 430061,China.6Department of Medical Rehabilitation,Zhuji People’s Hospital of Zhejiang Province,Zhuji 311800,China.7Department of Medical Rehabilitation,Zhuji Affiliated Hospital of Shaoxing University,Zhuji311800,China.
Abstract Background:Some studies have suggested acupuncture therapy can prevent postoperative nausea and vomiting.However,the best choice of acupuncture therapy for postoperative nausea and vomiting remains controversy.Methods:Several databases were searched from inception to April 2020.Randomized controlled trials met the criterion were included.Risk of bias was implemented with Cochrane risk-of-bias tool.Addis,R,OpenBUGS and STATA were used to conduct meta-analysis.The evidence was assessed by GRADE profiler 3.6.Results:Fifty studies involving 5980 patients were included.The risk of bias of most included studies were acceptable.The results of network meta-analyses indicated,compared with placebo,electroacupuncture was the best choice for postoperative nausea(odds ratio=0.09,95%confidence interval:0.02-0.51)and acupoint plaster for postoperative vomiting(odds ratio=0.07,95%confidence interval:0.01-0.42),acupoint catgut embedding+5HTRA for postoperative nausea and vomiting(odds ratio=0.05,95%confidence interval:0.01-0.15),and transcutaneous electrical nerve stimulation+5-hydroxytryptamine receptor antagonists for postoperative rescue antiemetics(odds ratio=0.14,95%confidence interval:0.08-0.46).Conclusion:It was suggested transcutaneous electrical nerve stimulation+5-hydroxytryptamine receptor antagonists was the best choice.The results provided guidance for the prevention of postoperative nausea and vomiting.
Keywords:Acupuncture therapy,Postoperative nausea and vomiting,Network meta-analysis,Transcutaneous electric nerve stimulation
Background
Postoperative nausea and vomiting(PONV)is one of the most common complications,as a relevant data referred to its affecting 20%-40%of surgical patients[1].The physiologic mechanism of PONV is complex,involving multiple neurophysiologic pathways[1].Clinicians tend to regard that nausea and vomiting are two independent physiological reactions located in supratentorial regions and medulla respectively,which can be triggered by the same stimuli and mediated in part through same neural circuits[2].Some antiemetics have been developed to cope with PONV,nevertheless,only one third of patients can benefit from prophylactic medication with the cost-effectiveness less than satisfactory[3,4].For one thing patients have no better choice but to pay an extra expense to possibly avoid PONV,for another,discharge will be delayed along with an increasing financial burden once PONV appears[5-7].
Thus,the top priority is to develop a more efficient therapeutic scheme.Some clinicians have recommended the combination of medication and nonpharmacologic interventions like acupuncture therapy including acupressure,manual acupuncture(MA),and transcutaneous electrical nerve stimulation(TENS),with noteworthy superiority in preventing PONV as researches have proved[8-10].Excellent safety and efficacy make them possible to be alternative interventions for PONV[7,10,11].PC6 may be the most shared acupoint for stimulation which is originated from Chinese Medicine theory that most malaises related to stomach can be treated by Neiguan(PC6)[12].Some previous meta-analyses held that acupoint stimulation can prevent PONV[12-14].However,those studies mainly concentrated on using acupuncture therapy alone or the integration of acupuncture therapy and western medicine,lacking of comparison in different acupuncture therapies.Meanwhile,there is still controversial whether non-invasive regimens are as effective as invasive ones[15].To handle them with proper assessments will help remove the fetters of acupuncture’s wider application in PONV.For our primary aim,we tested the hypothesis that which acupuncture therapy can be the optimal solution.Secondly,we tested the comparability between non-invasive regimens and invasive ones.For the sake of solving these issues,we used network meta-analysis(NMA)based on Bayesian model and hope this study could inspire relevant study.
Methods
Ethics and eligibility criteria
This systematic review adhered to the Preferred Reporting Items for Systematic review and Meta-Analysis statement for NMA[16].As all statistical analyses in this study were performed based on previous studies,informed consent was not required.The prospective protocol was registered in INPLASY(https://inplasy.com/)with an identifier INPLASY202060108 and more details can be obtained from Medicine[17].Adult patients undergoing surgery within general anesthesia were included.Any acupuncture therapy in combination with antiemetics or not was included as interventions.Control group consisted of sham acupuncture therapy,antiemetics.But other complementary or alternative therapies were excluded.The outcomes were the incidences of postoperative nausea(PON),postoperative vomiting(POV),PONV and postoperative rescue antiemetics(POR).Postoperative 24 h was the primary endpoint.Studies without the prescribed primary endpoint would not be included as well.Moreover,we would not conduct the result if less than 5 studies described the same endpoints.
Search strategies
Authors searched PubMed/Medline,Cochrane library,Web of Science,Ebsco,Ovid/Embase,China National Knowledge Infrastructure,Wanfang Database,VIP Database and China Biology Medicine disc from setup time to April 2020.Search strategy was adjusted according to various databases and the detail was shown in Appendix 1.
Study selection
Two reviewers scanned all studies and a third reviewer requested adjudications if necessary.Only the most informative and complete study of any duplicate publications was selected.
Data extraction
After identification of the target randomized controlled trials(RCTs),one reviewer extracted the data into a database created by Excel 2019 and checked by the second reviewer including studies information,patient information and outcomes information.The third reviewer was the referee in case of doubts or disagreements.In addition,GetData Graph Digitizer was used to extract the number from graphic data.
Risk of bias assessment
Cochrane risk-of-bias tool(version 2.0)was used to evaluate the quality[18].Two reviewers used Cochrane risk-of-bias tool(version 2.0)to assess all matched studies and the third reviewer requested adjudicationsif necessary.
Statistical analysis
Only if 3 or more studies measured the same interventions directly,could pairwise meta-analysis be conducted.Stata 14.0 was used,and odds ratio(OR)and 95%confidence interval(CI)were adopted.Heterogeneity is quantified with theI2statistic.WhenI2>50%,a random effect model was adopted;if not,a fixed effect model.And before selecting model,sensitivity analysis was accomplished if enough studies were available.Begg’s testing was performed to explore the publication bias if necessary.NMA was performed by Addis 1.16.8,OpenBUGS 3.2.3,R 3.6.3 and STATA 14.0.As the incidence rate was dichotomous data,OR and 95%credible interval were adopted.Considering the extreme case report that response may be 0,we added 0.5 to event rate artificially.Clinical heterogeneity was assessed according to participants’characteristics,interventions and outcomes of the included trials.R was used to assess the methodological heterogeneity.It gaveI2to evaluate the pooled network heterogeneity.Convergence was evaluated by Potential Scale Reduction Factor according to the Brooks-Gelman-Rubin method.We assessed global inconsistency by fitting both inconsistency model and consistency model.Then,node spilt analysis was performed to assess local inconsistency by comparing direct and indirect effect.League figures were used to demonstrate the results of multiple treatment comparisons.The surface under the cumulative ranking curve(SUCRA)values were used to rank the probabilities ranged from 0 to 100%.Network funnel plot were conducted to assess the publication bias.
Quality of evidence was evaluated by the Grades of Recommendations Assessment Development and Evaluation guidelines.The quality was graded in very low,low,moderate and high by using GRADE profiler 3.6.
Results
Study characteristics
As showed in Figure 1,we retrieved 21,548 articles,with 8,893 duplicate articles removed.A total of 12,655 articles were eliminated by reading titles and abstracts and 821 articles by reading the full texts.Finally,50 RCTs published from 1997 to 2020 with 5,980 patients matched the final criteria through web search and selection.Among the selected literatures,TENS and acupressure were the top 2 most popular acupuncture therapies,with 1,212 patients employing the former and 582 patients the latter.In regards to acupuncture prescriptions,PC6 and Zusanli(ST36)were the main acupoints to prevent PONV and most stimulation were performed during preoperative period rather than postoperative period.Table 1 showed the general characteristics of included studies.
Methodological evaluation
The risk of bias assessment for the 50 RCTs was summarized in Table 2.The overall risk can be accepted;44 studies were assessed having low to moderate risk of bias.The main high-risk bias came from the measurement of the outcome.
However, enough cattle were left to make the young man rich, and he and his wife lived happily together, except that every now and then the girl vanished from his sight, and never told him where she had been
Pairwise meta-analysis of outcomes
The pairwise meta-analysis results concluded by Stata were displayed in Table 3.
In Table 3,8 studies compared TENSvs placebo and 4 studies compared TENS+5-hydroxytryptamine receptor antagonists(5HTRA)vs.5HTRA.In the fixed model,the OR of them were 0.40(95%CI 0.29-0.54)and 0.33(95%CI 0.20-0.55).Performed by random model,the OR of TENSvs placebo for the periods 0-6 h,6-24 h were 0.34(95%CI 0.20-0.57)and 0.49(95%CI 0.17-1.39).
Nine studies compared TENS vs placebo and 5 studies acupressure vs.placebo.The OR of them were 0.43(95%CI 0.31-0.59)and 0.53(95%CI 0.28-0.98).Performed by fixed model,the OR of TENS vs placebo for the periods 0-2 h,0-6 h and 6-24 h were 0.44(95%CI 0.18-1.08),0.46(95%CI 0.32-0.68)and 0.49(95%CI 0.32-0.76).
Compared with placebo,the OR of TENS,5HTRA were 0.38(95%CI 0.29-0.49)and 0.47(95%CI 0.30-0.73),respectively.Compared with 5HTRA and TENS,the OR of TENS+5HTRA were 0.27(95%CI 0.15-0.50)and 0.25(95%CI 0.14-0.45).Begg’s test didn’t find publication bias(P=0.193).
Compared with placebo,the OR of TENS,acupressure and 5HTRA were 0.47(95%CI 0.36-0.62),0.35(95%CI 0.11-1.10),and 0.21(95%CI 0.11-0.42),respectively.Compared with 5HTRA,the OR for TENS and TENS+5HTRA were 0.59(95%CI 0.59-1.16)and 0.38(95%CI 0.21-0.69).Begg’s test didn’t find publication bias(P=0.107).
NMA of primary outcomes
The NMA results were displayed in Figure 2(network plot),Figure 3(SUCRA),Figure 4(league figure)and Figure 5(network funnel plot).
In Figure 2,PON was measured by 23 RCTs using 11 treatments.The specifc outcome was shown as league figure.Both single therapy(electroacupuncture(EA),acupressure,TENS,acupoint plaster(AP),acupoint injection(AI),5HTRA)and combined therapy(TENS+5HTRA,acupressure+5HTRA)had a better clinical effective rate than placebo.The differences among the above interventions were statistically signifcant.In Figure 3,it suggested that EA(SUCRA:82.2%)was the optimal treatment,followed by AI(SUCRA:80.9%)and AP(SUCRA:80.1%).Visual inspections showed that the eligible RCTsshowed symmetry in the funnel plot of PON.
A total of 24 RCTs with 11 treatments observed POV in postoperative 24 h.Compared with placebo,only dopamine receptor antagonists(D2RA)+5HTRA and MA could not work to POV’s benefit.Based on the SUCRA values,AP(SUCRA:84.6%)ranked as the best treatment,EA(SUCRA:84.4%)and TENS+5HTRA(SUCRA:80.0%)were the second and third best treatments,respectively.Publication bias of POV could be accepted in terms of the network funnel.
Twenty-five RCTs with 13 treatments reported incidence rate of PONV.Apart from MA,EA and acupressure+5HTRA,all therapies could lift the capacity of restrain According to the SUCRA values,ACE+5HTRA(SUCRA:90.9%)was the best treatment.The second and third most effective interventions were D2RA(SUCRA:81.5%)and EA+5HTRA(SUCRA:76.9%).Publication bias of PONV could not be detected in the network funnel of PONV.
The outcome of POR is reported in 26 RCTs with 9 treatments.As seen in Figure 4,compared with placebo,all included therapies could reduce using POR.TENS+5HTRA(SUCRA:78.5%)was the most favorable intervention,and EA(SUCRA:77.4%)was the second favorable intervention and acupressure+5HTRA(SUCRA:71.5%)was the third based on the SUCRA values.The asymmetry suggested potential publication bias.
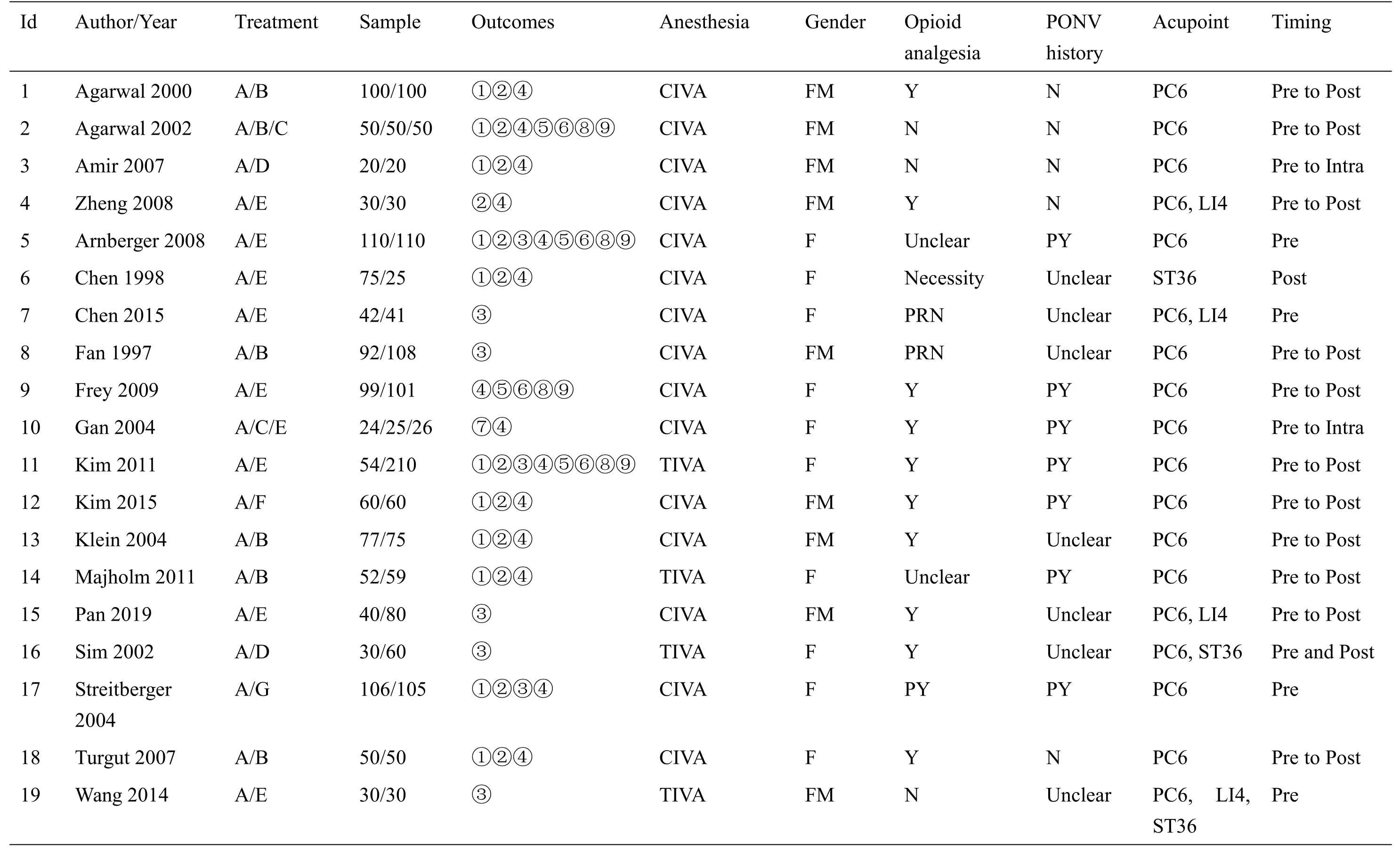
Table 1 Characteristics of enrolled studies

Table 1 Characteristics of enrolled studies(Continued)
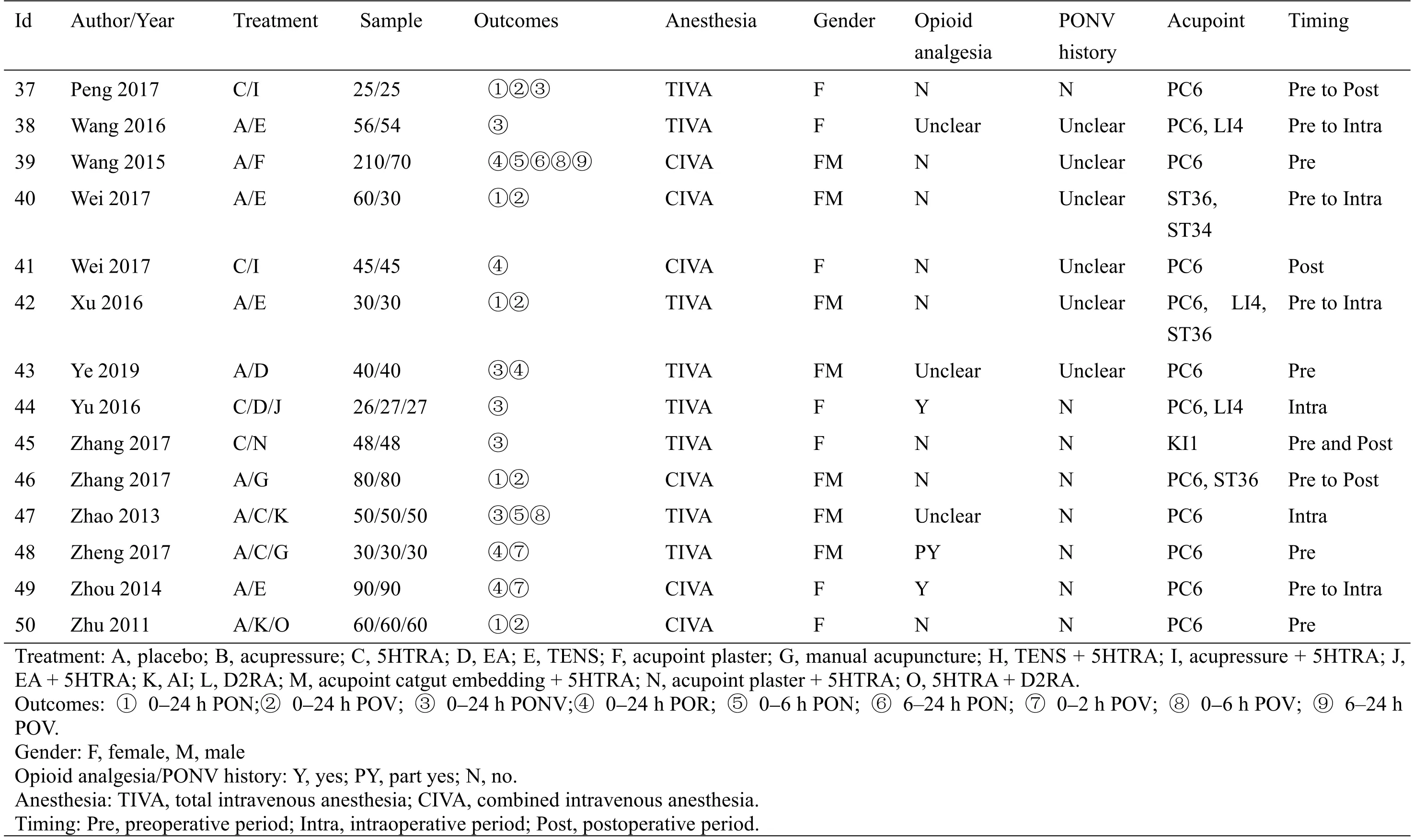
Table 1 Characteristics of enrolled studies(Continued)
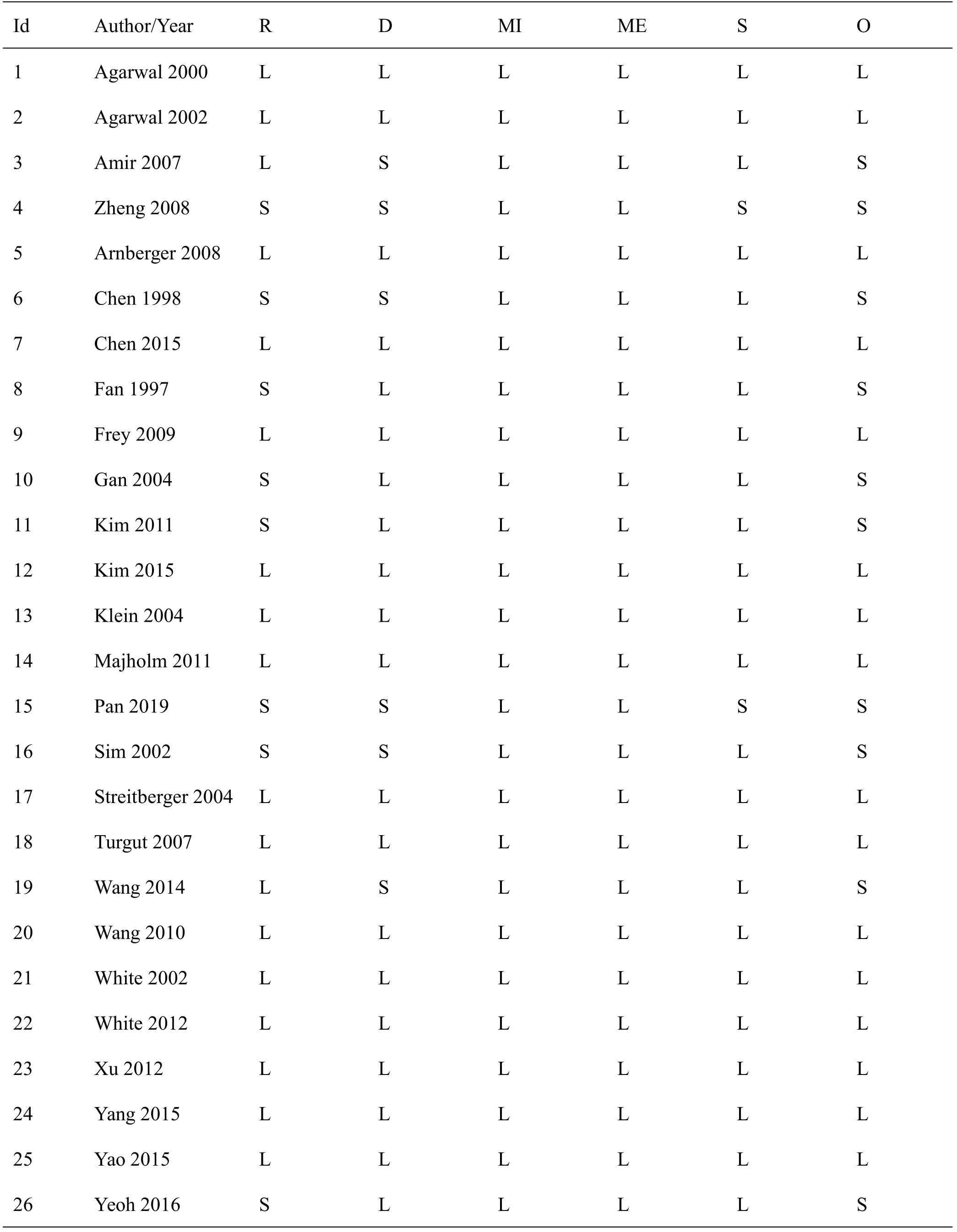
Table 2 Quality evaluation of enrolled studies
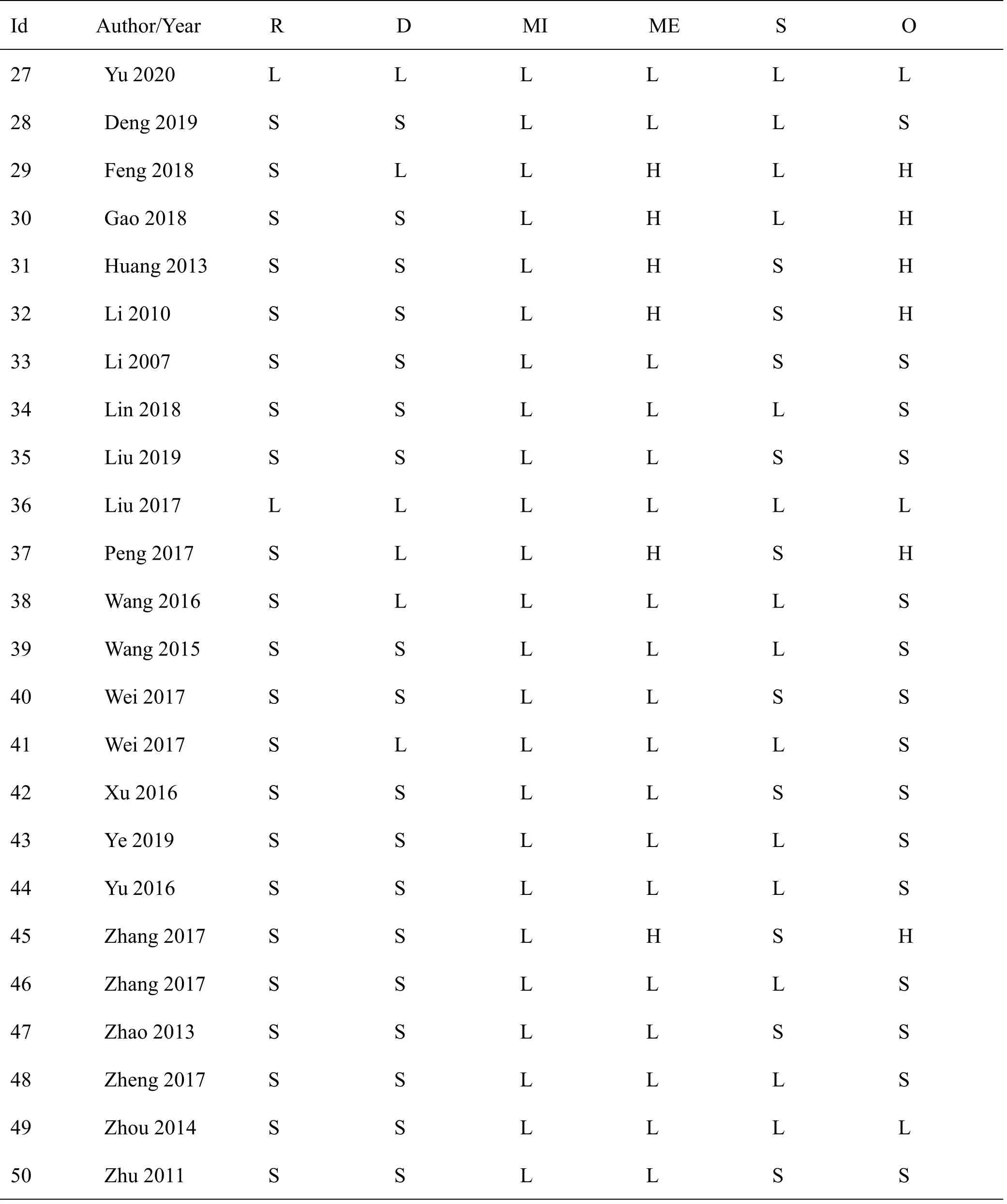
Table 2 Quality evaluation of enrolled studies(Continued)
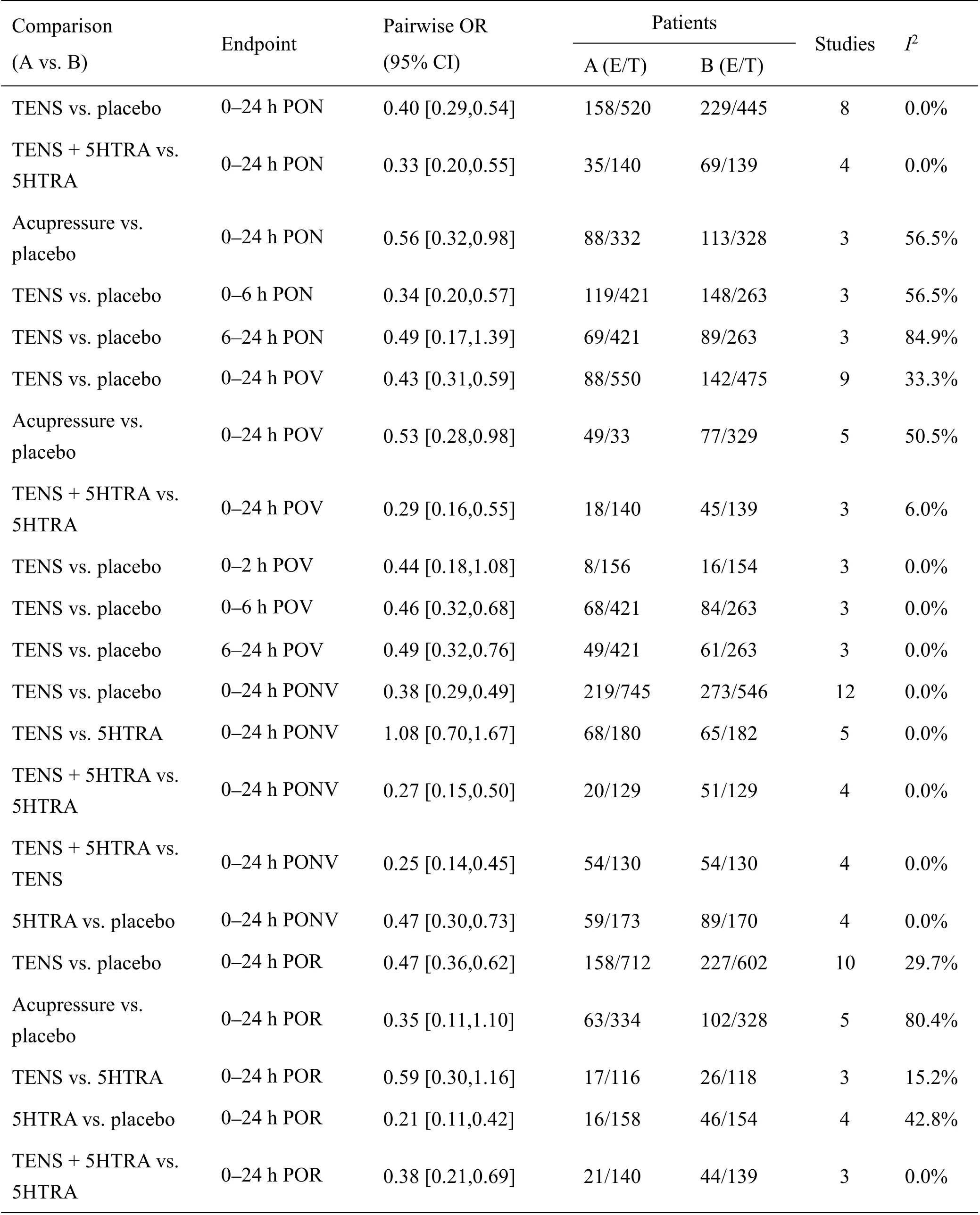
Table 3 Pairwise meta-analysis
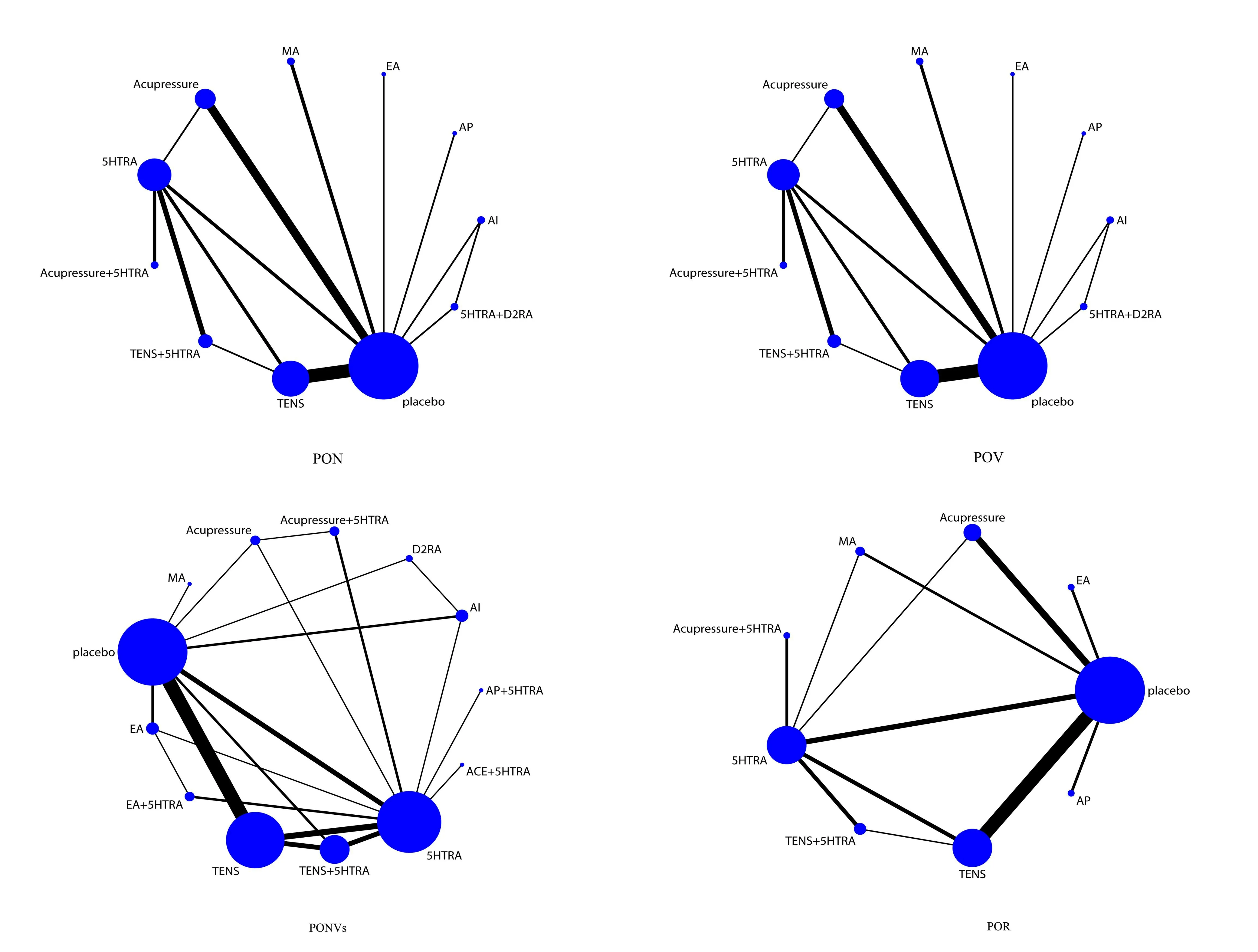
Figure 2 Network plots of primary outcomes.5HTRA,5-hydroxytryptamine receptor antagonists;AI,acupoint injection;AP,acupoint plastering;D2RA,dopamine receptor antagonists;EA,electroacupuncture;MA,manual acupuncture;TENS,transcutaneouselectric nervestimulation.
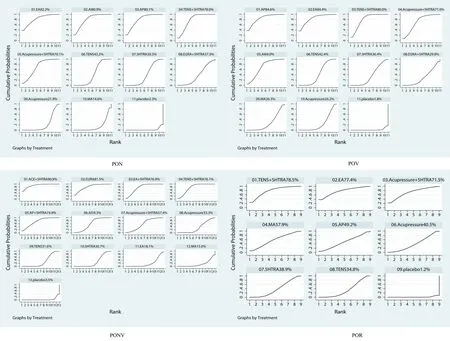
Figure 3 SUCRA of primary outcomes.5HTRA,5-hydroxytryptamine receptor antagonists;AI,acupoint injection;AP,acupoint plastering;D2RA,dopamine receptor antagonists;EA,electroacupuncture;MA,Manual Acupuncture;TENS,transcutaneouselectric nerve stimulation.
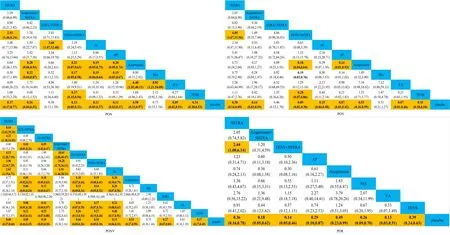
Figure 4 League figure of primary outcomes.5HTRA,5-hydroxytryptamine receptor antagonists;AI,acupoint injection;AP,acupoint plastering;D2RA,dopamine receptor antagonists;EA,electroacupuncture;MA,Manual Acupuncture;TENS,transcutaneouselectric nerve stimulation.

Figure 5 Network funnel of primary outcomes.5HTRA,5-hydroxytryptamine receptor antagonists;AI,acupoint injection;AP,acupoint plastering;D2RA,dopamine receptor antagonists;EA,electroacupuncture;MA,Manual Acupuncture;TENS,transcutaneous electric nerve stimulation.
NMA of secondary outcomes
The NMA results concluded are displayed in Appendix 2.
Eight RCTs reported PON in postoperative 6 h.Compared with placebo,AI(SUCRA:97.3%),TENS+5HTRA(SUCRA:73.1%)and TENS(SUCRA:40.3%)had better performance.Six RCTs reported PON in postoperative 6-24 h,and none of them had difference compared with placebo,TENS+5HTRA(SUCRA:70.2%)may be the best choice.
Five RCTs reported POV in postoperative 2 h,compared with placebo,MA(SUCRA:83.4%)and 5HTRA(SUCRA:67.9%)could prevent POV.
Eight RCTs tested the incidence of POV in 6 h,and the findings indicated that AI,AP and TENS can restrain POV,with their SUCRA came as 97.2%,43.0%and 31.8%respectively.A total of 6 studies reported in 6-24 h POV,and only TENS was better than placebo but TENS+5HTRA was the best choice as SUCRA suggested.
Quality of evidence.
The Grades of Recommendations Assessment Development and Evaluation summarized 21 items of evidence about acupuncture therapy in preventing PONV with an assessment of moderate,low and very low,and each of them has 7 items.None of acupuncture therapy were regarded as high-quality evidence.Appendix 3 gave out the items of evidence.
Discussion
PONV,a common but persistent problem,has extremely troubled clinicians and patients for years.A series of antiemetics have been developed,but the adverse effect cannot be neglected.Therefore,the latest guidelines have pointed out that there is no difference between acupoint stimulation and rescue antiemetics in preventing nausea and vomiting,and a combination of the above two methods may bring about extra benefits[7].The aim of this review is to figure out best regimen of acupuncture to fit in clinical needs.
A total of 50 studies were finally included and the risk of bias of this review can be accepted,because most of them are low to moderate risk.High-risk studies are due to inadequate outcomes reported with a state of unblinding.
With respect to primary outcomes,some inspiring evidence have been concluded as follow.We found that TENS,acupressure,5HTRA and TENS+5HTRA can prevent PON,POV,PONV and reduce the application of POR when comparing with placebo.The outcomes still demonstrated a superiority of treatments like acupressure+5HTRA,AP and EA in preventing PON,POV and PONV.AI was superior to placebo in preventing PON,POV and reducing the application of POR.The results maintained consistency with previous studies[12-14,19].When taken SUCRA and network OR into consideration,TENS+5HTRA should be the best choice with high ranks.Obviously,the combining therapy may have synergistic effects of TENS and 5HTRA,which had a positive uniformity with the guidelines[7].A potential hypothesis may be the explanation that both TENSand 5HTRA could change the concentration of serotonin which will activate the vomiting reaction[20-23].But we need more direct comparisons between TENS+5HTRA and placebo to suppose.Furthermore,TENS could modulate the sedative effect of propofol[24].AP and AI also revealed their effectiveness,while the both can combine drug effect with acupoint stimulation.Network OR value showed that the effect of APand AI were comparable and SUCRA showed that compared with AP,AI was better in preventing PON but worse in preventing POV.5HTRA and D2RA was used in AI.It said that AI may have an enhanced effect of the medication administered through acupoint stimulation[25,26].Capsaicin and evodiae were adopted in AP.Capsaicin was found to inhibit 5-hydroxytryptamine receptor expressed like 5HTRA[27].In contrast,evodiae as an herbal antiemetics based on theory of Chinese medicine could strengthen the expression of 5-hydroxytryptamine on the grounds of scientific researches,inferring that another mechanism for preventing PONV remains open to question[28,29].MA,the classical regimen,could not decrease the incidence of PONV while reducing antiemetics.The assumption may come up with that not all patients with PONV need antiemetics.Once the intensity of PONV exceeds the threshold,patients need antiemetics,indicating that the application of MA may lift the threshold of using antiemetics rather than nausea and vomiting.Such inferences still need further clinical confirmation.Admittedly,TENS may be the most popular
Besides,acupoints were taken into analysis as well.It should be noted that PC6,ST36 and Hegu(LI4)are the main acupoints in included studies.In Chinese Medicine theory,all of them can modulate qi mechanism,inhibit qi counterflow of stomach.PC6 can relieve the intensity of nausea while PC7 and GB37 cannot,the mechanism may associate with the modulation of coupling between the cerebellum and insula,which is the specific neural basis[30].EA and AI at ST36 can facilitate colonic transport and relieve gastrointestinal conduction disorder and it may be related to PKC and MAPK signal transduction pathways[25,31,32].In rats of labour pain,LI4 could enhance protein expression ofκ-opioid receptor and prodynorphin and the effect is similar to meperidine[33].It revealed that LI4,as an analgesic acupoint,may prevent PONV by reducing the use of opioid.In addition,Alizadeh’s study held that acupoints combination was better than acupoint alone in preventing PONV[34],but our study did not find similar conclusion.Thus,we will discuss the synergy and antagonism of acupoints in next study to assist in clinical decision.
Moreover,our review showed that the effects of invasive and non-invasive therapies are equivalent.However,Enzo’s study held that non-invasive therapy may have weaker effects than invasive ones[35].The discrepancy may be ascribed to distinct research themes:Enzo’s study aimed at nausea and vomiting induced by chemotherapy while ours focused on PONV.Based on our results,a non-invasive therapy is more recommended because bleeding and pain are still worthy of attention when using invasive therapy[36].
Nevertheless,the secondary outcomes are not as satisfactory as primary outcomes.Overbroad range of CI can lead to deviation of statistical results,because only a few studies reported the response during these periods.We desire that future trails can divide each time period in detail to provide reliable evidence for decision-making.
There are still some limitations in this review.For instance,inadequate studies applying AI and APmade it arduous to draw a definitive conclusion.What’s more,the timing of the onset of stimulation and the duration of stimulation is still ambiguous.And these points mentioned lead to aftermath that the quality of evidence should be treated with caution.To solve above limitations,future acupuncture clinical trials should follow the Standards for Reporting Interventions in Clinical Trials of Acupuncture[37].Various parameters like frequency and course of treatment should attempted to determine the efficacy[38]and take the advantages and disadvantages of all aspects into consideration.
Conclusion
With clinical evidence summarized by this review,it is observed that TENS+5HTRA may be the best treatment,and APand AI should get more attentions to confirm the effect.The results could be rewarding for clinical practice.Further research should be promoted by health policy makers,researchers and clinicians.

- TMR Non-Drug Therapy的其它文章
- Research on acupuncture treatment of chronic stable angina by Chinese scholars
- Electroacupuncture in perioperative anesthesia and analgesia management:a non-invasive adjuvant treatment
- Research on acupuncture treatment of episodic migraine without aura by Chinese scholars
- Integrating cupping therapy in the management of tinnitus and dizziness:a pilot study
- The effect of dry-cupping combined with lavender oil massage on postpartum perineal pain:a case study