
Informal caregivers’ quality of life and management strategies following the transformation of their cancer caregiving role:A qualitative systematic review
2021-05-19 08:05:54YingyingCaiAlisonSimonsSamanthaTolanJunfengZhangKexinZheng
Yingying Cai ,Alison Simons ,Samantha Tolan ,Junfeng Zhang ,Kexin Zheng
aDepartment of Chemotherapy,Jieyang People's Hospital,Jieyang,Guangdong,China
bSchool of Nursing and Midwifery,Faculty of Health,Education and Life Sciences,Birmingham City University,Birmingham,United Kingdom
cDepartment of Nursing Administration,Dongguan Songshanhu Central Hospital,Dongguan,Guangdong,China
dDepartment of Mental Health,Zhuhai City Center of Chronic Disease Control,Zhuhai,Guangdong,China
ABSTRACT Objectives:Globally,informal caregivers caring for cancer patients meet challenges within their caregiving role,which significantly influence their quality of life.This qualitative systematic review aimed to analyze how cancer caregiving influence the quality of life of informal caregivers and the management strategies of informal caregivers for their role as cancer caregivers.Methods:Following the enhancing transparency in reporting the synthesis of qualitative research(ENTREQ) statement,Wanfang database,the China National Knowledge Infrastructure (CNKI),CINAHL,MEDLINE,PubMed,Cochrane Library,PsycARTICLES and PsycINFO,and grey literature in English and Chinese from 1 May 2009 to 31 December 2019 were searched.Quality of included studies was assessed by the Critical Appraisal Skills Programme (2018) Qualitative Checklist and thematic synthesis was conducted.Results:Of the 8,945 studies identified,6 studies met the inclusion criteria.One analytical theme relating to the QoL of informal caregivers following cancer caregiving was identified:“challenges of caregiving”.In terms of the management strategies to the role of cancer caregivers,two analytical themes were identified:“self-adjustment”and“seeking for formal and informal support”.Conclusions:Cancer caregiving influences informal caregivers’ QoL significantly and informal caregivers develop diverse coping strategies to deal with the difficulties occurred while balancing the relationship between their own lives and caregiving.However,professional and policy support remain inadequate for informal caregivers that require the need for improvement in terms of health care professionals and policymakers.
Keywords:Caregivers Neoplasms Psychological adaptation Quality of life Social adjustment
What is known?
· Globally,the burden of cancer care is expected to increase notably in the future.
· Informal caregivers take the major responsibilities to take care of cancer patients,which could lead to negative impacts on the quality of life (QoL) of both cancer patients and informal caregivers.
· Considerable quantitative research has been conducted in investigating the current status of the QoL of informal caregivers.
What is new?
· Comprehensive assessment of the QoL of informal caregivers and their needs is essential when they begin their caregiving role.
· Short-term demand-oriented training programme is required because it could help informal caregivers adapt to their cancer caregiving role as soon as possible.
· Health care professionals should choose different support strategies according to the needs of informal caregivers.
· Professional and policy support are inadequate and improvement is needed.
1.Introduction
Globally,cancer is a huge challenge because it is the main cause of morbidity [1]and the second leading cause of mortality [2].In 2018,18.1 million people were diagnosed with cancer [3].Fortunately,because of early detection and diagnosis as well as better screening and treatments,cancer survival rates have been significantly improving and an increasing number of people survive [4].Therefore,with both morbidity and survival rates of cancer increasing,the number of cancer patients may continue to rise,and the burden of cancer care worldwide is expected to increase notably in the future.
Within the last few decades,there has been a tendency toward shorter hospital stays,and a growing number of cancer patients are now being cared for by family caregivers at home,rather than in hospitals [5].Even during cancer treatment in hospitals,family caregivers are still required for daily care [6].Hence,cancer patients' home caregivers,called“informal caregivers,”are taking major responsibilities for cancer patients’ care [7,8].These caregivers,the majority of whom are relatives,friends,and partners[9],provide uncompensated and informal care to cancer patients [10].As cancer patients become unable to perform activities of daily living [11],informal caregivers not only need to assume cancerrelated responsibilities,including treatment management and symptom monitoring,but also to undertake additional daily assistance in activities such as cooking and toileting[12].Nevertheless,because informal caregivers lack professional skills and knowledge of caregiving [13],they can be under great stress [14],causing deterioration in quality of life (QoL) for both cancer patients and their informal caregivers [5,15].
QoL is a multidimensional concept [16]that includes physical,social,psychological,and spiritual well-being [17].The reported prevalence of anxiety and depression among cancer informal caregivers is much higher than that of cancer patients themselves and caregivers who did not care for cancer patients[5,18],which is likely to reflect the deterioration of both physical and social wellbeing.Because of cancer caregiving,informal caregivers often experience sleep disturbances and fatigue [15]or even negatively change their health behaviors,including reducing daily intake of vegetables and fruits and increasing smoking and alcohol use[19].These changes might lead to deterioration in their weight,appetite,and physical strength,which could eventually worsen their own physical well-being,especially those who have been diagnosed with other diseases,such as heart disease,hypertension,and arthritis,before becoming informal caregivers [20].As their own physical well-being worsens,informal caregivers are less likely to provide high-quality caregiving for cancer patients,which would reduce the QoL for cancer patients [21].Meanwhile,because caregiving costs a large amount of unexpected time [22],informal caregivers have to reduce time spent on leisure and social activities,therefore leading to more physical problems and decreased social well-being [23].Furthermore,social isolation and the lack of physical activities might result in a high risk of anxiety and depression,which is likely to worsen their physical symptoms as well as their experience of isolation[24].Thus,each domain of the QoL of informal caregivers could affect the others,and their negative changes mentioned above are part of the reasons resulting in this vicious circle which may worsen without clinical interventions.
To improve informal caregivers' QoL,better understanding of how cancer caregiving influences their QoL and their management strategies for the role of cancer caregivers is essential.However,Chantarasap et al.[25]and Duan et al.[10]highlighted that the QoL of informal caregivers is often overlooked by health professionals and informal caregivers themselves,especially in the Asia Pacific Zone.In addition,to date,a great number of contemporary studies in the field of QoL of informal caregivers are quantitative research,using QoL scales to conduct cross-sectional surveys [16,26].This quantitative methodology tends to allow researchers to investigate the current status of the QoL of informal caregivers by using objective numbers[27]instead of exploring how cancer caregiving influences informal caregivers' QoL and how they make decisions during caregiving.To date,because there is no qualitative systematic review investigating the QoL of cancer informal caregivers,therefore,a qualitative systematic review is needed to integrate current studies and better understand informal caregivers’ QoL.Consequently,the aims of this qualitative systematic review are to analyze how cancer caregiving influences the QoL of informal caregivers and the management strategies of informal caregivers for their role of cancer caregivers.
2.Methods
2.1.Search strategy
The enhancing transparency in reporting the synthesis of qualitative research (ENTREQ) statement [28]was followed.Literature published from 1 May 2009 to 31 December 2019 was searched.The search was limited to 1 May 2009 onward because a great quantity of data demonstrated that the cancer field has developed rapidly [29]and informal caregivers’ QoL and management strategies have changed accordingly[30].The search strategy was developed based on the PEO(Population,Exposure,Outcome)framework,the relevant Medical Subject Headings (MeSH) terms,and free text including three themes:“caregiver,”“neoplasms,”and“quality of life”(see Table 1 and Appendix A).Eight bibliographicdatabases were searched,including the Wanfang database,the China National Knowledge Infrastructure (CNKI),CINAHL,MEDLINE,PubMed,Cochrane Library,PsycARTICLES,and PsycINFO.Grey literature was searched through three links:(a) Grey Literature Network Service,(b) Open System for Information on Grey Literature in Europe and(c)ProQuest Dissertations&Theses.To identify additional studies,both backward and forward citation chaining searching were conducted.
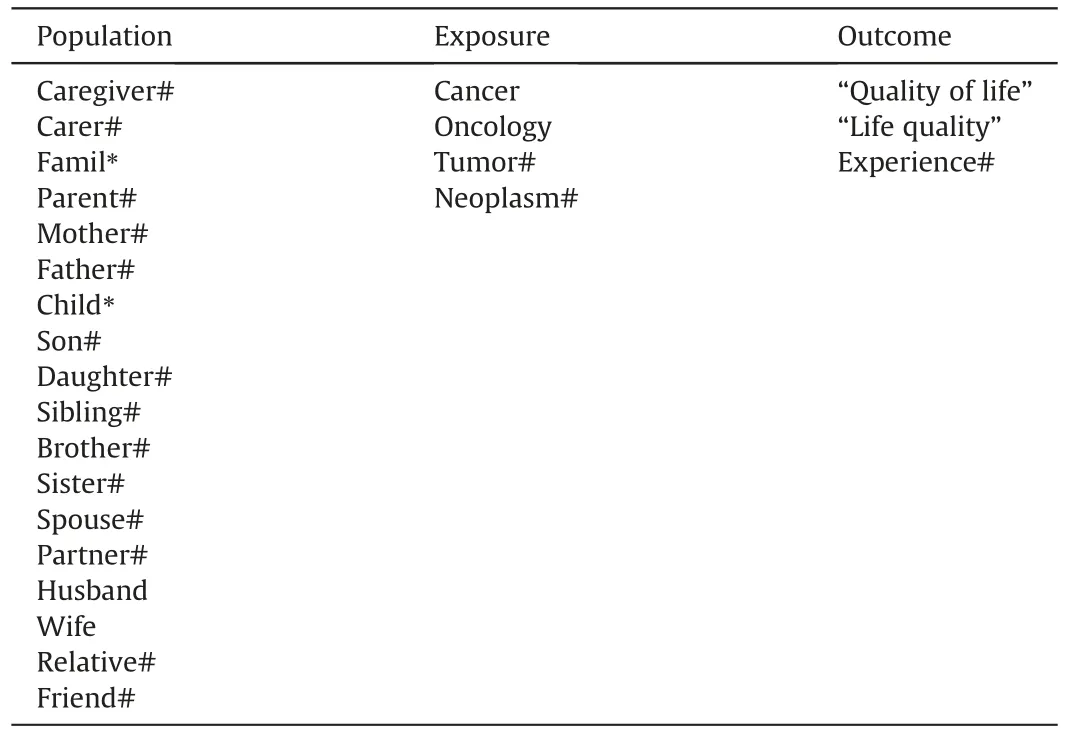
Table 1 Three key search terms and synonyms developed for the search strategy.
2.2.Inclusion and exclusion criteria
The inclusion and exclusion criteria were as follows:1)Types of population:Informal caregivers(≥18 years old),including relatives or non-relatives,caring for cancer patients were included.The reason for excluding informal caregivers younger than 18 years old is that they are minors who are experiencing a special psychological development stage [31]and caring for cancer patients may have more negative impacts on their QoL [32].This experience could result in higher risk for developing behavioral and emotional problems [31],which may be different than the adult experience.Furthermore,informal caregivers who had attended training related to caring or were employed were excluded.Informal caregivers caring for cancer patients who were diagnosed with any type and stage of cancer,either undergoing cancer-related treatments or not.2)Types of outcome:Any studies analyzing the QoL of informal caregivers related to cancer caring.Studies that investigated both QoL and any other phenomena were included if the data were reported separately.Studies that identified QoL of both cancer patients and their informal caregivers were included if the findings were reported separately.Any mixed-method studies were included if the qualitative data were reported separately.3) Types of study design and language:Only qualitative studies published in English or Chinese were included because of limited translation resources.Because the quantity of excluded studies published in other languages might affect the precision of the review [33],we documented any excluded studies.
2.3.Study selection
All citations were exported to EndNote.After duplicates were removed,all citations were screened via titles and abstracts,and the full text of all relevant studies identified was obtained and assessed by two reviewers independently,according to the inclusion and exclusion criteria.Discrepancies were discussed with the third reviewer to achieve consensus.
2.4.Quality assessment
To evaluate the trustworthiness of each study,the Critical Appraisal Skills Programme (CASP) [34]Qualitative Checklist was used for quality assessment by two reviewers independently.The 10 questions of CASP Qualitative Checklist consist of two parts:the first two screening questions are designed for briefly estimating the correlation between objectives and methodology of the study;the other eight questions are utilized to evaluate the methodology of the study comprehensively.Although low-quality studies tend to have higher risks of bias[35],they may also provide significant and valuable information[36].Therefore,the results of quality assessment were not used as an inclusion criterion and no study was excluded.Discrepancies were discussed with the third reviewer to reach consensus.
2.5.Data extraction
Data from the included studies,including bibliographic information,methodology,characteristics of population,exposure,and outcome information,were extracted by two reviewers independently.Disagreements were discussed with the third reviewer to reach consensus.
2.6.Data analysis and synthesis
The thematic synthesis method was chosen because it can identify similarities and differences among studies while generating new findings at higher levels of analysis [37],which enabled reviewers to analyze studies for implications for clinical practice and further research[38].The guideline developed by Thomas and Harden [39]was followed.The process of thematic synthesis was divided into three stages.1) The“l(fā)ine-by-line”coding of the text:All quotations were examined with coding text line by line.2)The identification of“descriptive themes”:The meanings of initial codes were analyzed and descriptive themes were developed.3)The synthesis of“analytical themes”:The descriptive themes were identified and analytical themes then developed.This process was conducted by three reviewers and disagreements were discussed with the fourth reviewer to achieve consensus.The data synthesis strategy was carried out using NVivo 11th software to code,store,and search qualitative data,which could minimize data-entry errors[40].Finally,no disagreements occurred among the reviewers.
3.Results
3.1.Description of studies
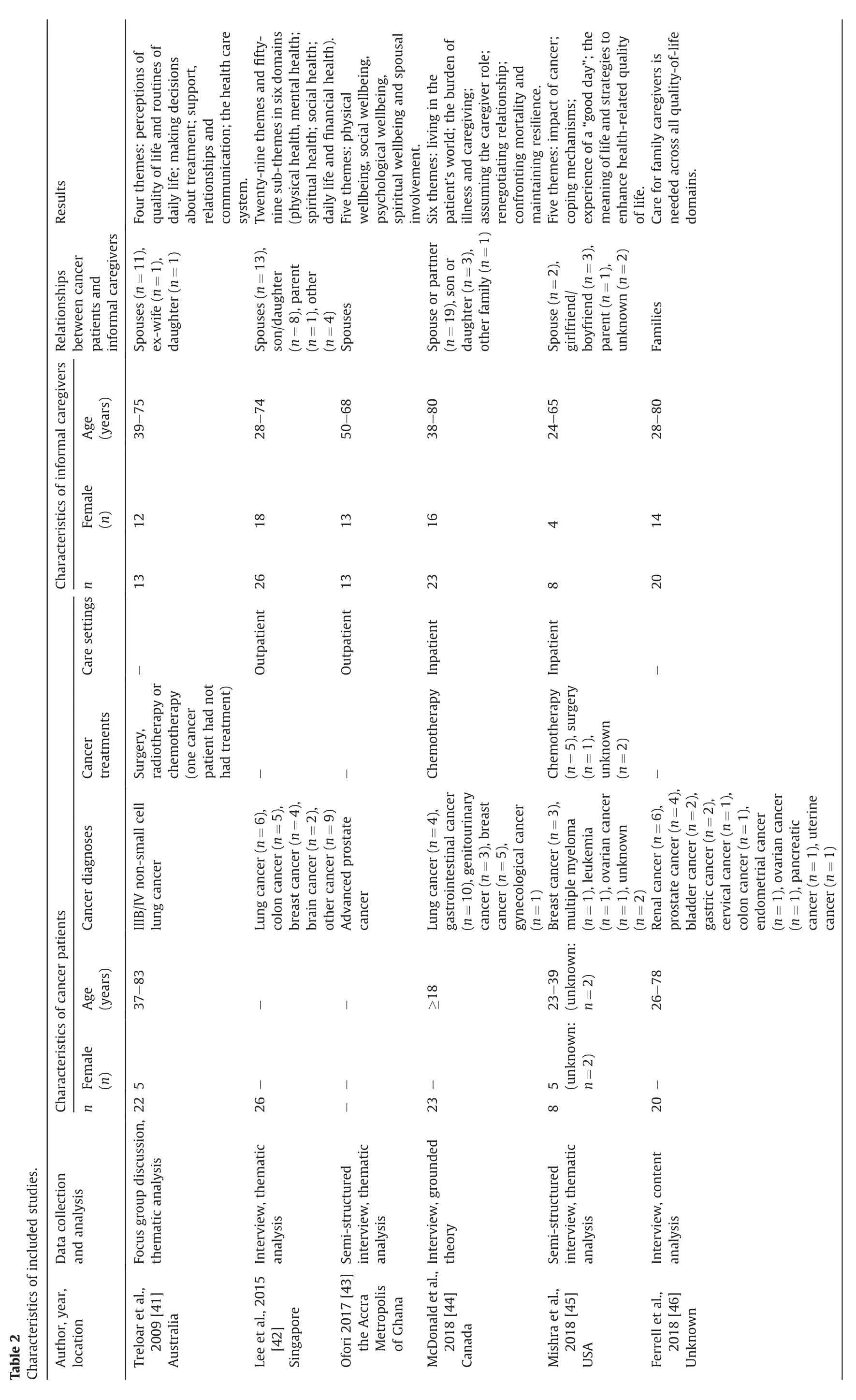
Of the 8,945 studies identified,6 studies met the inclusion criteria (see Fig.1 and Appendix B-The seven excluded studies after assessing eligibility and reasons of exclusion) and no non-English or non-Chinese study was excluded when reading the full text.The included studies,including a total of 103 caregivers,were from Australia [41],Singapore [42],the Accra Metropolis of Ghana[43],Canada [44],and the United States [45],and one of these studies’location remains unknown[46].Different cancer diagnoses(in total 18 cancer types),cancer treatments(surgery,radiotherapy,and chemotherapy),care settings (inpatient and outpatient),and relationships between cancer patients and caregivers (spouses,parent,son/daughter,or boyfriend/girlfriend) were obtained (see Table 2).
The quality assessment results revealed that two studies[41,46]did not define why qualitative methodology was used and how data analysis was conducted,and only three studies [42-44]critically examined the role of researchers and identified potential bias related to researchers.Despite these faults,all included studies were of medium or high quality (see Table 3).
3.2.Findings
Based on the two aims of this review about the QoL of informal caregivers following cancer caregiving and the management strategies of informal caregivers for their role of cancer caregivers,three analytical themes were identified:(a) challenges of caregiving,(b)self-adjustment,and(c)seeking for formal and informal support (see Table 4 and Appendix C-Data synthesis process).
3.2.1.The QoL of informal caregivers following cancer caregiving
Challenges of caregivingemerged as the analytical theme,indicating the difficulties in changing to the role of caregiver and the process of caregiving.
As part of the analytical theme“challenges of caregiving,”four descriptive themes were identified:(a) Physical well-being:Conflicts between needs of cancer patients and informal caregivers,(b)Social well-being:Role adjustment and financial burden,(c)Psychological well-being:The complexity of psychological changes,and (d) Spiritual well-being:Traditional values.These four descriptive themes are discussed below.
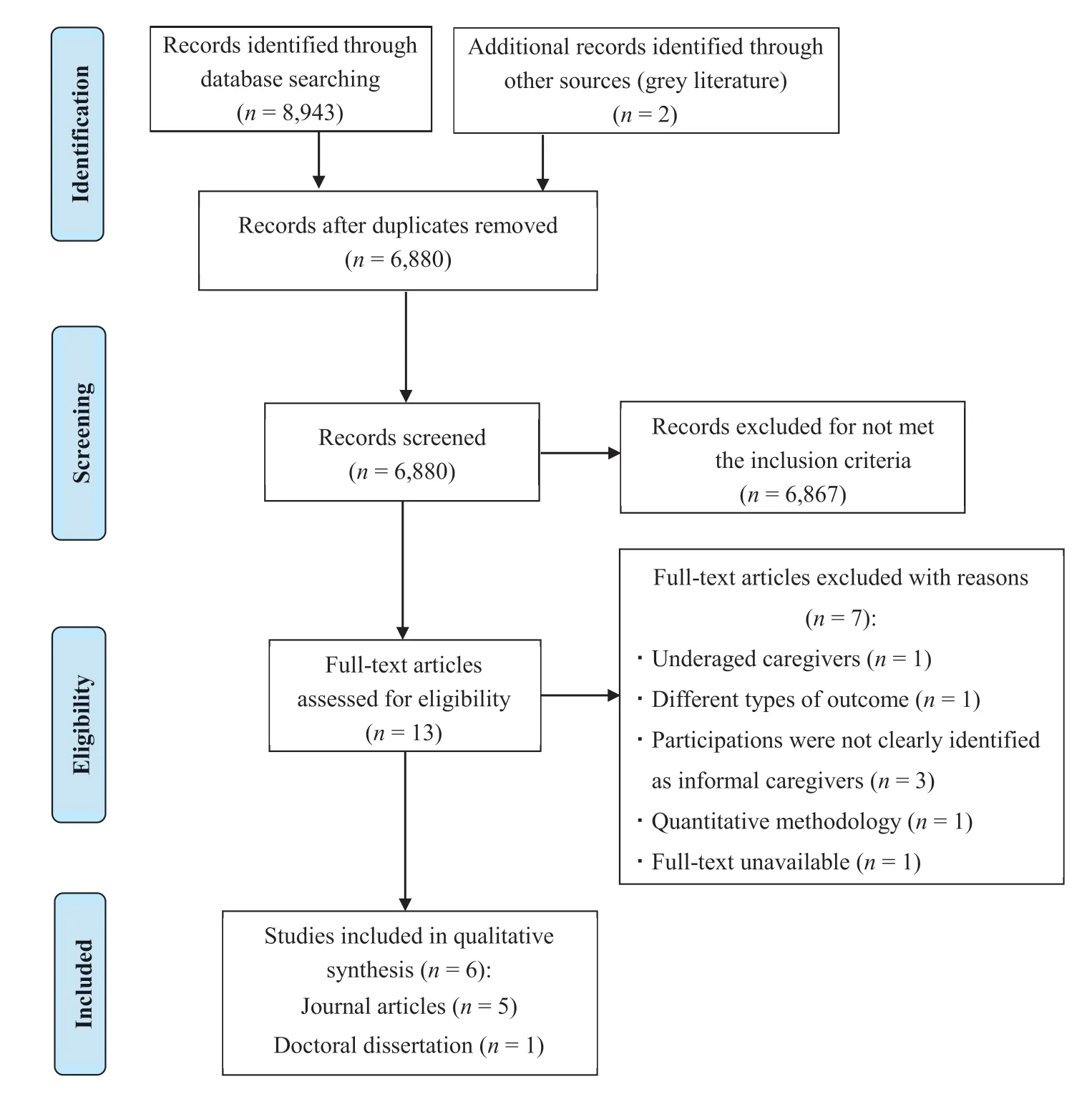
Fig.1.Flow chart of the literature search and selection process.
3.2.1.1.Physical well-being:conflicts between needs of cancer patients and informal caregivers.In taking care of cancer patients,informal caregivers found difficulties in balancing their own needs and cancer patients’needs.Because of caregiving activities,such as massaging and lifting cancer patients,informal caregivers experienced work overload,which led to a lack of time to rest or even to the deterioration of their own health status [42,43].As informal caregivers reduced their amount of sleep,they tended to experience insomnia,tiredness,headaches,pain in different body parts,cough,distress,memory deterioration,high blood sugar,and low or high blood pressure [42-45].For those informal caregivers who were diagnosed with chronic diseases before becoming cancer caregivers,the symptoms of chronic diseases were aggravated,such as the cough of asthma,leading to chronic disease exacerbation[43,44]:
“I have pains in my chest.I cough.The cough is persistent...I have been there(hospital)several times.One doctor told me to be careful of the food I eat.So I have noticed that when I eat rice or yam,I suffer the coughs.”([43];p.43)
3.2.1.2.Social well-being:role adjustment and financial burden.From the time when patients were diagnosed with cancer,informal caregivers had no choice but to transform their roles,living with cancer patients not only as family members but also as caregivers[41-46].As family members,first of all,informal caregivers paid close attention to cancer patients’psychological changes and tried to maintain them in a positive frame of mind[41-44,46].However,the unpredictable shift of psychological changes and changed personality in cancer patients,resulting from the diagnosis of cancer or cancer treatments,were hard to understand and manage by both parties [44,46].Meanwhile,because cancer patients were unable to work because of the disease,informal caregivers had to earn more money to pay for the costs of daily life,for example,food or school fees for their children,to which both parties would otherwise contribute,in addition to the high cost of cancer-related treatments,including medication,laboratory tests,overnight hotel stays,restaurant meals,and transportation to hospitals[42,43,45,46].However,to balance the relationship between work and caregiving,informal caregivers were forced to adjust their fulltime job to part-time work or even abandon their job,resulting in sadness and anxiety about future health care coverage[41-44,46]:
“When his sickness started and it was not severe,I did go and stand in for him.Because some of these things,you see at as physical but the spiritual aspect is also there.So whilst dealing with the physical,you also deal with the spiritual.”([43];p.65)
“I do miss the work.I think if mom had been living in [the same province]when she was first diagnosed,I probably wouldn't have had to quit,but having to be off for six months,that's a long time to have a leave of absence.”([44];p.73)
Informal caregivers need to assist cancer patients not only in conducting daily activities,for example,eating,toileting,bathing,and dressing,but also in planning for cancer-related matters,including making appointments and taking medications[41-43,46].In addition to their household role or original caregiver role in taking care of other people,for example,their children or grandchildren,informal caregivers reported more difficulties in managing the additional transformation to the cancer caregiving role[43,46]:
“He is not able to eat,or stand or sleep either.So my children and I hold him as a baby.We bathe him on the bed and do everything else for him… Sometimes,he's like a baby,so you can be easily fed up with him.Even feeding him was a problem.You have to spoon-feed him.It took us about 2 hours just to feed him with porridge.”([43];p.45)
3.2.1.3.Psychological well-being:the complexity of psychological changes.Similar to the psychological impacts on cancer patients when they were diagnosed with cancer,informal caregivers also experienced several stages,varying from being shocked to accepting cancer.In the beginning,informal caregivers were angry and refused to accept the cancer diagnosis because they had never thought about cancer before [42-46].Informal caregivers bargained with the death of cancer patients while expressing fear about the unpredictable future,including the uncertainty of cancer development and its complications[43,44,46].Furthermore,facing cancer complications suffered by cancer patients exaggerated informal caregivers’ sense of guilt and uselessness because they could do nothing or suspected that they could not provide the best care for cancer patients [41-46].Even worse,some informal caregivers were anxious about the problems caused by the death of cancer patients,for instance,raising their children alone [43-45]:
“There's uncertainty in life ….It's just that the illness and cancer itself brings around,it creates a lot of uncertainty that you weren't prepared for.”([46];p.289)
3.2.1.4.Spiritual well-being:traditional values.In terms of personal values,informal caregivers regarded caring for their loved one as their responsibility[43,45,46].Hence,informal caregivers tended to hide their negative emotions because they believed that being supportive was part of their responsibilities [44-46].In terms of traditional social values,especially in Africa,caregiving tended to be deemed the duty of married women [43].Hence,despite caregivers having some spare time,additional forms of entertainment were not acceptable for informal caregivers both personally and socially,which exaggerated their sense of depression or anxiety and eventually led to feelings of guilt [43,45]:
“There are many forms of entertainment.But now that my husband is not well,I do not have any entertainment.How can I entertain myself when my husband is not well?”([43];p.50)
3.2.2.The management strategies of informal caregivers for their role of cancer caregivers
For the management strategies of informal caregivers for their role of cancer caregivers,two analytical themes were identified,which were“self-adjustment”and“seeking for formal and informal support,”discussed below.
3.2.2.1.Self-adjustment.The analytical theme“self-adjustment”revealed the essence of how informal caregivers adjust to better transform and manage their cancer caregiving role,including three descriptive themes:(a) behavioral adjustment,(b) spiritual adjustment,and (c) lifestyle adjustment.
3.2.2.1.1.Behavioral adjustment.To keep the focus on caring,informal caregivers would act as managers to organize affairs relevant to caregiving,such as developing a detailed selfmanagement system to take the reins from professionals,which could prevent them becoming emotional [41,44].To cope with difficulties,some informal caregivers tended to initiate more conversations with cancer patients or their family members than usual,because chatting with them,particularly sharing memorable events that happened in the past,could make their relationship closer,allow informal caregivers to express their feelings,and eventually improve the QoL of informal caregivers [43-45].Conversely,some informal caregivers avoided communicating with cancer patients,especially those who were suffering from cancer pain or had a changed personality,because informal caregivers found difficulties in resolving queries and insults from cancer patients [43].Because informal caregivers put the needs of cancer patients before theirs,they did not want to share issues that might upset or worry cancer patients [41,43-46].Even if they were experiencing their own health problems,informal caregivers still did not discuss their trouble and tended to take non-prescription drugs to relieve symptoms[43]:
“Yes,I think[patient]and I tend to talk a lot more.He's not as afraid to show his emotions.He has broken down a few times,which is something he probably wouldn't do before.I think it's good ….I think we've grown closer.We certainly have appreciated how much we rely on one another,and respected the fact that we need to be there for each other.”([44];p.74)
3.2.2.1.2.Spiritual adjustment.Although it was difficult for informal caregivers to live in the world of illness,they recognized that death was inevitable and tried to adapt to it[44,46].On the one hand,some informal caregivers deliberately ignored the truth to keep faith that they could beat cancer and cancer patients would be cured;on the other hand,they were realistic and understood that cancer might not be cured [43,46].Therefore,most informal caregivers enjoyed their daily life and regarded every day as the last day living with cancer patients,which was quite different compared with their attitude before caring for cancer patients [45,46].Meanwhile,they prepared for the future to face cancer and appreciate life and people living around them more than previously[44,45].Nevertheless,a minority of informal caregivers were confused about the meaning of life or even lost their faith in God[45,46]:
“I mean I'm hoping,there's part of me that's hoping that we beat this cancer.But there's the other part that's saying I've got to be realistic as well.”([44];p.74)
3.2.2.1.3.Lifestyle adjustment.Informal caregivers reported that their eating habits changed because of the heavy financial burden of caregiving;for example,they did not purchase higher-cost fooditems because they tried to reduce unnecessary costs to ensure financial survival [42,43].Another reason for the changes in their eating habits,especially eating frequency,was lack of time because of caregiving,which also resulted in reduction of social activities[42-44,46].Limited time also altered their sleep habits,which included sleeping less to provide additional care for cancer patients or switching sleeping places to offer more convenient caregiving[42,43,46].Nevertheless,as a proportion of informal caregivers realized that taking care of themselves was the basis of good caregiving,they ensured they slept and ate well to guarantee their strength [43,44,46].Although reduction of social activities was inevitable,informal caregivers still tried to keep a balance between the physical and mental needs of cancer patients and their own[43,44,46].For instance,they planned ahead for caregiving activities,such as making medical appointments and preparing meals;by doing so,they could manage to have some free time[43,44,46].Meanwhile,informal caregivers also modified their approaches for relaxing,such as watching television with cancer patients and listening to the radio,which could not only provide relaxation but also bring them closer together [43-45]:
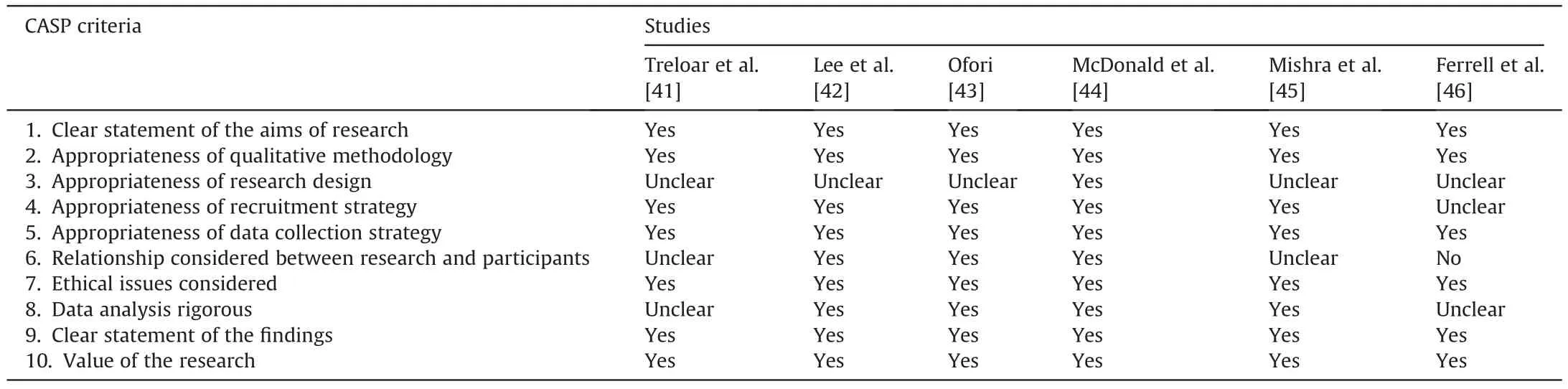
Table 3 Quality assessment of included studies.
“I have to wake up to rub his back to make him slightly more comfortable.Frankly speaking,I love to sleep but there is no other way,so I have to stay awake.”([42];p.824)
3.2.2.2.Seeking for formal and informal support.The analytical theme“seeking for formal and informal support”showed what informal caregivers seeking for supporting to help themselves transform their role of cancer caregivers and whether their needs were being met,and included four descriptive themes:(a) family and friend support,(b) religious support,(c) professional support,and (d) policy support.
3.2.2.2.1.Family and friend support.Informal caregivers highlighted the importance of family and friend support that was encouraging and could prevent their giving up [42-44].Although support might be limited because of factors beyond their control,for example,living far away from their family or limited personal financial resources,support from family and friends of cancer patients or informal caregivers was still available for daily care(including washing,feeding,and bathing),along with mental and financial support [43,44].Moreover,informal caregivers emphasized that they would feel upset and discouraged if their family members or friends neglected them and never made contributions to their daily activities [43,46].Without support from family members and friends,informal caregivers tended to disconnect from them and care for cancer patients alone,which increased their sense of isolation and led to the depression from overwork and fatigue from cancer care[43,46]:
“So actually it is a sickness that if you do not have family members around you…...It is my son that has been helping me carry him on bed and doing everything for him when he messes the bed,even food you have to feed him.That is what we are on till now.”([43];p.45)
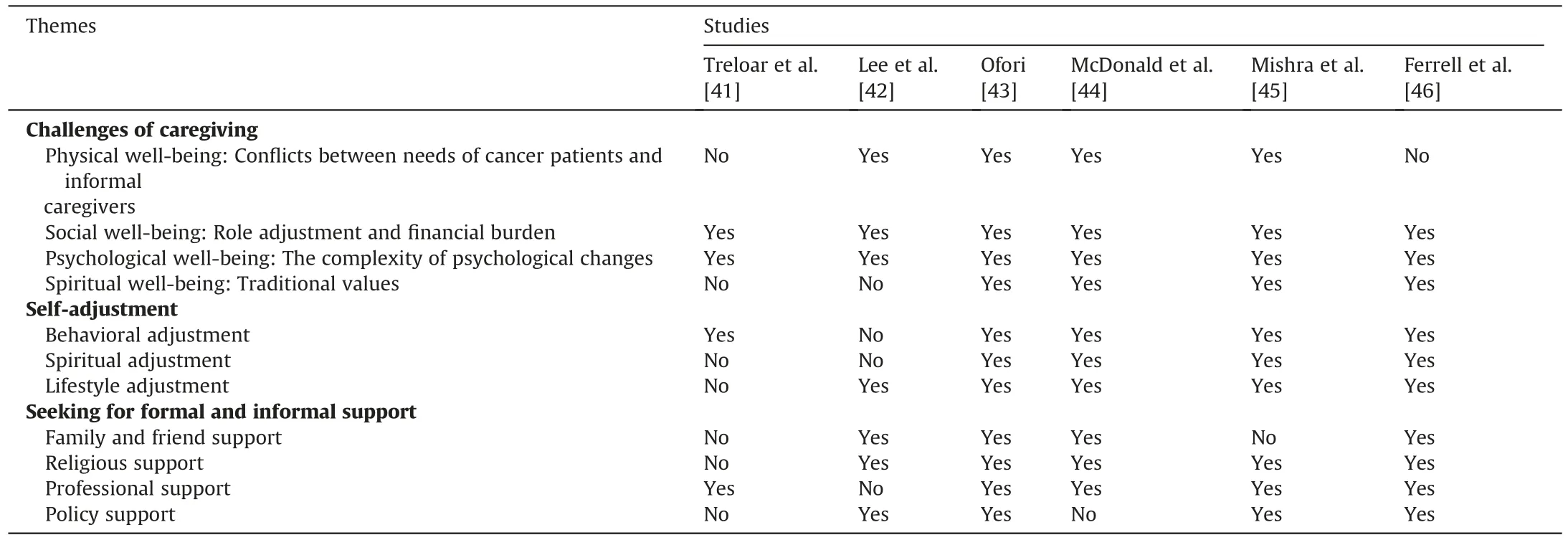
Table 4 Themes identified in included studies.
3.2.2.2.2.Religious support.Informal caregivers insisted that they could obtain strength from God,especially when they felt hopeless in fighting difficulties [42,44-46].Most informal caregivers kept the habit of praying and prayed for early recovery or remission of cancer pain of cancer patients [43,45].Even though cancer patients did not recover after praying,informal caregivers still did not give up their belief but joined another camp instead,which enabled both parties to sleep well [43].If cancer patients were so seriously ill that informal caregivers were unable to leave the patient alone,informal caregivers tended to pray or fast at home or donate money to the church instead of joining prayer camps [43]:
“…...I'm a prayer,we are always praying.[God]is the only one that can take us day by day.He is the only one that can have you go the next day.Thank Him for the day you had and you thank Him for the day He is giving you the next day.That is what will keep you going”([45];p.51)
3.2.2.2.3.Professional support.Although few informal caregivers stated that they could receive professional support,most informal caregivers complained about the lack of accessible resources (education about cancer treatments,counselling services,and services outside office hours),and expressed their expectations and desire for professional support,including support groups,home services,and online services [41,43,44,46].First,informal caregivers reported they were unaware of available services around them [41,44].Second,informal caregivers desired to learn more caregiving knowledge and skills[43,45].However,most of the time they could hardly understand the medical terms used by physicians,which confused them and eventually resulted in their low level of confidence [43-46].Third,not only guidance but also emotional or mental support should be accessible for informal caregivers,tailored to individual needs [44-46]:
“So,I don't really know whether I really need to talk to psychiatrist[…]I don't know what they…...would it be psychologist or whoever they provide just to help people get through it.I don't know what I'd say to them.‘I'm having a hard time.’ Well,isn't everybody? […]Sometimes you're just sort of reaching for something,but you don't know what.”([44];p.75)
“I haven't had anybody ask me if I needed to talk to anybody,like a caregiver support group,or an actual therapist that I could sit down and chat with and talk to that person about my issues that I can't talk to my wife about because I don't want to alarm her or concern her.”([45];p.52)
3.2.2.2.4.Policy support.Although some medical insurance covered the medical costs and some government funding was accessible for caregivers,these sources were limited [43].Those informal caregivers who obtained financial support from the government reported their concerns about the changes or sudden cutbacks in the policy,which would put them in an economic crisis[42,46].Moreover,some informal caregivers,particularly those who lived in rural areas,emphasized the insufficiency or unavailability of health insurance,which caused distress,in addition to their unstable socioeconomic circumstances [43,45]:
“Medifund(an endowment fund set up by the Government to help needy Singaporeans who are unable to pay for their medical expenses) is finishing soon.Sometimes [I]apply,[it does]not necessarily be approved.But if [I]cannot get it,it will be troublesome for [me]”([42];p.824)
4.Discussion
Based on the results of this review,cancer caregiving influences informal caregivers’ QoL significantly during the whole process of caregiving,including their physical,social,psychological,and spiritual well-being.Meanwhile,to manage the transformation to a caregiving role,informal caregivers develop diverse coping strategies to deal with the difficulties during caregiving while balancing the relationship between their own lives and caregiving.Consequently,the comprehensive assessment is crucial for informal caregivers when patients are diagnosed with cancer and a personalized support plan is necessary.
The findings indicated that informal caregivers tended to minimize their needs,particularly physiological and safety needs,if conflicts occurred between their needs and caregiving.This is because the most important needs for a particular individual might not always conform to Maslow's hierarchy of needs because of individual differences or the external environment[47,48].The needs of informal caregivers were influenced by the cancer diagnosis of patients and their traditional individual values,according to the findings.Being diagnosed with cancer is not only a huge blow to patients but also to the informal caregivers,which results in complex psychological changes in both parties.In this case,compared with before the diagnosis,the order of informal caregivers'needs is reversed and different,in addition to their individual differences,such as traditional individual values.Therefore,the comprehensive assessment of the QoL of informal caregivers and their needs is essential when they begin their caregiving role.
When placed in the caregiving role unexpectedly,informal caregivers had anxiety and depression related to the uncertainty of future cancer development and treatments,a lack of caring knowledge and skills,and the unpredictable psychological changes in cancer patients.Hence,health care professionals should provide informal caregivers with training to increase their knowledge and skills,especially knowledge related to cancer and the impact of cancer on patients.Meanwhile,because informal caregivers have to spend more time in caring,their time for such training programs is limited,and they require short-term demand-oriented training that could help them adapt to the role as soon as possible,as found in the study of Lambert and Girgis[49].To date,an increasing number of studies have explored the applicability and effectiveness of eHealth in cancer care.E-health uses the Internet or related technologies to transmit information,such as YouTube[50]and mobile apps [51],which is convenient for cancer patients and their informal caregivers to use at any time and place[52].In addition to the medical terms that are confusing to informal caregivers,eHealth provides information that could simplify complicated medical terms with the help of computer technology,such as 3D animation[53].In 2016,a meta-review synthesized evidence from 10 systematic reviews on the effects of eHealth for cancer patients and reported that eHealth could have positive impacts on their knowledge,information competence,and perceived support [54].Yet the meta-review did not find enough related reviews that investigated the influences of eHealth on cancer informal caregivers to identify its effectiveness in this situation.Although several studies aimed at testing the feasibility of eHealth interventions for informal cancer caregivers [51,55],the results are not rigorous because of the small sample size and there remains a gap for further research to fill.
Furthermore,the theme of“seeking for formal and informal support”highlighted the desire of informal caregivers for professional psychological support and the importance of family and friend support,which is consistent with the study of Cho et al.[56].Therefore,Cho et al.[56]suggested that informal caregivers and cancer patients should be treated as a“unit”because they are highly involved with each other's lives,which could fulfill informal caregivers'needs for taking control of cancer caregiving,as found in this review.Based on the findings of this review,family conversations and activities are encouraged for not only relaxing both cancer patients and informal caregivers but also to remind them of memorable events that happened in the past to draw their relationships closer and allow them to express their feelings.In other words,informal caregivers are likely to benefit more if cancer patients participate in the management of their caregiving role,which allows both parties to communicate more than usual.However,the findings also emphasized that informal caregivers believed that being supportive was their duty,and therefore they tended not to express their feelings or talk about their difficulties because it might upset the cancer patients.Consequently,it is recommended that health care professionals choose different support strategies according to the needs of informal caregivers,including discussing the difficulties and feelings encountered in the care process with the caregiver alone or with the caregiver and the patient.
Furthermore,the findings found that informal caregivers still complained and showed their worry about the lack of adequate policy support,especially the health insurance from the government.Although it is not yet clear whether adequate policy support could directly improve the QoL of informal caregivers,at the very least the improvement of policy support can reduce the burden on informal caregivers.
5.Strengths and limitations
This review was strengthened by including informal caregivers caring for cancer inpatients or outpatients in a wide age range,living with different cancer diagnoses and undergoing different cancer treatments.In addition to the large sample size and diverse relationships between cancer patients and informal caregivers,the generalized results could be applied to different countries and regions.However,the gender of informal caregivers was unbalanced because there were 77 females and only 26 males included in the review,which may overlook the QoL and experiences of informal male caregivers [57].Hence,the quotations from male caregivers are inadequate and further research is needed.Only studies published in English and Chinese were included,which may also miss studies published in other languages.
6.Conclusion
This review contributes to a better understanding of how cancer caregiving influences the QoL of informal caregivers and the management strategies of informal caregivers for their role as cancer caregivers.Ultimately,three analytical themes emerged,which were“challenges of caregiving,”“self-adjustment,”and“seeking for formal and informal support.”Based on the results,we recommend comprehensive assessment as crucial for informal caregivers when patients are diagnosed with cancer and personalized support plan is necessary,for example,a short-term demand-oriented training program and additional assessments of individual support needs.Furthermore,continued policy improvement is needed and research based on clinical practice is crucial in order to represent effective interventions to improve the QoL of informal caregivers.
Ethical approval
No ethical approval was needed in this review because this is secondary research and the quotations were retrieved from primary studies.
CRediT authorship contribution statement
Yingying Cai:Conceptualization,Methodology,Data curation,Software,Writing-Original draft.Alison Simons:Conceptualization,Methodology,Writing-Reviewing and Editing,Supervision.Samantha Toland:Conceptualization,Methodology,Writing-Reviewing and Editing,Supervision.Junfeng Zhang:Data curation,Writing-Reviewing and Editing,Software.Kexin Zheng:Data curation,Software.
Declaration of competing interest
The authors declare no conflict of interests.
Appendices.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2021.03.006.
 International Journal of Nursing Sciences2021年2期
International Journal of Nursing Sciences2021年2期
- International Journal of Nursing Sciences的其它文章
- Supplement to the published paper“Theory-guided interventions for Chinese patients to adapt to heart failure:A quasi-experimental study”
- Realities,scope,challenges,and facilitators for implementation of nurse practitioner’s role in India:A review
- Reliability and validity of the Chinese version of the Work-Family-School Role Conflicts Scale among nurses
- Reliability and validation of the Arabic version of the Conditions for Workplace Effectiveness Questionnaire-II
- Reliability and validation of the Positive Aspects of Caregiving scale among Japanese caregivers of people with dementia
- Analysis of adversity quotient of nursing students in Macao:A crosssection and correlation study