
Effect of zinc treatment on clinical outcomes in patients with liver cirrhosis: A systematic review and meta-analysis
2021-01-14 00:34:36HueyTanAdamStreeterMatthewCrampAshwinDhanda
World Journal of Hepatology 2020年7期
Huey K Tan, Adam Streeter, Matthew E Cramp, Ashwin D Dhanda
Huey K Tan, Matthew E Cramp, Ashwin D Dhanda, South West Liver Unit, University Hospitals Plymouth NHS Trust, Plymouth PL6 8DH, United Kingdom
Huey K Tan, Matthew E Cramp, Ashwin D Dhanda, Hepatology Research Group, Institute of Translational and Stratified Medicine, Faculty of Health, University of Plymouth, Plymouth PL6 8BU, United Kingdom
Adam Streeter, Medical Statistics Group, Faculty of Health, University of Plymouth, Plymouth PL6 8BU, United Kingdom
Abstract
Key words: Zinc; Cirrhosis; Mortality
INTRODUCTION
Chronic liver disease is a serious problem both in the United Kingdom and globally.Approximately 0.1% of the European population is affected by cirrhosis which account for 1.8% of all deaths corresponding to 170000 deaths per year[1].
Liver cirrhosis constitutes the third most common cause of premature death in the United Kingdom[2].The incidence of liver cirrhosis has been increasing in the United Kingdom at a faster rate than the top four most-commonly diagnosed cancers (lung, breast, bowel and prostate)[2].It is estimated that over 600000 people in the United Kingdom have serious liver disease, and 60000 of those have cirrhosis.Over 14000 people die of liver disease each year in the United Kingdom.This figure has increased by 400% since the 1970s[3].
Regardless of the underlying etiology of liver disease, malnutrition becomes a significant clinical problem as it progresses[4].Protein-calorie malnutrition is well documented and accounts for more than 60% of patients with advanced alcoholrelated cirrhosis[5].Micronutrient deficiency including trace element deficiency has also been documented, which may play a role in disease pathogenesis through regulating antioxidant, anti-inflammatory and anti-fibrotic pathways[6].
Zinc is the second most abundant trace element in the body after iron.It forms part of more than 300 enzymes in the body[7].It plays an indispensable role in cell growth, cell differentiation and human metabolism[7].Therefore, zinc deficiency can contribute to oxidative stress, growth disorder, cognitive disorder and immune dysfunction[7].Attesting to zinc’s biological importance is its known association with the activity of proteins, including the enzymes needed for the production and destruction of collagen, thus directly affecting the process of fibrosis[7].It also possesses antiinflammatory and antioxidant characteristics that may indirectly affect hepatic stellate cells[8].
The global prevalence of zinc deficiency ranges from 4% in countries rich in animal protein and up to 73% in countries with plant-based diets[8].However, up to 83% of cirrhotic patients have zinc deficiency which is associated with disease severity[8].Zinc deficiency in liver disease is multifactorial[9].Changes in carbohydrate-lipid metabolism precipitates protein calorie and micronutrient malnutrition in patients with chronic liver disease[9].Zinc is bound to albumin, alpha 2-macroglobulin and acids so the rate of zinc absorption is due largely to albumin concentrations[10].As liver disease progresses, the level of albumin decreases and this may lead to decreased absorption of zinc, resulting in progression of liver disease and an increased risk of hepatocellular carcinoma[10].Other factors that are responsible for zinc deficiency in liver cirrhosis include disturbed zinc absorption by the digestive tract as a result of the effects of cytokines, mainly interleukin-6 and endotoxins on gut blood flow[11].This changes the small bowel intestinal mucosa and decreases zinc absorption[11].Diuretic therapy also plays a factor as it increases renal zinc excretion and reduces serum albumin and the binding capacity for zinc.
Zinc supplementation has beneficial effects on antioxidant and inflammatory pathways and therefore may delay or prevent progression of cirrhosis[12,13].We performed a systematic review of the published literature to determine whether zinc supplementation was associated with improved clinical outcomes and long-term survival in patients with cirrhosis.A systematic review of the role of zinc supplementation in the management of chronic liver diseases has been recently published[14].The review evaluated its effect on response to hepatitis C virus treatment, hepatic encephalopathy and changes in biochemistry but did not assess the effect of zinc supplementation on overall long-term survival[14].
MATERIALS AND METHODS
The protocol for this systematic review was prospectively registered on the PROSPERO database (reference: CRD42018118219) including the literature search strategy.
Types of studies
We included all interventional clinical trials in humans including randomized controlled trials and open-label trials or observational cohort studies that compared zinc supplementation of at least 28 d with those of standard intervention, or placebo in patients with cirrhosis.Trials were included irrespective of publication status, year of publication or language.We excluded non-human studies and laboratory studies using non-clinical samples.
Patients
All adults (> 18 years old) with liver cirrhosis of any etiology, diagnosed using by liver histology, imaging or non-invasive methods.We excluded studies with patients under 18 years of age and with known solid organ cancer including hepatocellular carcinoma.
Intervention
Studies that compared more than 28 d of zinc supplementationviaany route (oral or parenteral) with placebo or other standard intervention for the management of patients with cirrhosis.
Outcome measures
The primary outcome was 1-year mortality.Secondary outcomes were 6-mo mortality, 2-year mortality, change in severity scores [Child Pugh/ model for end-stage liver disease (MELD) score], complication rate from cirrhosis (hepatic encephalopathy, new ascites, variceal bleed, new jaundice or hepatocellular carcinoma).Studies had to report at least one of these outcomes to be considered for inclusions in the systematic review.
Search strategy
Electronic searchesviaMEDLINE (PubMed) 1961-present, EMBASE (1974-present), the Cochrane library (Cochrane Database of Systematic reviews), Cochrane Central Register of Controlled Trials, conference abstracts from 1980 for the following annual meetings: American Gastroenterology Association, American Association for the Study of Liver Disease, European Association for the Study of the Liver, United European Gastroenterology, British Society for Gastroenterology and British Association for the Study of the Liver.
Comprehensive searches of the following biomedical electronic databases were also conducted: MEDLINE, EMBASE, PubMed and TRIPS.The search strategy included subject headings and keywords related to “alcohol”, “zinc” and “l(fā)iver”.The full search strategy is presented in Supplementary material.The references in all identified review articles and studies were also inspected to identify other trials.Two authors independently assessed the eligible studies.
Selection of studies
Titles and abstracts of studies retrieved using the search strategy were screened independently by two authors (Tan HK and Dhanda AD) to identify eligible studies.For potentially relevant articles or in cases of disagreement between the two reviewers, the full text article was obtained and inspected independently by a third reviewer.Where an eligible study failed to report data on the primary or secondary outcomes, this information was requested from the corresponding author by email.A follow-up email was sent after 2 wk if no response was obtained.
Data extraction and management
Data were extracted independently by two authors (HT and AD) using a standardized, pre-piloted form for assessment of study quality and evidence synthesis.We studied the following data: Study setting and target population, study methodology, details of intervention, primary and secondary outcomes and method of measurement and information of bias.Extracted data were discussed and this discussion was documented.
Assessment of risk of bias in included studies
Two authors independently assessed risk of bias in the trials without masking the trial names using a standard checklist.Risk of bias was assessed using the National Institutes of Health risk of bias tools for controlled trials or observational studies[15].Any discrepancies or unusual patterns were checked with an independent reviewer.
Controlled intervention studies were assessed for randomization, allocation method, blinding, and similarity of baseline characteristics, drop-out rate, protocol adherence, outcome measures and method of analysis.
Observational studies were assessed for whether there was a defined population, the participation of eligible population, appropriate outcome measures and analysis methods, loss to follow-up rates and confounding factors.
Data synthesis
We provide a narrative synthesis of the findings from the included studies, structured around the target population, timing of intervention, and type of outcome.
The survival (until death) rates from each study contributed to a meta-analysis of the efficacy of zinc supplementation in reducing mortality.If heterogeneity was deemed to be at least moderate as determined by theI2statistic exceeding 30% detected at least at the 5% level, then the data would be meta-analyzed with a random effects model, otherwise a fixed effects model would be considered, if there were too few studies to detect heterogeneity.If any subset of studies were found to share characteristics that contributed to heterogeneity across all the studies, then further meta-analyses would be conducted on those subsets.Analysis was performed using themeta package[16]with a current installation in R.
RESULTS
Study selection
Seven hundred and twelve records were identified; 49 of them were retrieved and assessed for eligibility.Six studies met selection criteria but outcome data could not be obtained from one and another was an uncontrolled cohort study.Therefore, a total of four randomized controlled trials were included in this systematic review (Figure 1)[17-20].Study characteristics are presented in Table 1.
Characteristics of included studies
All four included studies were randomized controlled trials (RCTs).All but one study documented both gender and age.None of the studies reported ethnicity of their patient cohort.All four studies selected different clinical populations includingpatients with cirrhosis with hepatic encephalopathy, decompensated hepatitis C cirrhosis, and cirrhosis with etiology not documented.All studies were conducted in community settings.The definition of cirrhosis was based on histological and biochemical confirmation in three studies; the remaining study did not specify the method of diagnosis of cirrhosis.Only one study was designed to test the effect of zinc supplementation on mortality.
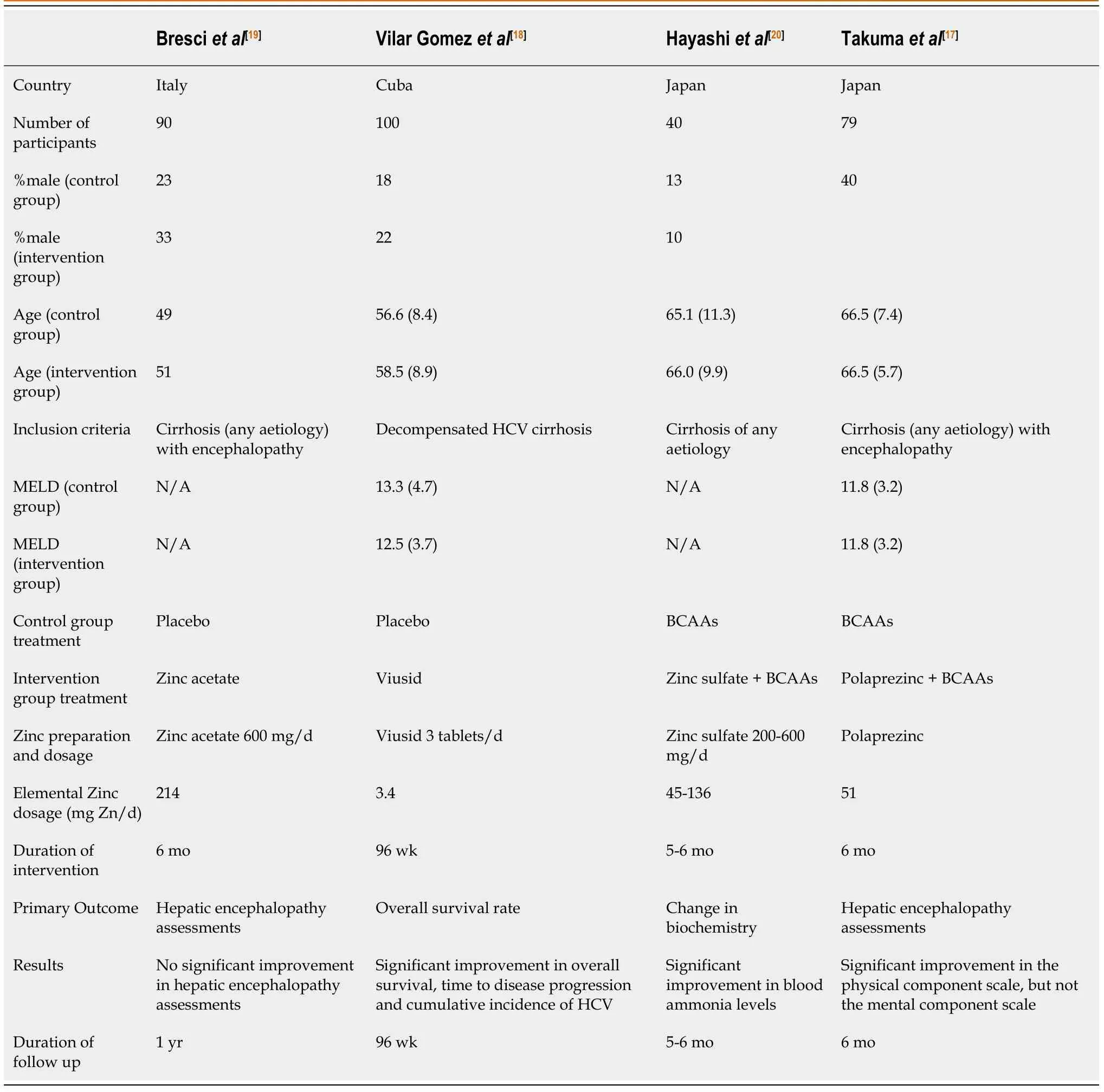
Table 1 Characteristics of studies included in systematic review, n (%)
Only two studies (Takumaet al[17]and Vilar Gomezet al[18]) reported severity of cirrhosis with mean Child Pugh scores of 6.0 and 6.3 and MELD scores of 11.8 and 12.9.
Bresciet al[19]examined the effect of long-term oral zinc supplementation on recurrent hepatic encephalopathy.Ninety cirrhotic patients with recurrent encephalopathy were treated with 600 mg of oral zinc acetate daily for 30 d in addition to standard therapy.The final values of psychometric tests were better in the zinc group compared to the standard therapy group, but the differences were not statistically significant.Three deaths were reported within 6 mo (one in the placebo and two in the intervention group).
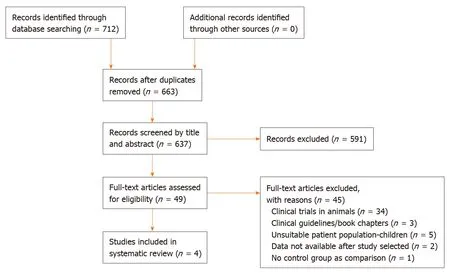
Figure 1 Flow diagram of study identification and selection.
Vilar Gomezet al[18]evaluated the efficacy of Viusid for 96 wk in reducing mortality in 100 patients with hepatitis C-related decompensated cirrhosis.Viusid was chosen because it is a nutritional supplement with recognized anti-inflammatory and antioxidant properties.It contains 11 active compounds including zinc sulphate and glycyrrhizic acid.Glycyrrhizin is the most active ingredient of Viusid and has antiinflammatory, immune-modulating and antiviral properties.The total amount of daily elemental zinc participants received was 3.4 mg, the lowest zinc content of any of the included studies.The study demonstrated a significant improvement in overall survival, time to disease progression and cumulative incidence of hepatocellular carcinoma.No differences were observed between groups for incidence of liver decompensation (including hepatic encephalopathy, spontaneous bacterial peritonitis, hepatorenal syndrome and gastrointestinal bleeding).
Hayashiet al[20]randomized 40 patients with cirrhosis to receive a combination of branched chain amino acids and zinc sulfate 600 mg daily for 6 mo.No deaths were reported during the study.They demonstrated a significant improvement in blood ammonia levels in the combination group, but there was no further investigation done to determine the mechanism of action and long-term clinical efficacy.
Takumaet al[17]investigated the effectiveness of oral polaprezinc (51 mg zinc and 174 mg of L-carnosine daily) in 79 patients with hepatic encephalopathy.They concluded that oral polaprezinc did significantly improve the physical component scale, but not the mental component scale in patients treated with zinc supplementation.One death occurred in the placebo treated arm only.This study was limited by short-term followup (6 mo) and non-blinded treatment allocation.
Survival
No studies reported 1-year mortality, which was the primary outcome of this systematic review.Three studies (Bresciet al[19], Hayashiet al[20], and Takumaet al[17]) reported 6-mo survival and one (Vilar Gomezet al[18]) reported 2-year survival.There is a substantial amount of heterogeneity across the selected study trials in terms of zinc formulation, dosage and patient characteristics.The heterogeneity includes dose quantity and frequency, formulation and types of patients.
Risk of bias assessment
We used the National Institutes of Health risk of bias tools to assess the quality of included studies[16].Two studies (Vilar Gomezet al[18]and Hayashiet al[20]) were of low risk of bias and two studies of uncertain risk of bias (Bresciet al[19]and Takumaet al[17]).Risk of bias assessments are presented in Supplementary Table 1.The two studies scored low as a result of lack of blinding and non-similarity in baseline characteristics.Three out of four studies reported information on patient characteristics.Thus, multivariate meta-regression was not appropriate.Selection bias is likely as two studies included only male subjects.Lack of information precluded a proper evaluation of all the risk of bias in the studies.
Meta-analysis
TheI2statistic measuring heterogeneity across all included RCTs was estimated to be 66% and significant at the 5% level (P= 0.03).The overall effect of zinc supplements from the included RCTs was estimated to reduce the risk of mortality by 0.98 [95% confidence interval (CI): 0.90-1.05; Figure 2].Three out of the four included studies had a 6-mo follow-up.The study by Vilar Gomezet al[18]reported the largest effect (risk ratio = 0.82), although uncertainty around the point estimate was relatively wide (95%CI: 0.68-0.99).Notably it had a longer 2-year follow-up, and so the meta-analysis was repeated without this particular study, which according to its weight, contributed the least to the overall estimated effect.The effect of all the studies measuring mortality within a 6-mo follow-up were similarly located close to, and not significantly different from, the null effect.Repeating the meta-analysis on these resulted in a risk ratio of unity (95%CI: 0.90-1.05) for the effect of zinc supplementation on the risk of mortality over a 6-mo follow-up (Figure 3).
DISCUSSION
This systematic review identified just four studies that assessed whether zinc supplementation is associated with improved clinical outcomes in patients with cirrhosis.All four eligible studies were highly heterogeneous in terms of patient characteristics, treatment formulation and duration.Four different zinc preparations, with daily elemental zinc doses ranging from 3.4 to 214 mg daily, were tested.Two of these (Viusid, polaprezinc) contained other active compounds, which could have contributed to the positive clinical outcome, for example Viusid contains only 3.4 mg of elemental zinc along with 10 other active ingredients.Three studies tested zinc supplementation in combination with other intervention (branch chain amino acids and nutritional support).
A further limitation is the low mortality rate in all eligible studies.With such a low event rate, any effect of zinc on mortality is difficult to determine.This suggests that either severity of cirrhosis was mild or follow-up duration was insufficient.Only two studies reported severity of cirrhosis with the majority of subjects classified as Child Pugh class A.Two out of four studies were designed to determine the benefit of zinc on hepatic encephalopathy and not powered to detect differences in mortality.
Both Vilar Gomezet al[18]and Takumaet al[17]suggested the most likely beneficiaries from zinc supplementation would be those with portal hypertension and leaky gut with its resultant risk of sepsis.Preclinical andin vivoevidence suggests that zinc may reduce gut permeability[21].Zinc carnosine (polaprezinc) improvedin vitrogut epithelial cell migration and proliferation[21].In healthy volunteers, zinc carnosine treatment reversed both indomethacin-induced and extreme exercise-induced gut leakiness[22].To test the benefit of a combination strategy of zinc supplementation and treatment of gut leakiness in advanced cirrhosis, long-term studies in patients with portal hypertension are required.
Given the limited data, we are unable to determine whether zinc supplementation improves survival or reduces disease severity in patients with cirrhosis.Research is still needed to confirm the preclinical benefits seen with zinc supplementation on antifibrotic, anti-inflammatory and antioxidant processes.To determine whether zinc supplementation improves clinical outcomes of patients with cirrhosis, further high quality studies are required to ascertain the optimal zinc formulation, dose, duration of treatment and patient population to treat.
In conclusion, this systematic review has highlighted the paucity of high quality studies investigating the effect of zinc supplementation in patients with cirrhosis.Eligible studies were of variable design and quality.The primary analyses all had substantial heterogeneity reflecting the differences in study design, inclusion criteria and primary outcome.The difference in etiology and severity of liver cirrhosis also make the effect of zinc supplementation difficult to interpret.With a plausible rationale for benefit from zinc supplementation, there is a strong argument to develop well designed studies in patients stratified clearly by severity of cirrhosis and presence of portal hypertension to determine the long term outcome of zinc supplementation.

Figure 2 Forest plot of all included randomized controlled trials using a random effects model.

Figure 3 Forest plot of included randomized controlled trials reporting 6 mo mortality using a random effects model (Vilar Gomez et al[18] excluded).
ARTICLE HIGHLIGHTS
Research background
Zinc is an essential trace element integral to many cellular and immune functions.Zinc deficiency is highly prevalent in patients with cirrhosis and related to disease severity.
Research motivation
Zinc supplementation has been used to treat complications of cirrhosis including hepatic encephalopathy.However, it is unknown whether zinc supplementation in patients with cirrhosis results in a change in the risk of progression of cirrhosis or death.
Research objectives
This study aimed to evaluate whether zinc supplementation improves clinical outcomes and long-term survival in patients with cirrhosis.
Research methods
A systematic review was performed including all studies in Medline, Embase or Cochrane database with inclusion criteria of adult human studies, comparing zinc supplementation of at least 28 d with standard care or placebo in patients with cirrhosis.Mortality and clinical severity score data were extracted.Random effects meta-analyses determined risk of mortality in patients receiving zinc supplementation versus comparator at 6 mo and 2 years.Risk of bias was assessed using the National Institutes of Health quality assessment tool.
Research results
Seven hundred and twelve articles were identified of which four were eligible.Zinc formulations and doses varied for different intervention periods in patients with differing etiology and severity of cirrhosis.Two studies were considered to be at high risk of bias.There was no significant difference in 6-mo mortality between patients treated with zinc versus controls.Changes in severity scores were not reported in any study.
Research conclusions
Findings are limited by the small number of eligible studies and significant heterogeneity in intervention and patient population.Zinc supplementation is not statistically associated with reduced mortality or improved long term outcome in patients with cirrhosis.
Research perspectives
There is substantial heterogeneity in study design, inclusion criteria and primary outcome.The difference in etiology and severity of liver cirrhosis also make the effect of zinc supplementation difficult to interpret.Further well-designed prospective studies are required to determine whether zinc supplementation improves long-term clinical outcome in patients with cirrhosis.
 World Journal of Hepatology2020年7期
World Journal of Hepatology2020年7期
- World Journal of Hepatology的其它文章
- Is right lobe liver graft without main right hepatic vein suitable for living donor liver transplantation?
- Diagnosis and management of hepatic artery in-stent restenosis after liver transplantation by optical coherence tomography: A case report
- Non-alcoholic steatohepatitis and the risk of myocardial infarction: A population-based national study
- Anti-inflammatory and anti-oxidant effects of aloe vera in rats with non-alcoholic steatohepatitis
- Ipragliflozin-induced improvement of liver steatosis in obese mice may involve sirtuin signaling
- Oxidative stress in alcohol-related liver disease