
Review of radiographic findings in COVID-19
2020-11-28 08:41:48AudreyKaufmanSonumNaiduSarayuRamachandranDaliaKaufmanZahiFayadVenkateshMani
World Journal of Radiology 2020年8期
Audrey E Kaufman, Sonum Naidu, Sarayu Ramachandran, Dalia S Kaufman, Zahi A Fayad, Venkatesh Mani
Abstract
Key words: Coronavirus; COVID-19; Pneumonia; Computed tomography scan; X-Ray;Pandemics
INTRODUCTION
The World Health Organization (WHO) announced a disease outbreak on January 5,2020, reporting that their China Country Office received notification on December 31,2019 of multiple cases of pneumonia of undetermined etiology in Wuhan City in Hubei Province, China. This outbreak has since ballooned into a worldwide pandemic. Patterns of radiographic findings have now been described in this illness.The intention of this study is to review published literature for the range of radiographic findings in these patients and review the overall role of imaging.
The WHO’s original report mentioned 44 cases diagnosed as of January 3, 2020 with 11 (25%) of those stricken being severely ill. Some of the patients shared a common work location at the Huanan Seafood market. The seafood market being a common link suggests the possibility of animal to human transmission. A betacoronavirus has been identified as the cause of the illness and is similar to the viruses that cause severe acute respiratory syndrome (SARS) and Middle East Respiratory Syndrome. Based upon comparative genomic analysis, this novel coronavirus likely emerged from an animal reservoir of a bat, with a Malayan pangolin potentially serving as an intermediate host.
The novel virus was officially named “Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV-2)” by the International Committee on Taxonomy of Viruses. On February 11, 2020 the WHO named the disease caused by the virus“coronavirus disease 2019 (COVID-19)”. In rapid course over the last few months, the virus has spread worldwide causing a global pandemic. As of April 18, 2020, there have been 2160207 confirmed cases and 146088 deaths reported globally. Also as of April 18, 2020, the United States has 690714 confirmed cases and 35443 deaths.
CLINICAL PICTURE
The presentation of COVID-19 is most remarkable for pulmonary symptoms that if become serious can quickly turn deadly. In a series of 41 patients, the clinical symptoms of COVID-19 commonly included fever (98%), cough (76%), and myalgia(44%). Dyspnea was present in 22 of 40 patients (55%) in the same study and became apparent a mean of 8.0 d after onset of symptoms. Respiratory symptoms progressed to acute respiratory distress syndrome (ARDS) in 29% of all cases. Another study focused on 21 moderately ill hospitalized patients who did not require oxygen therapy and found, among this group, fever (86%) and cough (57%) to be the most common presenting symptoms. According to the Centers for Disease Control and Prevention,pulmonary disease is considered severe in 14% of cases with symptoms including dyspnea, hypoxia or > 50% lung involvement on imaging and is considered critical in 5% of cases with symptoms including respiratory failure, shock or multi-organ failure. With the accumulation of data on hospitalized patients, it is now possible to examine characteristics and comorbidities related to COVID-19. A large study of 5700 patients in the New York City area showed hypertension (56.6%), obesity (41.7%) and diabetes (33.8%) to be the most common comorbidities.
PATHOLOGY
Patterns of histopathology have been described to a limited extent. According to Xubiopsy and autopsy reports are “barely accessible” in this fast-moving crisis.This group published a pathology case report of postmortem biopsy specimens from a patient that died of a severe case of COVID-19. The pulmonary specimens showed desquamated pneumocytes and hyaline membrane formation consistent with ARDS in the right lung, and pulmonary edema and hyaline membrane formation consistent with early ARDS in the left lung. Bilateral interstitial infiltrates, predominantly lymphocytic in nature, were also seen on histopathologic evaluation. Additionally,there were viral cytopathic-type changes in pneumocytes within the alveolar spaces.This single case study did not identify any viral inclusions within the pathology specimens. A more recent report of three cases where histopathology was obtained showed direct evidence on electron microscopy of viral inclusions within endothelial cells in one patient’s transplanted kidney. Using light microscopy and immunohistochemical staining, the group also found endothelial cell inflammation and apoptosis in many organs including the heart, kidney, liver and small bowel.Laboratory findings of bloodwork on COVID-19 patients generally show a picture of viral infection with low lymphocyte counts. In a study of 99 patients, most subjects had a decreased absolute value of lymphocytes in the peripheral blood. Another study of 34 patients found 50% had a decreased lymphocyte count. This finding may be secondary to the virus causing an immune response in which chemokines recruit specific immune cells such as lymphocytes to the site of infection. In addition,studies have found increased prothrombin time and D-dimer in COVID-19 patients admitted to the intensive care unit. Other laboratory findings include elevations in C-reactive protein and erythrocyte sedimentation rate.
REVIEW OF IMAGING LITERATURE
Methods
This study reviews the published literature for the range of radiographic findings evident in patients suffering from SARS-CoV-2 infection. Towards this end, we searched PubMed for the following terms on April 6, 2020 without imposing a starting date limit: “Covid”, “19”, “Radiology”, “Radiography”, “Computed Tomography(CT)”, “Imaging”, “Chest Radiographs (CXR)”, “X-Ray”, “Positron Emission Tomography (PET)”, “Ultrasound”, “Sonography”, “Magnetic Resonance Imaging”,and “Angiography”. English language, peer reviewed articles were looked at exclusively. After excluding articles that were outside the realm of investigation, a total of 133 articles were systematically reviewed to extract any radiographic data,both objective and subjective. In light of the swift development of new and increasing data, the study also included a look at preprinted manuscripts available on medRxiv.org and covered those that appeared most relevant with an indication of the unpublished status to date. The data within each article were organized in groups into the following categories: Study design (case study or series or letter.); Number of cases; Location (Country where imaged); Imaging Modality; Biological Sex; Age;COVID-19 lab diagnosis; Radiographic findings. The subtopics for radiographic findings include disease distribution, progression and focal and generalized patterns of disease.
Results
Study design was represented by 39 case reports and 78 case series reports. These were all retrospective review studies. Relevant letters to journals and review articles were also reviewed for background. The single case reports have a male:female ratio of 23:15, while the series reports have a male to female ratio of 1982:2016. The range of number of participants within each series report shows very small series of 2-10 cases being the most common (28/78) and representing over one third of these studies(35.9%). Table 1 shows the breakdown of number of participants per study.
The case distribution by country where the imaging was performed in this data set is as follows: China 99; Italy 8; United States 5; Korea 4; Taiwan 3; Germany 2; Japan 2;Singapore 2; Turkey 2; Brazil 1; Thailand 1; and Vietnam 1. The age range distribution reveals single case reports have an age range of 27-79, with a mean age of 47.1 years old (with standard deviation of 17.4), while series reports have an age range of 2 mo-95 years old. It is difficult to assess the number of laboratory proven cases in our literature review, however the vast majority of studies mention that the cases werelaboratory confirmed mostly using real-time reverse transcription polymerase chain reaction (RT-PCR) technique on samples obtainedbronchoalveolar lavage,endotracheal aspirate, nasopharyngeal swab or oropharyngeal swab.
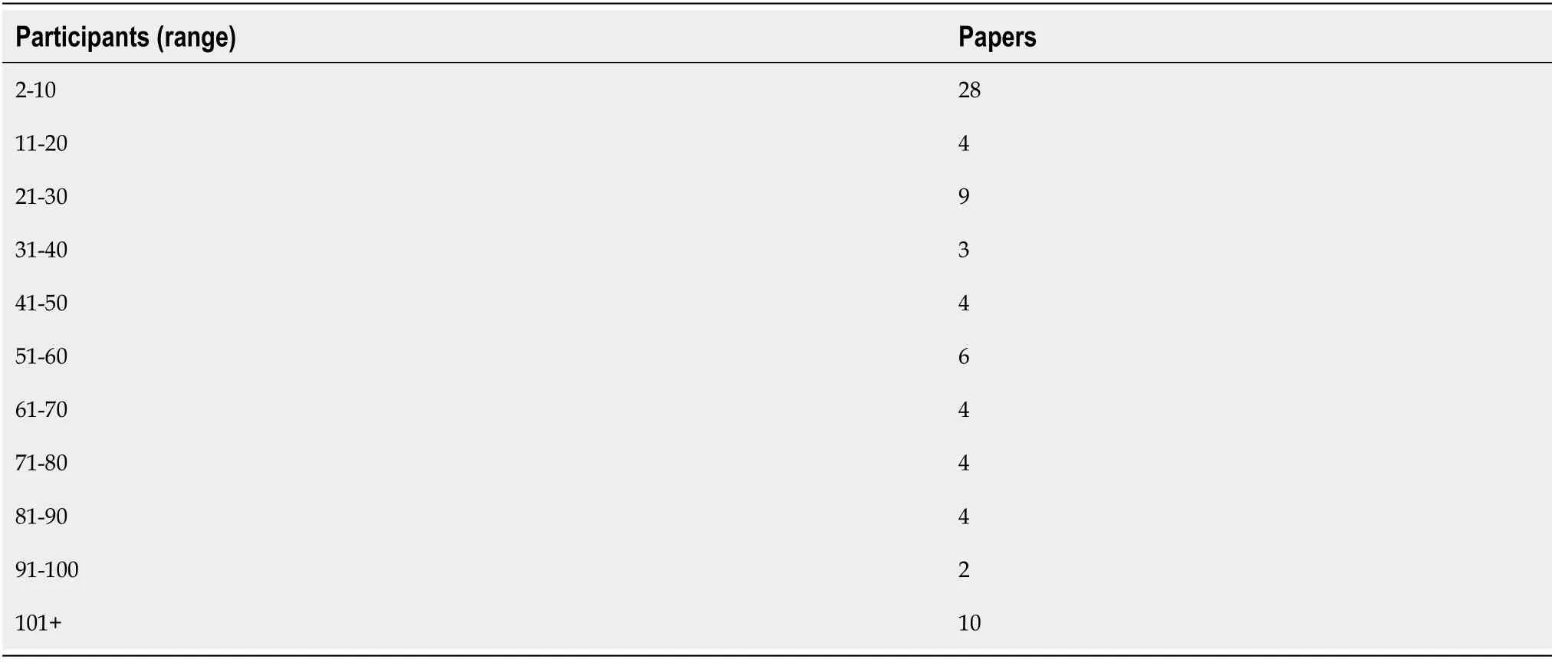
Table 1 Distribution of number of participants per study
The number of instances in which an imaging modality was utilized and focused upon in the various studies is as follows: CT 121, plain CXR 8, PET 4, and Sonography 4. Due to the significant and often fulminant pulmonary pathology present with SARSCoV-2 infection, radiographic imaging has concentrated mainly on CXR and CT. An overall review of the published data shows pulmonary findings on both CXR and chest CT with infiltrates nearly universally bilateral, peripheral and often multi-lobar with adjacent reactive pleural changes. Ground glass opacities (GGO) were frequently present either with or without concurrent consolidation, crazy paving (ground glass density superimposed with thickening of the interlobular septa and intralobular lines)and rounded morphology. Pleural effusions, lymphadenopathy and pneumothorax are seldom mentioned. Other imaging modalities noted in our review included rare mention of 18F labeled fluorodeoxyglucose positron emission tomography (F-FDGPET), sonography and magnetic resonance (MR).
CXR highlights
CXR are described in the literature but the data are relatively scant as compared to CT.In a series of two female patients, the CXR for each subject showed bilateral consolidation in the lower lung fields with follow up showing patchy consolidation.Another case study included chest radiography, the first described in Taiwan, and showed bilateral, ill-defined and patchy opacities consistent with pneumonia.Another study of 21 patients which focused on chest CT also included 5 patients with CXR. In this study the CXR failed to demonstrate early GGO in two patients and missed the peripheral nature of the infiltrates in another patient. This suggests that CXR performed early in disease course may lack the sensitivity needed to detect COVID-19 related lung disease. Such studies led to the use of chest CT to diagnose COVID-19 lung disease at earlier stages, particularly in the earlier months of the outbreak.
A larger study out of Hong Kong examines the usefulness of CXR. They studied 64 RT-PCR positive cases of COVID-19 and determined consolidation to be the most common CXR finding in 30/64 (47%). Also commonly noted were GGO 21/64 (33%),peripheral infiltrates 26/64 (41%), lower lung zone involvement 32/64 (50%) and bilaterality 32/64 (50%). Pleural effusion was uncommonly present in 2/64 (3%). They found peak severity on CXR at 10-12 d from the onset of symptoms. They concluded that CXR depicts similar findings as CT. Their study found RT-PCR to be more sensitive 58/64 (91%) to early disease than the CXR 44/64 (69%). Similarly, a recent study out of Italy retrospectively analyzed 240 RT-PCR positive cases to determine the most common lung alterations found using CXR with respect to time since symptom onset. Abnormalities most frequently occurred bilaterally and peripherally, with reticular alteration being the most common finding in early phases of the disease.GGO became predominant in later phases and consolidation, while occurring less frequently, also increased with time. CXR showed abnormalities in 75% of the RT-PCR confirmed cases. Therefore, while it has not generally been recommended due to low sensitivity, these observations confirm recent suggestions that CXR should be considered as a feasible imaging technique in diagnosing COVID pneumonia. Figure 1 depicts original CXR in laboratory positive cases of COVID-19 from our institution.
CT highlights
CT has been widely used to evaluate lung pathology associated with COVID-19.During the time period reviewed, the larger series studies in which CT was performed reveal a range of pulmonary findings. Hanin a study of 108 COVID-19 patients found 70 (65%) had infiltrates in two or more lobes with almost all the infiltrates (97%)peripherally located. When only present in a single lobe, the right lower lobe was the most common in 30/38 (79%). Overall, the findings commonly included patchy GGO(86%) and GGO with consolidation (41%), vascular thickening (80%), crazy paving(40%), air bronchograms (48%), and a halo sign (an area of GGO surrounded by consolidation, 64%). Lymph node enlargement, effusion and pleural thickening were absent.
Liuin a study of 73 COVID-19 patients grouped laboratory positive patients by disease severity in order to assess for differences in CT appearance. In mild illness(6 patients), 8% had bilateral infiltrates, 50% showed no lung changes, and 50% had an enlarged hilus and thickened lung texture. In moderate illness (43 patients), 100% of cases showed GGO bilaterally and peripherally with GGO as the single manifestation in the lungs in 12/43 (28%). Other common findings in this group were paving stone sign (35%), inter and intralobular septal thickening (27%) and air bronchogram (7%).In severe disease (21 patients), 76% had bilateral, extensive GGO, 24% had consolidation and 67% had peribronchial thickening. Critical disease (3 patients)showed confluent lesions, multi-lobe involvement, pulmonary fibrosis and white lung.Short term follow-up CT scans show dramatic improvement in 12 cases with only four patients having residual linear densities. Overall these larger studies highlight the prevalence of GGO in the lung periphery often bilaterally, that with severe disease tend to coalesce into more dense consolidation.
While the majority of the articles we reviewed were imaged in Asia, recent studies also suggest similar radiographic findings in other areas of the world. For example, in one study from Italy, GGO were the most prominent abnormality noted on CT in RTPCR positive COVID-19 patients where they were present in 58/58 (100%) of cases.Commonly noted findings in this study were: Multi-lobe involvement (93%), bilateral infiltrates (91%), consolidation (72%), crazy paving pattern (39%), rounded morphology (32%) and linear opacities (27%), while pleural effusion (3%) and cavitation (0%) were uncommonly seen. Additional interesting findings from this Italian study include perilesional sub-segmental vessels enlargement (> 3 mm, mean of 3.9 mm ± 0.6) in 89% of cases. In our review, vessel enlargement in COVID-19 was not often mentioned, but was described by Han(80%), Bai(59%), and Zhao(71%). The notable contrast in this Italian study was the presence of mediastinal lymphadenopathy that was noted in 58% of cases.
Disease progression through CT imaging is documented by Shiin a case study followed over three weeks with four CT scans. This patient was SARS-CoV-2 positive and was treated with anti-viral and anti-inflammatory medications and supportive care. On day eight from onset of symptoms, there are bilateral peripheral multifocal GGO. A day 15 scan shows mixed GGO and consolidation. A day 19 scan shows similar yet resolving findings and is followed by a day 31 scan showing complete healing. A larger series of moderately ill hospitalized patients demonstrated a peak in severity of CT findings approximately 10 d after symptom onset. Lingdescribed their experience with 295 RT-PCR positive COVID-19 cases. They found 49 cases had negative initial CT scans and 15/49 developed findings after 3-6 d,while 34/49 CT scans remained negative. They suggest that since clinical symptoms and CT findings are not always present in COVID-19 careful screening and isolation practices are critical.
Bernheimgive another perspective on disease progression by looking at CT appearance relative to duration of symptoms in their review of 121 patients from China. Bilaterality increased in incidence when patients were scanned later relative to symptom onset: Early (0-2 d, 28%), intermediate (3-5 d, 76%) and late (6-12 d, 88%).Additionally, the group found the following increasing over time: GGO and consolidation both bilaterally and peripherally, total lung involvement, linear opacities, crazy paving pattern and reverse halo sign (central ground glass density with surrounding consolidation). A rounded morphology of the infiltrates was seen in 54% of all the patients and was most prevalent in the intermediate group (67%).Figure 2 depicts original chest CT images in laboratory positive cases of SARS-CoV-2 from our institution.
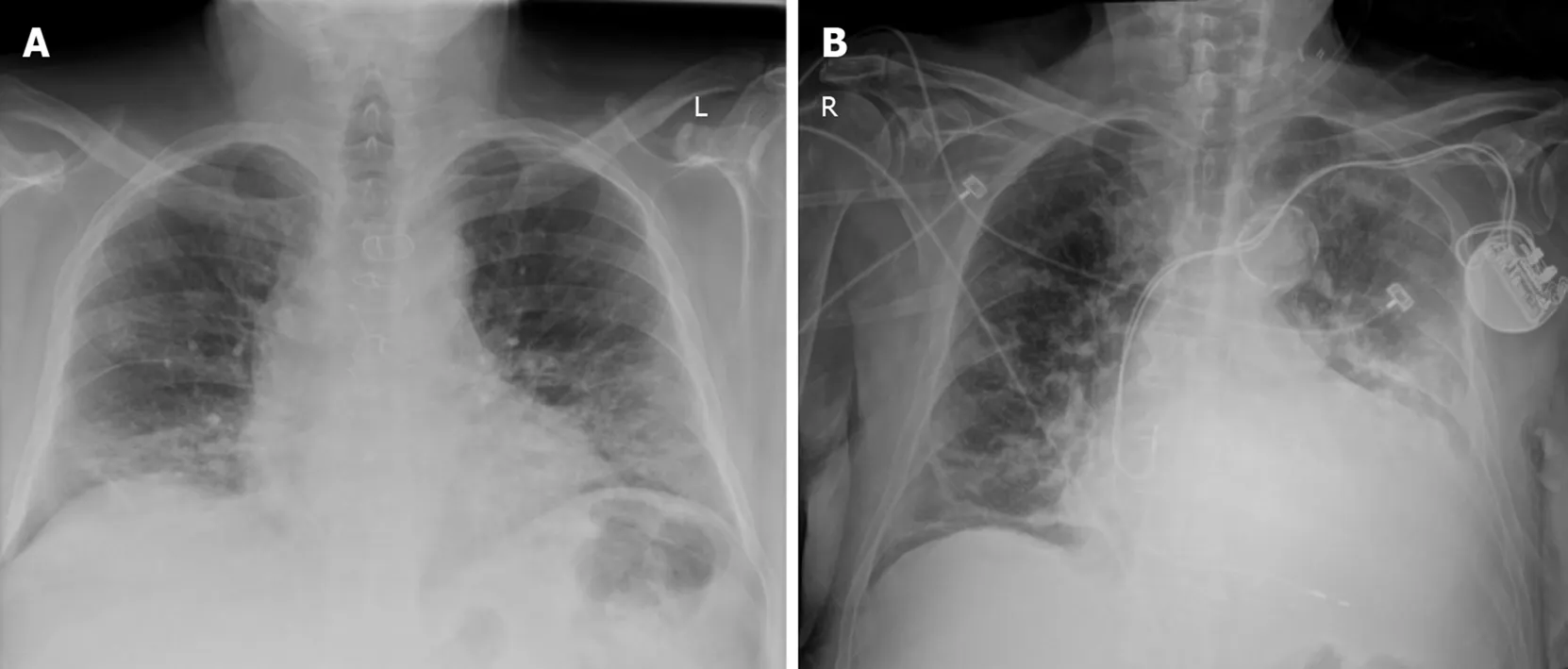
Figure 1 Anteroposterior chest radiographs in two patients with coronavirus disease 2019 pneumonia from our institution. A: Interstitial infiltrates and ill-defined, patchy, rounded peripheral opacities in bilateral lung fields; B: Interstitial infiltrates with linear and patchy, rounded opacities in bilateral lung fields and heavily calcified aortic arch.
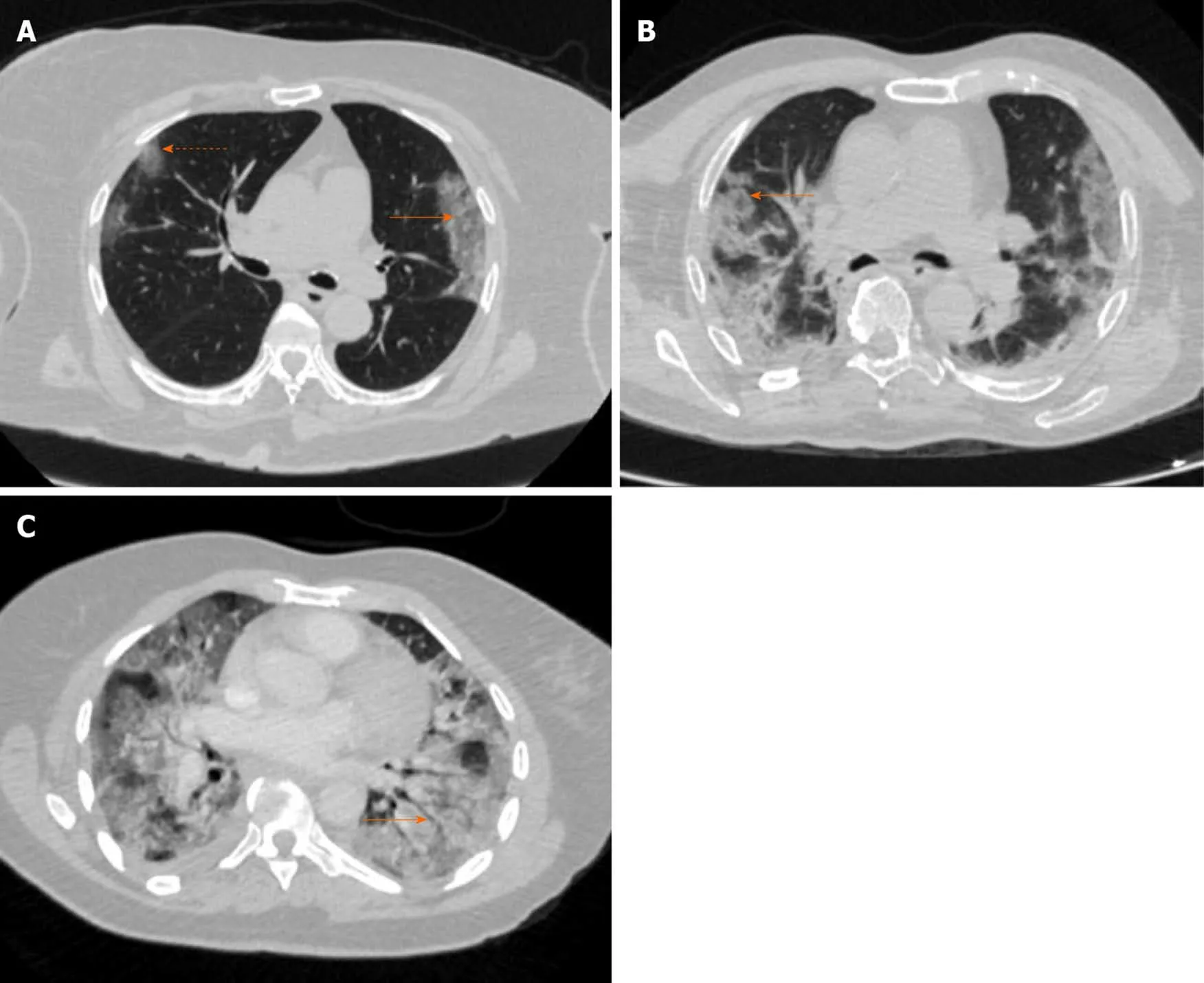
Figure 2 Axial thin-section chest computed tomography in three patients with coronavirus disease 2019 pneumonia from our institution.A: Non-contrast exam with rounded, bilateral ground glass opacities (dashed arrow) and interlobular septal thickening giving appearance of crazy paving (solid arrow); B: Non-contrast exam with rounded, bilateral ground glass opacities and areas of surrounding consolidation giving appearance of reverse halo sign (solid arrow); and C: Contrast enhanced exam with ground glass and dense consolidation bilaterally and air bronchogram (solid arrow).
Regarding distribution of pulmonary findings in COVID-19, two studies showed a predominance of multilobar involvement. Five lobes were involved in 27% of 121 cases and 44.4% of 63 cases. This is consistent with an imaging picture of viral pneumonia rather than bacterial lobar pneumonia. Regarding central versus peripheral distribution of infiltrates, Bernheim’s group found none of the 121 cases with a central peribronchovascular distribution. Conversely, peripheral pathology was present in 52% of all cases, and became more prominent as a finding later in the disease course (64% in intermediate time-point scans, 72% in late scans).
Specific populations
A few studies evaluated COVID-19 in a pediatric population. In a series of five confirmed positive cases of (age range of 10 mo – 6 years), three pediatric patients had modest patchy GGO. The other two cases showed normal findings on CT, and none of these patients had CXR. Another group that evaluated 4 pediatric cases found the CT scans to be nonspecific and mild. These small samples suggest milder disease in a pediatric population.
A more recent study includes radiographic findings from nine COVID-19 infected pediatric patients. Compared to adults, these patients also presented with less severe symptoms. Ground glass opacities, patchy, high-density shadows, and parenchymal bands were the most common CT findings, however, some of these infected pediatric patients showed no abnormal CT features.
A few investigations looked at COVID-19 in pregnancy. One study followed 15 confirmed COVID-19 positive pregnant women ranging from gestational week 12-38. CT findings were reported to be similar to non-pregnant patients with GGO early in the time course, and further consolidation and crazy paving pattern with progression. Delivery itself did not exacerbate the pneumonia in 10 cesarean sections and one vaginal delivery. Additionally, this group found no infections in the neonates(= 11). Another study of COVID-19 positive patients (41 pregnant; 14 non-pregnant)examined pulmonary findings on CT and showed that consolidation was statistically more common in pregnant patients than non-pregnant patients, and conversely, GGO with reticulation was significantly less common in pregnant patients than nonpregnant patients. These differences may relate to the physiological and anatomic changes of pregnancy.
Other modalities highlights
Although CT and CXR predominate the imaging landscape in COVID-19, there are a few studies of other modalities. Qinstudied 4 presumptively positive cases of COVID-19 that underwentF-FDG PET/CT. According to the group, the nuclear scans were performed before the infectivity of the virus was apparent and this was the first PET study on presumptive positive patients in Wuhan, China. They found uptake in ground glass and/or consolidated opacities peripherally located in more than two lobes of the lung. Of note, they found no disseminated lesions suggesting tropism of the disease for the lungs. Also, in three of four cases, they foundF-FDG uptake in nearby (hilar, mediastinal and subclavian) non-enlarged lymph nodes suggesting lymphadenitis. There was also a single case report in the literature ofF-FDG PET/CT imaging in a COVID-19 confirmed positive case that shows avid uptake of the tracer in areas of consolidation bilaterally and uptake in hilar and mediastinal lymph nodes as well. The risk to perform nuclear scans in COVID-19 patients is noted, as the high infectivity of the virus and the extended length of time the patient stays in the radiology suite for PET imaging is much lengthier than most other tests.
There is a published case report and a 20 case series report describing the use of sonography in COVID-19, in a point-of-care setting. The lung sonograms were performed using a portable device at the bedside and in both studies demonstrated evidence of irregular pleural lines, sub-pleural consolidation, areas of white thick lungs and thick irregular vertical artifacts suggesting interstitial-alveolar damage. The authors highlight the advantage of reducing infectious exposure to other patients and healthcare workers by performing the study at the bedside. In addition, they believe it to be easily repeatable and widely available particularly in a low resource setting.
A more recently published paper by Soldatiis a proposed guide to standardize the performance of lung ultrasound exams in patients with COVID-19.The proposal covers acquisition protocol, reviews anatomical landmarks, highlights salient findings and proposes a scoring mechanism. The group presents an important point that because sonography is more portable and available in a wider range of settings throughout the world, as compared to other imaging modalities, it is more accessible to low and middle income countries and will, thus, improve the disparity often present in trials with imaging endpoints. Regarding specificity of lung ultrasound, a separate study showed that in the not-very-early stages of COVID-19,lung ultrasound can provide relative disease specificity when bilateral and patchy artifactual findings and signs of multifocal white lung are present. In addition, there is a more recently published study of lung ultrasound (LUS) in a pediatric population with confirmed COVID-19. This was an observational study of 10 consecutive symptomatic pediatric patients admitted to two tertiary medical centers in Rome. In these cases, LUS was performed using the Soldatiacquisition protocol referenced above. A LUS was performeda portable device at the bedside while awaiting RT-PCR results. Abnormal LUS findings were noted in every case. Vertical artifacts (70%) and pleural irregularities (60%) were the most common abnormalities detected. Pleural effusions were notably absent in all 10 patients. The group argues LUS has a distinct advantage in following COVID-19 in children because it does not use ionizing radiation.
A panel of international experts in sonography reviewed its use in COVID-19 and cover a multitude of important topics. They discuss the need to establish appropriate use of sonography by thoroughly evaluating both the sensitivity of the technique in varying degrees of COVID-19 lung involvement and the positive and negative predictive values under varied conditions. The group highlights the potential benefits of sonography to evaluate for the following: Progression of pulmonary involvement,post-procedure changes, presence of pneumothorax, ventricular function, fluid status and presence and drainage of pleural effusions. The challenges of using sonography are described and include prolonged exposure to the operator, the need for scanner boards and transducers that can be disinfected thoroughly and the corollary of the need for scanner covers that protect the machine itself without overheating it.
There is a report of MR being used to evaluate a single SARS-CoV-2 patient showing mild pulmonary symptoms but with a severe progressive encephalopathy.A gadolinium enhanced MR scan of the brain was performed but revealed no pathology. A more recent case report compares lung findings in a chest CT to those found in a cardiac MR performed two days later to rule out myocarditis. The blackblood single shot fast spin echo sequence showed pulmonary infiltrates and consolidation closely matching those in the CT.
As emphasized by the overwhelming dominance of pulmonary symptoms and the PET/CT finding of tropism for the lungs, it is not surprising that there is little written regarding radiographic findings in other organs systems. The literature review revealed cardiac injury, defined by elevation in serum cardiac biomarkers, is common among patients hospitalized with COVID-19. In a study from Wuhan, China of 416 consecutive hospitalized patients, cardiac injury was found in 82 (19.7%) cases and was statistically associated with older age, comorbidities such as hypertension, a tendency to require mechanical ventilation and higher in-hospital mortality. This same study mentioned renal injury in 8/416 (1.9%) and coagulopathy in 12/416 (2.9%).Another study in preprint found acute myocardial injury in 6/53 (11.3%) cases.Neurologic issues have also been reported in the literature. In a different study from Wuhan, China, neurologic manifestations were found in 78 of 214 (36.4%) consecutive hospitalized patients. Symptoms included headache, loss of taste or smell, dizziness,impaired consciousness, myopathy and stroke. Gastrointestinal symptoms associated with COVID-19 have been described as well. For example, one study found 5 of 34(14.7%) patients complained of diarrhea upon hospital admission.
ROLE OF THE RADIOLOGIST
The use of imaging in COVID-19 is debated within the radiology community. Many of the major radiology professional societies have recently come out with statements on this subject. The American College of Radiology states: Viral testing is the only specific method of diagnosis as recommended by the Centers for Disease Control; generally,chest imaging findings are not specific; and chest CT is considered “Usually Not Appropriate” in standard acute respiratory illness. Because of these considerations,joined with additional complex issues relating to infection control, the American College of Radiology says performing CT is not advised for screening for COVID-19 infection. They advise radiologists to become acquainted with the CT appearance of the disease so it can be recognized in patients imaged for a concurrent medical issue.Similarly, the Society for Cardiovascular Magnetic Resonance states cardiovascular MR should not be performed in COVID-19 patients unless absolutely clinically necessary. Our medical center follows these guidelines and reserves advanced imaging for when it is critical to clinical care, rather than using it as a first-line diagnostic tool in COVID-19 patients.
To understand the debate it is important to know that the current diagnostic gold standard for SARS-CoV-2 infection is laboratory RT-PCR testing to identify viral ribonucleic acid from the aforementioned biological samples. This process, in many settings, takes significantly longer than performing a CT scan and has been shown to have a lower sensitivity (60%) than chest CT (97%). Similarly, another group showed a lower sensitivity of RT-PCR (71%) as compared to chest CT (98%). Thus, diagnostic testingchest CT was recommended in various studies and has been used clinically,mostly outside the United States. For example, an Italian preprint study supports using chest CT because it is known as the gold standard for interstitial pneumonia.They found CT to have a sensitivity of 95.48%. The group also points out that diagnostic accuracy is influenced by the prevalence of the disease, and thus, during a pandemic the predictive value gives a more precise measure of CT reliability. Their study showed a high negative predictive value of > 90% and positive predictive value of 69%-84%. Therefore, they argue CT is fast, reliable and good for first-line triage where the virus is widespread.
In a region of Japan with lower disease incidence, Himotostudied the diagnostic performance of typical CT features of COVID-19 when imaged more than three days following symptom onset. The group concluded CT has an important supplemental role in identifying COVID-19 pneumonia and differentiating it from other forms of pneumonia, which can be clinically useful while awaiting the RT-PCR results. Specifically, of the 21 patients they studied, six were RT-PCR positive for COVID-19 and 15 suffered from pneumonia of other origin. Of the six positive cases,100% showed GGO with or without consolidation bilaterally with peripheral predominance. Rounded morphology and a higher number of lobes affected were significantly higher in COVID-19 infection as compared to other pneumoniae. Their radiologists showed high sensitivity (100% and 83%) in detecting COVID-19 pneumonia. They found the highest specificity (93% and 80%) when using criteria of bilateral GGO, peripheral predominance and absence of any airway abnormalities,nodules, mediastinal adenopathy and pleural effusion.
Dangisin a report in press, found low-dose submillisievert chest CT to show a high degree of sensitivity, specificity, positive predictive value, negative predictive value and accuracy overall (86,7%, 93.6%, 91.1%, 90.3%, and 90.2%, respectively) and after 48 h of symptoms (95.6%, 93.2%, 91.5%, 96.5%, and 94.4%, respectively). They also relay the advantage of finding concurrent bacterial pneumonia in COVID-19 true positive cases (7 of 72 cases, 9.7%) and finding alternative diagnoses in true negative cases (18 of 102 cases, 17.6%). As described early on in this crisis by Kim, the role of the radiologist includes detecting lung abnormalities at the earliest time point in the disease course, gauging the severity and progress of disease, and identifying radiographic findings that suggest concomitant bacterial co-infections. Overall, in the current state of affairs when testing is readily and quickly available, CT is reserved for complicated cases and to rule out concomitant pathology. Alternatively, where RTPCR testing is slower, CT imaging can be used to characterize and diagnose COVID-19 pneumonia.
The American College of Radiology emphasizes in boldface type on their website,“... knowledge of this new condition is rapidly evolving, and not all of the published and publicly available information is complete or up-to-date”. The medical community needs to be circumspect in decision-making based upon the available literature. In a recent report by Wynantsa critical assessment is made of published and preprint reports of prediction models of COVID-19 disease. The group found all 31 of the analyzed prediction models to have a high risk of bias relating to a multitude of reasons including using non-representative controls, excluding cases that had not experienced the target event by the end of the study and performing inadequate statistical analyses. They recommend that the medical community proceed with caution in using the prediction models available. Clinical radiologists should stay abreast of updated professional guidelines and, as always, read current literature with a critical eye. During a pandemic, there is value in reading review articles, such as Sunto remain aware of accepted science in the field.
Recent additions from professional societies include comprehensive consensus statements that provide critically important guidance to radiologists. A notable example was released by the Canadian Society of Thoracic Radiology in conjunction with the Canadian Association of Radiologists covering thoracic imaging in suspected and confirmed COVID-19 cases. As this particular consensus statement covers a multitude of key practical issues, clinical radiologists should be familiar with its contents and refer to it as needed.
Considering the contagion, the world faces, caution has clear benefits. Imaging at point-of-care is safer. However, if thoughtful and viable institutional policies are in place to create a decontaminated and safe radiology suite, then advanced imaging should be instituted to better understand the manifestation and progression of this deadly disease. The risk of being too prudent in investigating COVID-19 is that the medical community does not know enough and needs to know more. SARS-CoV-2 infections could spread further and wider over time before we fully understand its mechanism of action. Clearly, we need to be vigilant about safety, but we need to be equally vigilant about elucidating the pathology at hand. Collecting robust dataadvanced imaging in a safe environment should also be a priority.
For radiologists, another pertinent issue is overall quality in reported findings. In a recent article, Salehisystematically reviewed 37 published studies on diagnostic findings in CT of the chest in COVID-19 disease. They found wide variability in the terminology used in imaging reporting which can lead to confusion for healthcare providers. This is the first proposal of a reporting and data system for COVID-19. The group proposed a comprehensive lexicon to be used for typical and atypical findings in CT of COVID-19 patients with a grading system corresponding to the suspicion for lung involvement. Radiology practices should strongly consider implementing a structured reporting system for consistency and optimization in quality of patient care.
As more is learned about COVID-19, there likely will be an expanded role for imaging and radiology research. For example, mentioned above in relatively few publications was enlargement of pulmonary vessels. This finding potentially could have been present in other studies but was perhaps missed because vascular enlargement is most commonly measured subjectively in clinical radiology. As was noted in laboratory findings, these patients can have increased prothrombin time and D-dimer levels suggesting a hypercoagulable state. Thus, CT angiography may become more prominent in evaluation of thromboembolic complications. Qanadli and Rotzingerpromote this idea as they write in support of structured CT reporting for COVID-19, while strongly advocating for the inclusion of vascular abnormalities therein. Objective analysis of pulmonary segmental and sub-segmental arterial branches on CT could also prove to be an interesting way to evaluate COVID-19 perfusion abnormalities. Dual energy CT, not regularly used in the clinical domain for this purpose, could be researched to measure lung perfusion in COVID-19 patients.
Other imaging modalities may also have a larger role in future investigations of COVID-19. With a better understanding of the pathophysiology of SARS-CoV-2 infection, PET-CT has the potential to delineate involvement of the hematopoietic and other organ systems using 18F-FDG and other, novel radiotracers. MR will be useful to better define cardiovascular, neurologic, gastrointestinal and renal sequelae.Sonography will likewise be useful in characterizing sequelae in multiple organ systems.
ROLE OF ARTIFICIAL INTELLIGENCE
An entirely different angle of research involves combining imaging with artificial intelligence (AI). AI is often cited as an important method to compile large volumes of data to assist health experts. The SARS-CoV-2 pandemic has overwhelmed health care systems. Putting AI to work as intelligence augmentation needs to be a priority in order to assist physicians and public health experts during this and future crises. For radiologists the overarching goal of AI is to read imaging studies expeditiously and accurately, preferably in a triaged fashion. Augmented intelligence can integrate data from disparate sources to develop predictive models in diagnostics. By integrating imaging data, radiology reports and clinical information, AI will be a powerful tool for rapidly cataloguing information to assist radiologists and clinicians to best care for patients.
As described by Rijn, following an initial time investment by a radiologist to train a deep learning system, tasks such as image segmentation can be performed with speed and accuracy. Articles in preprint archives describe training and testing of convolutional neural networks on CXR. Deep learning algorithms based upon 2D and 3D learning models on non-contrast chest CT are being developed to aid in detection, quantification and analysis of progression in COVID-19 and are also found in print and in preprint repositories. An additional recent CT study tested an AI model that combines CT image data with multiple clinical factors and performed well compared to an experienced thoracic radiologist. A final and important addition to the conversation is the potential for AI-derived radiographic imaging biomarkers to enhance predictive population health. Utilizing AI in this manner could literally change the course of a multitude of diseases, including the current pandemic.
STUDY LIMITATIONS
This review study has some limitations. First, the majority of studies reviewed have a small number of subjects. Of our 117 case and series studies combined, 67 (57.3%) of these had 1-10 subjects with more than half of these, 39 in total, being single case studies. The lack of many larger series studies represents the novelty of COVID-19 and over time larger studies will surface in the literature. Another limitation is the possibility that some cases and series reports are represented more than once within the dataset. Also, this review did not attempt to identify image acquisition parameters or image quality. Finally, these early case and series reports are chiefly representative of hospitalized patients. Therefore, they do not represent the community-based experience of COVID-19.
CONCLUSION
The radiology literature reveals general hallmarks of SARS-CoV-2 infections. These include CXR findings of bilateral pulmonary infiltrates with a tendency toward the lung periphery and chest CT findings of bilateral and peripheral ground glass and consolidated opacities, with an absence of concomitant pulmonary nodules, cavitation,adenopathy and pleural effusions. Data from more recently affected countries are now emerging. The cutoff for this study was April 6, 2020 – since then, multiple studies have been published with results that mirror those discussed in this review.Radiologists will need to follow accumulating published data of radiographic findings in COVID-19 to confirm and reassess these earliest reported studies and to continue to address best radiographic practices.
 World Journal of Radiology2020年8期
World Journal of Radiology2020年8期
- World Journal of Radiology的其它文章
- Quantification of uric acid in vasculature of patients with gout using dual-energy computed tomography
- Sonographic evaluation of prostatic artery embolization: Far beyond size measurements
- Role for contrast-enhanced ultrasound in assessing complications after kidney transplant