
Upper body peripherally inserted central catheter in pediatric single ventricle patients
2020-11-25 12:51:50SantoshKaipaChristopherMastropietroHamzaBhaiRiadLutfiMatthewFriedmanMouhammadYabrodi
World Journal of Cardiology 2020年10期
Santosh Kaipa, Christopher W Mastropietro, Hamza Bhai, Riad Lutfi, Matthew L Friedman, Mouhammad Yabrodi
Abstract
Key Words:Thrombosis;Central venous catheters;Catheterization peripheral;Univentricular heart;Children
INTRODUCTION
Children with critical congenital heart disease (CHD) often require a central venous catheter (CVC) in the medication administration, fluid resuscitation, nutrition and hemodynamic monitoring prior to surgical repair and for post-operative care management.A subset of children with CHD can require central venous access for a longer period of time[1,2].The use of central venous catheters (CVCs) or percutaneously inserted central catheters (PICCs) for prolonged periods can result in complications including venous stenosis and thrombosis, especially in neonates[3,4].Central venous thrombosis is a cause of considerable morbidity and mortality in children who undergo surgery for CHD[5,6].Patients who undergo surgery for CHD are at high risk of developing thrombosis due to a hypercoagulable state often related to cardiopulmonary bypass and blood product transfusions[1,7,8].
There are several options for CVCs location including umbilical in neonates,femoral, internal jugular, or subclavian vein, transthoracic intracardiac catheters, and PICCs[9].Considerable variation exists between centers in the most commonly used catheters and sites, and no formal recommendations have been published to guide current practice[9-11].
Infants with single ventricle physiology need to have patent superior vena cava and upper-extremity veins to ensure adequate passive pulmonary blood flow[12].Stenosis or thrombosis of these central veins can delay surgery and, in some patients, preclude further palliation surgeries.Due to these concerns about obstruction of upper extremity veins many institutions discourage the use of upper extremity CVCs or PICCs in this patient population.However, data on the rate of venous thrombosis in children with single ventricle physiology in whupper extremity CVCs are placed are limited[8,13,14].In our practice, the use of upper extremity PICCs in this patient population is common.
We aim to describe our use of upper extremity PICCs in children with single ventricle physiology who have undergone superior cavopulmonary anastomosis as their stage two palliation surgery.
MATERIALS AND METHODS
Patients
This study was approved by the Institutional Review Board at our institution.This is a retrospective cohort study of pediatric patients undergoing cardiac surgery at our institution over a 5-year period–January 2014 to December 2018.Patients who underwent superior cavopulmonary anastomoses (Hemi-Fontan or bidirectional Glenn procedure) were identified from our institutional pediatric cardiac surgical database and data was extracted from chart reviews of the electronic medical records.Patients who required cervical extracorporeal membrane oxygenation support at any point prior to their superior cavopulmonary anastomosis procedure and patients who did not undergo a first stage palliation procedure were excluded from the study.
Institutional protocols
All patients at our institution undergo diagnostic cardiac catheterization prior their superior cavopulmonary anastomosis for surgical planning purposes.Routine screening for the presence of CVC- or PICC-associated thromboses however is not performed, studies are ordered based on the discretion of the primary care team.All patients had a diagnostic cardiac catheterization to assess hemodynamics prior to the second stage pallation surgery.
Location and type of central venous access is not protocolized.For most patients, an umbilical venous catheter is placed in neonates with CHD at birth.If a patient continues to need stable intravenous access beyond 48 h of life, a PICC is placed in the intervention radiology suite and the umbilical venous catheter removed.Intraoperatively, most patients receive a double lumen intra-cardiac, right atrial catheter is placed.For some patients, an internal jugular or subclavian CVC is placed as an additional venous access site.The ongoing need for a central venous access is assessed daily during the multidisciplinary morning rounds.For patients who are deemed to require central venous access for a prolonged period to time postoperatively, which includes most of the patients with single ventricle physiology who undergo stage 1 palliation procedures, a PICC is placed and right atrial catheters and other CVCs are removed.A heparin infusion (2 U/mL) is administered as a carrier fluid for all central venous access lumens while they are in place.
Beginning in January 2016, central venous catheter-related thrombus prophylaxis protocol in our cardiac intensive care unit was implemented.For patients who were deemed to require their central venous access for 72 h or more, low molecular-weight heparin (LMWH) is started within 48 h post-operatively or within 12 h after the placement of central venous access for non-surgical patients.The dose is adjusted by a designated clinical pharmacist based on Anti-Xa activity (goal range:0.25-0.49 IU/mL).Prophylactic LMWH protocol is delayed in for significant post-operative bleeding, concern for high risk of bleeding, use of another agent for therapeutic anticoagulation, compromised renal function (creatinine clearance <30 mL/min/1.73 m2), or concern for heparin-induced thrombocytopenia.LMWH is initiated at 0.75 mg/kg/dose every 12 h for patients who were less than 2 mo old and 0.5 mg/kg/dose for patients who were greater than 2 mo old.
Data collection
Patient characteristics including demographic data, diagnoses, and first stage palliation procedures were collected.Data regarding type and duration of the central venous access, number of catheters, and use of anticoagulation after the cardiac surgery were also collected.We also collected information regarding central venous access utilized during any hospital admissions during the inter-stage period between stage 1 palliation procedures and superior cavopulmonary anastomosis.Outcome data regarding thrombosis was collected from vascular ultrasound, computerized tomography, fluoroscopy, echocardiogram and cardiac catheterization studies obtained prior to superior cavopulmonary anastomosis.
Statistical analysis
Data are presented using descriptive statistics.Categorical data are presented as frequency with percentage and continuous variables are presented as median with(25%, 75%) unless otherwise noted.Chi square test was used to compare the rate of complications between the group of patients with PICCs and CVCs.
RESULTS
We reviewed 76 patients who underwent cardiac catheterization prior undergoing superior cavopulmonary anastomoses as their stage 2 palliation procedure (hemi-Fontan or bidirectional Glenn).Patient characteristics are shown in (Table 1).The median age at first stage palliation surgery was 9 d (25%, 75%:6, 15).Thirty (39%)patients were female and 35 (46%) patients had hypoplastic left heart syndrome.The distribution of the primary cardiac defects is shown in (Figure 1).
All patients had at least one CVC or PICC placed prior to their second stage procedure.The types of CVCs and PICCs used are summarized in (Figure 2).Fifty-six patients (73%) had an upper extremity PICC at some point prior to their superior cavopulmonary anastomosis with a median duration of 24 d (25%, 75%:12, 39).Seventeen patients who had PICCs also had an upper extremity CVC (internal jugular or subclavian vein) in place at some point prior to superior cavopulmonary anastomosis with a median duration 10 d (25%, 75%:8, 14).No patient had an upper extremity PICC and CVC in place simultaneously.Sixty-eight patients (89%) received aspirin and 68 patients (89%) received LMWH prophylaxis while PICCs or CVCs were in place.
Venous thrombus was identified in 5 patients (7%), all of which were seen on upper extremity vascular ultrasound.Three patients had hypoplastic left heart syndrome and underwent the Norwood operation, one patient had tricuspid atresia and underwent pulmonary artery band placement, and one patient had double outlet right ventricle and underwent pulmonary artery band placement.No thrombi were detectedviaother radiologic studies or cardiac catheterization.In total, upper extremity ultrasounds were obtained in 11 (14%) patients due to suspicion for thrombus.Thrombus was detected in association with 2 of the 56 PICCs (43.6%) and 3 of the 17 CVCs (18%) and the incidence of thrombosis was significantly different between the PICCsvsCVCs (P<0.04).Thrombosis was identified at a median of 5 d (Range:4-18 after their first stage palliation surgery and a median of 9 d (Range:7-16) after placement of PICC or CVC.All 5 patients were switched from prophylactic LMWH dose to therapeutic LMWH after identification of thrombosis and subsequent cardiac catheterization demonstrated thrombus resolution in 3 of 5 patients.The presence of thrombosis in two patients delayed their surgery and, in one patient, precluded the patient from having the second stage surgery.These two patients had PICCs and chorionic villi sampling prior the cardiac catheterization.None of the other 71 patients were found to have thrombosis on cardiac catheterization.Characteristics of the patients with upper extremity thrombus are shown in (Table 2).
DISCUSSION
At our institute, we utilize upper extremity PICCs in most of our single ventricle physiology patients.This cohort demonstrates that the practice of using upper body PICC lines has a low rate of thrombosis among single ventricle physiology patients.There is a large range of reported incidence of venous thrombosis after cardiac surgery in the literature.A prior study from our institute identified a rate of thrombosis of 6%among all patients who underwent cardiac surgery which similar is to this cohort[1].Manlhiotet al[2], reported thrombosis in 11% of pediatric patients with CHD[2].In another case series with 89 umbilical venous catheters and femoral central venous catheters, the incidence of the thrombosis among single ventricle patient was high as 42%[15].In a third study, Milleret al[4]reported no cases of thrombosis in 156 right internal jugular vein catheters in patients who underwent Glenn or Fontan operations[4].
Upper body venous thrombosis is a major concern for single ventricle patients because it could preclude them from further palliative operations in the future.It is important to weigh the risks versus the benefits when deciding the location and type of central venous catheter.In general, pediatric patients will require a deep sedation or mechanical ventilation during central venous catheter replacement.In our institute,PICCs are placed in interventional radiology suite, if a patient’s condition allows for a transfer.Patients receive local anesthetic and minimum sedation for placement with a high success rate.
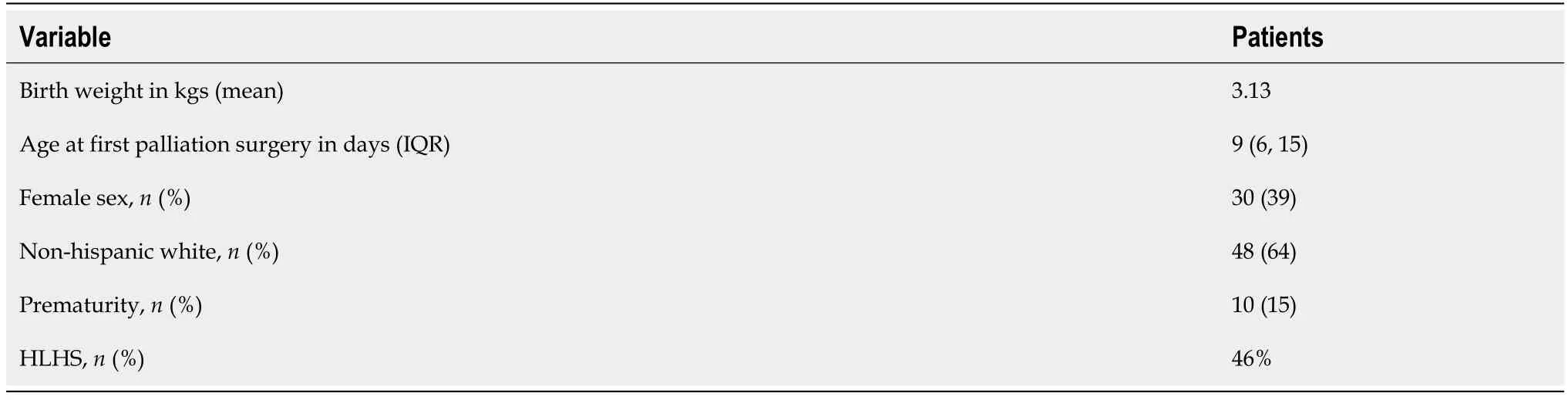
Table 1 Characteristics of the patients in the cohort

Table 2 Haracteristics of the five patients with upper extremity thrombus detected on ultrasonography or cardiac catheterization
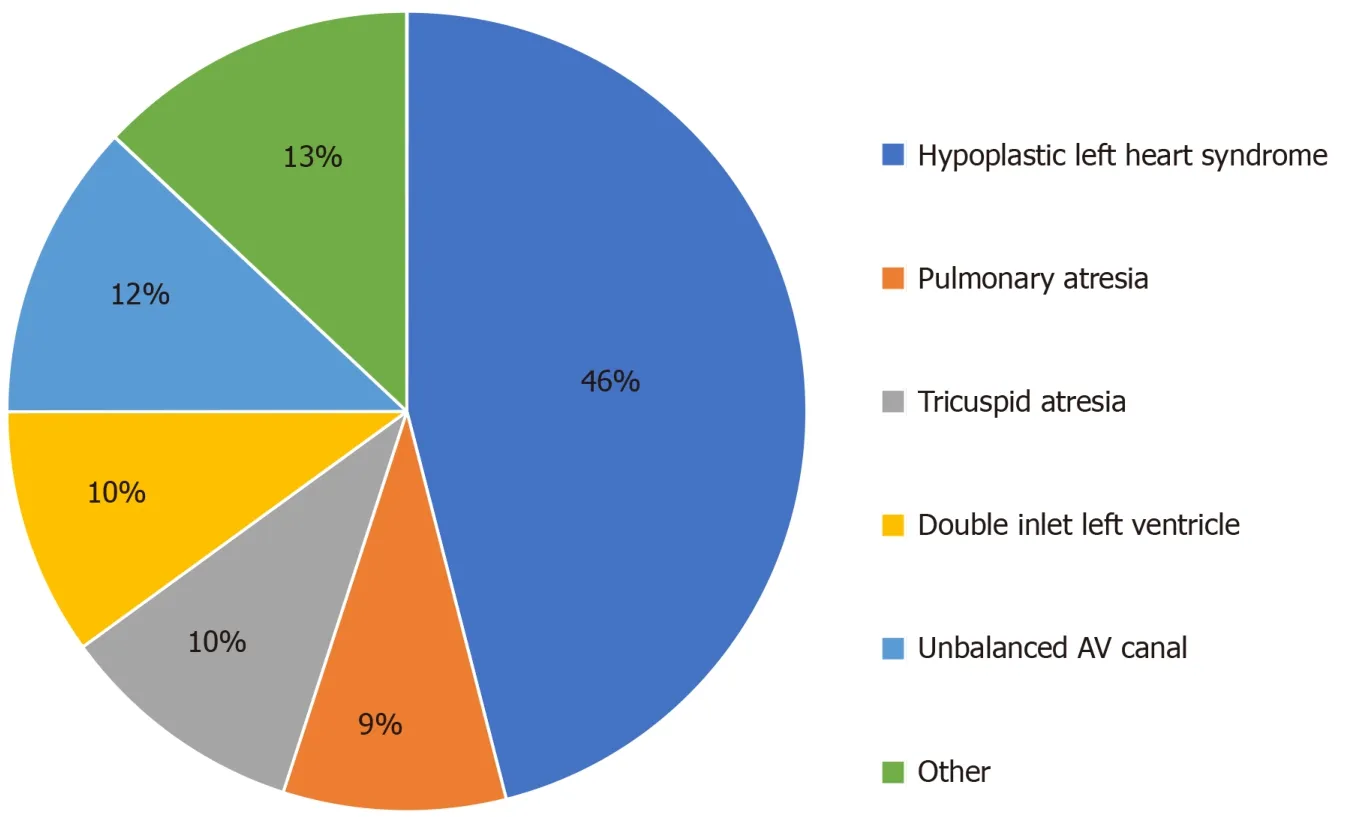
Figure 1 Pie chart summarizing primary cardiac diagnoses, represented as percentages.
Obtaining venous access for pediatric patients who undergo congenital heart surgery can be challenging and might take a significant amount of time after induction of anesthesia or require surgical replacement in some cases.As a result, having a PICCs replaced prior to the surgery will facilitate the preoperative process and save operating room time along.Upper extremity venous access will be at the head of the operation table for easy access by the pediatric cardiac anesthesia team.Moreover,most of the single ventricle patients will require several diagnostic or interventional cardiac catheterization over the course of their life, upper extremity PICCs will decrease the number of the femoral venous access attempts.
There is limited data comparing safety and complication rate of PICCs over CVCs in children.Most of the studies have focused on complications with PICCs in neonates and children with leukemia[8,16].There are few studies published that compare the rates of infection and thrombosis in the hospitalized pediatric patients with PICCs versus CVCs.Noonanet al[17]recently published their experience of the 2709 venous catheters,126 PICCs and 1583 CVCs.They reported that the rates of central line-associated blood steam catheters (CLABSIs) and venous thromboembolism were higher among patients with PICCs[17].Data measuring the different complications between PICCs and CVCs among patients with congenital heart disease is very sparse.In this cohort, we did not report the incidence of the CLABSIs, as we have a very low CLABSI rate at our institute with over 800 CLABSI free days during the timeframe of this study.
The majority of patients (60%) who developed thrombosis had upper body CVCs at some point in addition to the PICCs.There was resolution of thrombosis on subsequent cardiac catheterization prior to the second stage palliative after treating them with low-molecular-weight heparin in 60% (3/5) of patients with thrombosis.There were two patients who had PICCs without additional CVC who developed nonocclusive thrombosis, which resolved prior to the cardiac catheterization.There was no one excluded from the second stage from the group who had only PICCs due to the present of the thrombosis.Another interesting finding from our cohort was that patients who were diagnosed with catheter-related thrombosis developed it in close proximity to the first stage palliation surgery.This suggests that the immediate postoperative period is prothrombotic and early anticoagulation, once the risk of bleeding is reasonable, may be beneficial.
This is a retrospective study at the single center.We do not perform routine upper body ultrasound for thrombosis detection.Imaging for thrombosis identification was directed by symptoms prior second stage cardiac catheterization which might underestimate the rate.Additionally, patients had to survive until pre-stage II diagnostic cardiac catheterization in order to be assessed for the outcomes.The majority of our patients were receiving anti-coagulation which might contribute to this low rate of thrombosis.There is no controlled evaluation for other important clinical indicators like anticoagulation practices or rate of CLABSIs
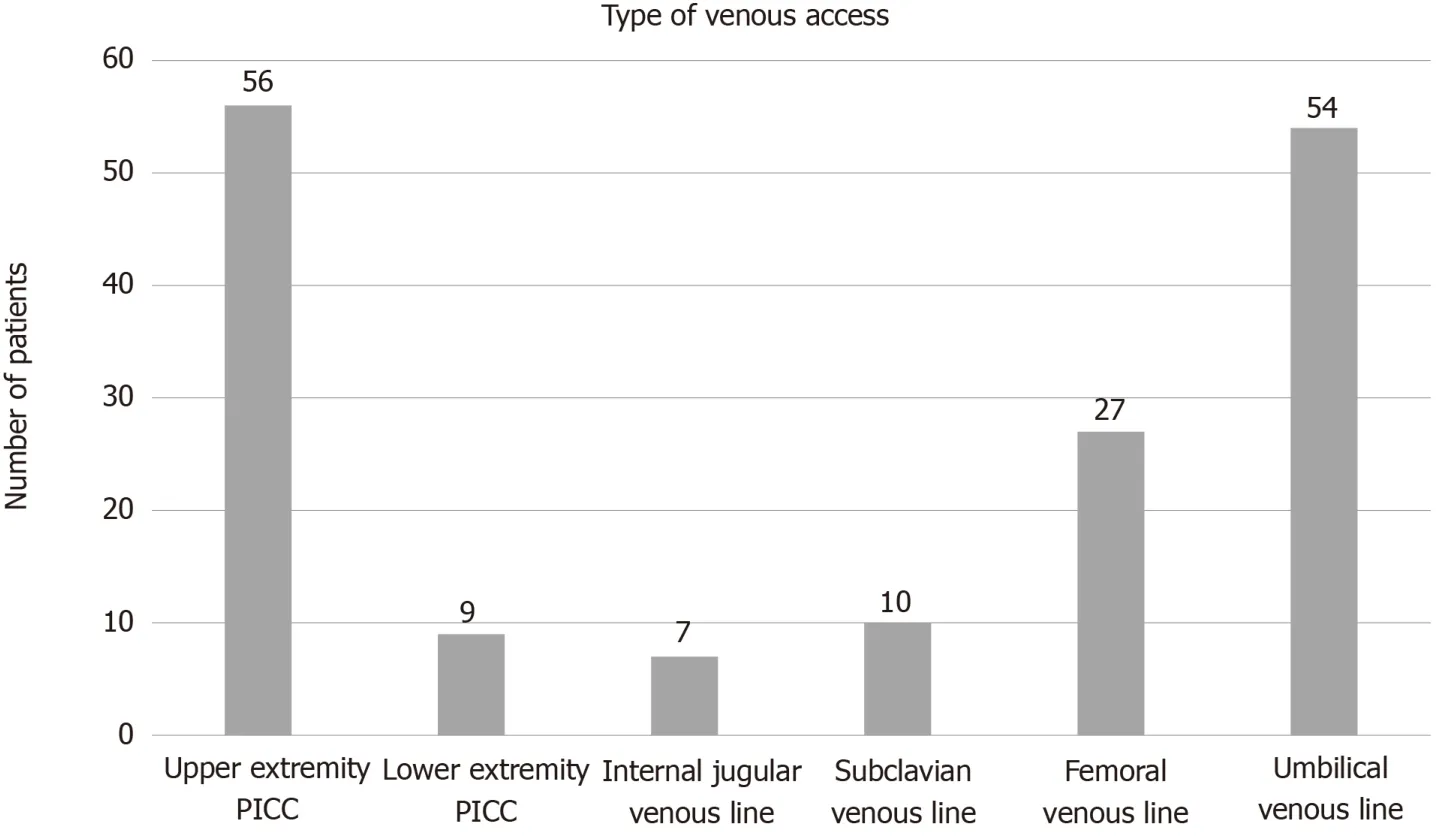
Figure 2 Bar graph illustrating the different types of central venous access utilized for patients with single ventricle physiology prior to their superior cavopulmonary anastomosis.
CONCLUSION
In this retrospective study of children with single ventricle physiology, the placement of percutaneously inserted central catheter in the upper extremity is a reliable way to achieve long-lasting central venous access and associated with a low risk of clinically significant stenosis or thrombosis.
ARTICLE HIGHLIGHTS
Research background
There is risk of stenosis and thrombosis of the superior vena cava after upper extremity central catheter replacement.This complication is more serious among patients with single ventricle physiology, as it might preclude them from undergoing further life-sustaining palliative surgery.Data on the rate of venous thrombosis in children with single ventricle physiology with upper extremity central venous catheters are limited.Also, there is a wide variation in practice regarding the choice of central access in this population across the centers.
Research motivation
To study the risk of using upper body percutaneously inserted central catheter (PICC)in single ventricle patients.The results of this study could be used to develop a multicenter study to determine the risk and benefit of using this type and location of the catheter in this population.
Research objectives
To describe the incidence of thrombosis associated with the use of PICCs in patients with single ventricle physiology.
Research methods
We retrospectively reviewed the charts of patients with single ventricle physiology who underwent second stage palliation surgery.Data regarding the type and duration of central venous access were collected in addition to the data regarding thrombosis or stenosis.
Research results
We reviewed a total of seventy-six patients underwent superior cavopulmonary anastomoses, of which 56 (73%) had an upper extremity PICC at some point prior to this procedure.Median duration of PICC usage was 24 d (25%, 75%:12, 39).Seventeen patients (30%) with PICCs also had internal jugular or subclavian central venous catheters (CVCs) in place at some point prior to their superior cavopulmonary anastomoses with a median duration of 10 days (25%, 75%:8, 14).Thrombus was detected in association with 2 of the 56 PICCs (4%) and 3 of the 17 CVCs (18%) and the incidence of thrombosis was significantly different between the PICCs vs CVCs (P <0.04).All five patients were placed on therapeutic dose of low molecular weight heparin at the time of thrombus detection and subsequent cardiac catheterization demonstrated resolution in three of the five patients.No patients developed clinically significant venous stenos is.
Research conclusions
The placement of PICC in the upper extremity in children with single ventricle physiology was associated with low risk of clinically significant stenosis or thrombosis and provide a reliable way to have long-lasting central venous access.
Research perspectives
Further research and multicenter studies specifically looking at the incidence of complications with upper body PICCs in single ventricle patients are warranted.
 World Journal of Cardiology2020年10期
World Journal of Cardiology2020年10期
- World Journal of Cardiology的其它文章
- Safety and efficacy of soluble guanylate cyclase stimulators in patients with heart failure:A systematic review and meta-analysis
- Risk score for predicting abdominal complications after coronary artery bypass grafting
- Electronic cigarettes—myocardial infarction, hemodynamic compromise during pregnancy, and systolic and diastolic dysfunction:Minireview