
Access to smart devices and utilization of online health resources among older cardiac rehabilitation participants
2020-06-12 08:57:02AbdulghaniSaadiArunKanmanthareddyMaheshAnanthaNarayananKarenHardyMarkWilliamsVenkataAlla
World Journal of Cardiology 2020年5期
Abdulghani Saadi, Arun Kanmanthareddy, Mahesh Anantha-Narayanan, Karen Hardy, Mark Williams,Venkata M Alla
Abstract
Key words: Cardiac rehabilitation; Smart devices; Internet; Perceived barriers
INTRODUCTION
Cardiac rehabilitation (CR) is an important component in the management of patients with heart disease[1]. However, despite abundant evidence demonstrating its benefits and strong recommendations from multiple international and national associations, it remains underutilized[2,3]. Newer models of CR delivery such as home-based CR,which can be implemented and monitored using Internet, have emerged as potential solutions to address some of the barriers to widespread adoption of CR. Furthermore,there is increasing evidence that such models can be equally effective and can be used to complement or extend traditional CR[4]. Highlighting this gap and opportunity, the American Heart Association (AHA) issued a presidential advisory for improving access and utilization of CR. In this advisory, AHA emphasized the importance of adopting newer models and chronic disease management interventions that can be delivered and monitoredviatelephone, Internet or other means of communication[2].
Nonetheless, implementation and success of such models outside the research setting can be limited by participant access to Internet and “smart” “devices”, as well as proficiency and ease of utilization[5,6]. Approximately 90% of the general population uses Internet, with 60% of these reporting use for digital health information (DHI). In contrast, among seniors, approximately 60% report using Internet and less than half of these use Internet to access DHI[7-9]. These observations highlight the barriers to access and underscore the need to understand the reasons for such barriers so as to enable effective delivery of smart models for CR in older adults. The purpose of this study was to explore the availability of Internet/smart devices, current utilization patterns,and proficiency in using them for health-related issues in an older cohort of attendees within an urban outpatient CR program.
MATERIALS AND METHODS
Study participants were enrolled from four American Association of Cardiovascular and Pulmonary Rehabilitation-certified, hospital-based CR programs within a single healthcare system in Omaha, NE, United States. Subjects were recruited over a period of six months in 2018 to participate in a survey consisting of 28 items. Indications for CR were: Stable angina, myocardial infarction, heart failure, percutaneous coronary intervention and cardiac surgery. Internet utilization was measured as usage time per day in hours. On-site subject recruitment and survey administration were conducted by a single investigator. Participation was voluntary and there were no financial or other incentives offered for participation. The survey was only available in English.Subject education status was categorized as “College” (completion of a four-year college degree or greater) and “No College” for participants with some college education, a high school degree, or less. Data were described using averages and percentages. Potential relationships between various items were assessed using Chi square tests for categorical data and Pearson's coefficient for continuous data. A significance level of 0.05 was used, and all data analyses and graphics were developed using the STATA14 statistical package (College Station, TX, United States).
RESULTS
A total of 169 (45%) of the eligible 376 CR participants consented and completed the survey. Patients wishing to forgo participation reported lack of interest as the primary reason. Demographic characteristics of participants are displayed in Table 1. Study participants were 74% male, 90% Caucasian, and 52% had college degrees or above.Among the participants, 15% did not own any smart device and 85% owned a smart device (any of smartphone, tablet or personal computer). Of those who owned a smart device, 34% owned ≥ 3 devices. Smartphone ownership was 47%, and this is consistent with previously published data in this age group[7]. Approximately twothirds of survey participants (63.8%) were daily users with an average Internet time of 1.9 hours (SD ± 1.7). Although 54% of participants used Internet for general purposes such as emails, paying bills, shopping and social media, only 18% used Internet for health-related purposes. Of those who used online health resources, 33% reported accessing online reviews of doctors, 42% used patient portals offered by their electronic health record, and 22% reported that they cross checked or verified information provided by their providers. However, 50% reported either difficulty or they had never tried searching for information related to their medical condition.
The utilization of other DHI was low; 22.2% watched health-related videos online,29.8% used mobile health applications, 12.5% used wearable devices, and 2.8% used smart fitness tools. As for barriers to utilization, 71% of participants reported perceiving no barriers to using Internet, 5.9% did not have Internet, 4.2% could not afford Internet, and 16.9% either found Internet difficult to operate or preferred not to use it. Mean use time was higher in participants who were < 65 years (2.5 h/d)compared to those who were ≥ 65 years of age (1.8 h/d) though this was not statistically significant (NS,P= 0.12). Age had a weak negative correlation with use time (Pearson'sr= -0.16,P= 0.08). Perceived barriers to Internet use were not different between the 2 groups (< 65 years: 24%vs≥ 65 years: 28%,P= 0.63).Participants who had a college education or above had a higher mean use-time of 2.3 h/dvs1.6 h/d in the “No College” group (P= 0.02) (Figure 1). Of all participants without a college education, 39% perceived barriers to Internet use versus only 20% of participants with a college degree who perceived a barrier to Internet use (P= 0.028).Finally, a significantly greater proportion of participants (39%) with an income of <$40 K, perceived barriers to Internet use compared to 17% of those with an income ≥$40 K (P= 0.007).
DISCUSSION
The major findings of our study are: (1) The majority of CR attendees had Internet access and device ownership was high (85% in general, and 47% for smart phone); (2)Despite three quarters of CR attendees reporting no perceived barriers, only 18% used the Internet for DHI; and (3) Consistent with the general population, younger age,college education, and higher income predicted greater use of the Internet and less perceived barriers[9]. In a randomized trial of 80 patients (mean age of 63 years),Widmeret al[10]demonstrated that digital health interventions significantly improved weight loss and reduced cardiovascular-related emergency department visits following acute coronary syndrome. Additionally, the positive impact of “homebased or self-delivery” CR models using a variety of smart technologies has also been demonstrated in patients with chronic heart failure (HF)[11,12]. However, patient education is absolutely essential to the success of such programs. While utilization of Internet and smart devices is common in younger individuals, adoption of technology is less pronounced among older individuals[13]. However, recent trends are encouraging and demonstrate that an increasing number of older individuals are adopting these tools. Our survey indicates that the Internet and device-use in this patient population is consistent with the general population as reported by the Pew Research Center and US Census Bureau[7,8].
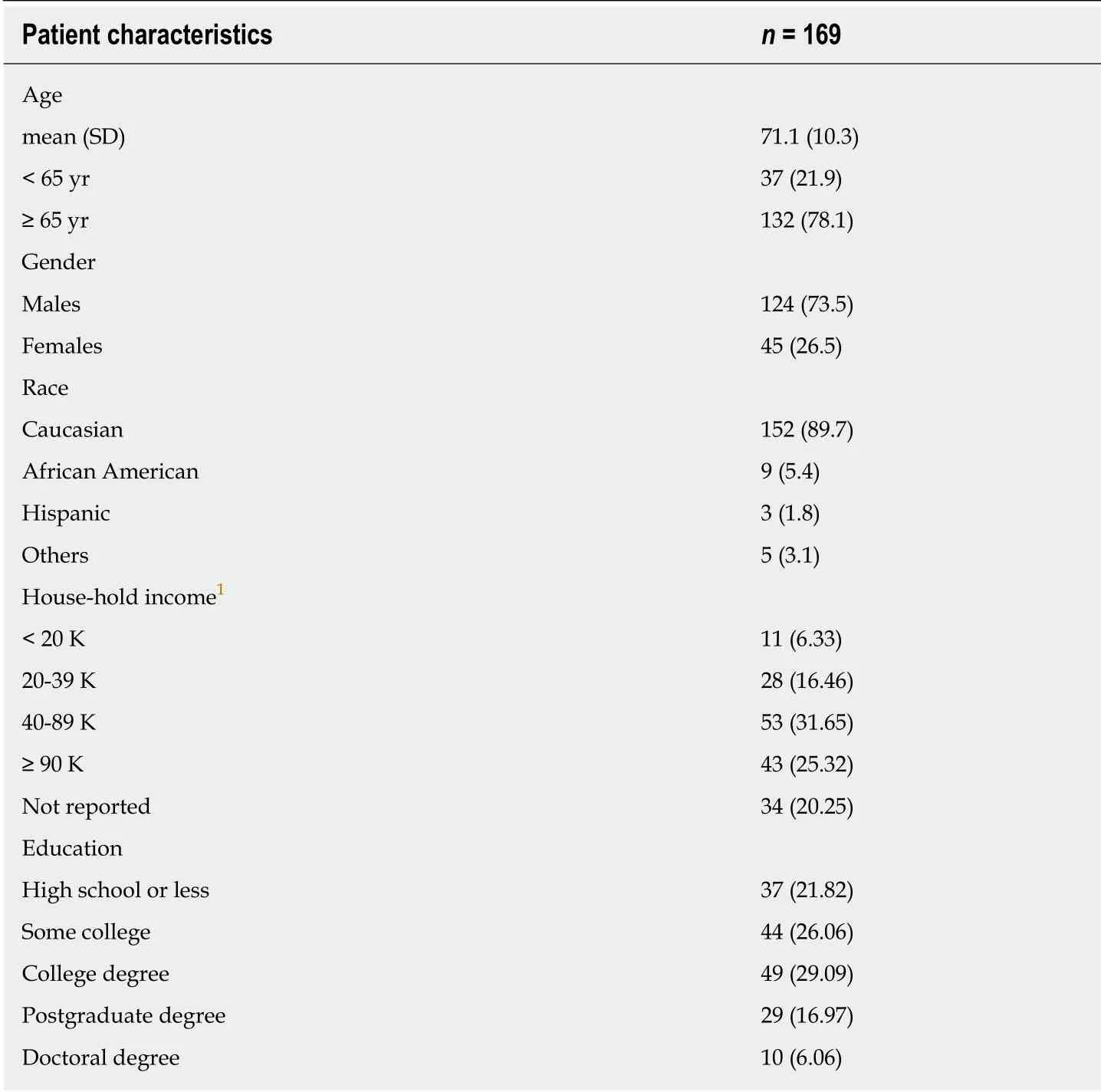
Table 1 Patient characteristics, n (%)
Given the findings in our survey, device ownership and access to Internet are unlikely to be limiting factors in delivering home-based CR using smart technology.However, despite device availability and perception of ease of use, the actual utilization of devices and internet for health-related applications was low with less than one third of study participants using these various devices for accessing DHI.Multiple factors likely contribute to this discrepancy between degree of use of smart tools for general purpose applicationsvshealth-related applications. Some of these factors could be attitudinal,i.e., older patients trust their health care providers much more than younger patients and may prefer to maintain this trust by not seeking online resources and tools[14]. Generational beliefs pertaining to religion, social norms,and preference for personal interactions could also contribute to the reluctance of older adults to use smart devices for DHI[15,16]. Furthermore, older people are more likely to have negative views about the societal impact of Internet and smart devices.Finally, people older than 50 years have been shown to have a greater concern over internet privacy and this may add to their reluctance to use smart devices for DHI[17].
Aside from the aforementioned attitudinal factors, a number of physical and cognitive impairments that are frequently seen in this demographic group are known to contribute to the lower use of smart devices among older adults. These may include visual or hearing impairments, small joint arthritis, tremor, and impaired fine motor skills or coordination, all of which impair ability to use keyboard, mouse or touch screen functions etc[15,16,18]. In addition, memory issues and cognitive dysfunction can hinder ability to retrieve passwords, impair learning ability (necessary for learning new skills), and ability to recall information, thereby resulting in disinterest and disengagement with technology and smart tools[15,16,18]. It is also worth mentioning that a number of devices and apps are designed with the younger user in mind and there is an increasing appreciation of the need to redesign these interfaces to improve technology engagement among senior citizens[19]. Not surprisingly, interfaces that provide healthcare-related information are often more complex and not as user friendly as commercial platforms that cater to entertainment or shopping,etc. This results in technology anxiety and lower self-efficacy in the interactions of older adults with health-related smart apps. All of the above age-related factors interact in a complex fashion and result in decreased technology adoption for health-related applications among older individuals. Interestingly, although younger persons reported greater Internet time (2.5 h)vsolder persons (1.8 h) per day, this difference was not statistically significant although this could be a result of the small sample size of our study.
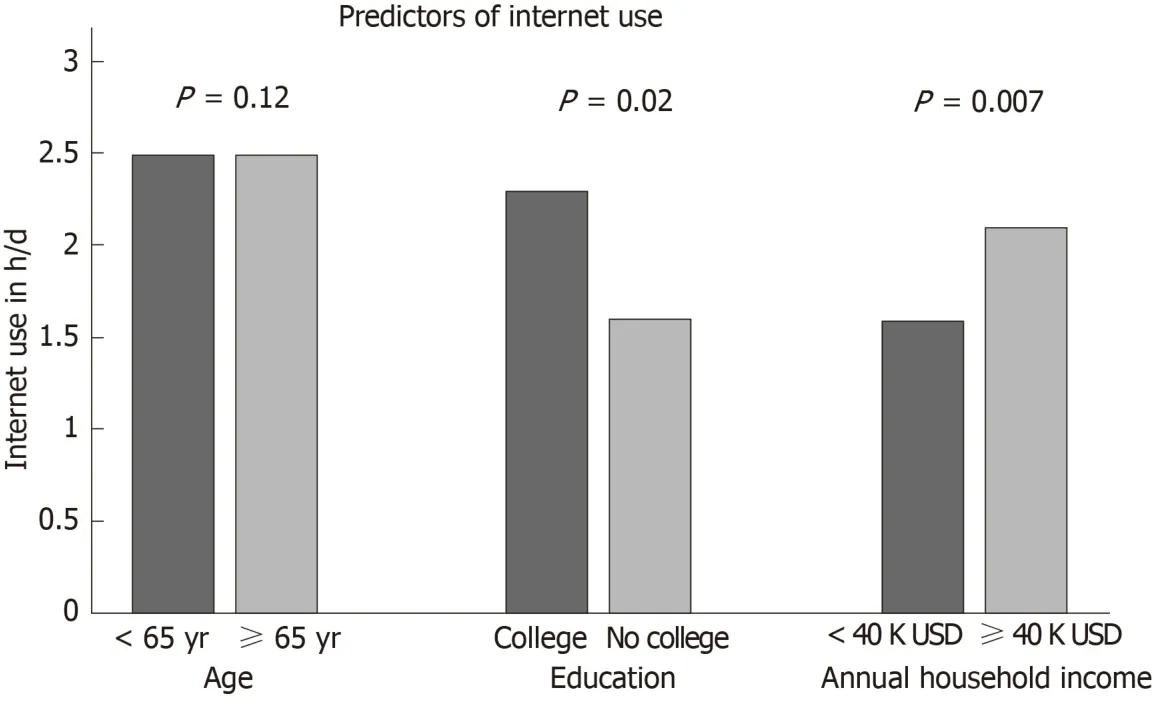
Figure 1 Bar graph of Internet use time in h/d by age, education and annual house-hold income.
A major strength of our study is its novelty and an assessment of the ownership of smart devices, usage patterns and barriers has not been previously identified in the CR population. Our study has some limitations that include small sample size and lack of sample diversity. Our subjects were mostly urban Caucasian males thus limiting the generalizability of our findings. Only 45% of eligible patients responded to our survey and there is a possibility of responder bias. Our survey was not pilottested for validity and should be considered exploratory. Finally, variables such as usage time were self-reported rather than measured and could be impacted by recall bias.
In conclusion, our study demonstrates that most older patients attending CR in an urban metropolitan area have access to Internet/smart devices and do not perceive significant barriers to use. Despite this, most participants did not utilize these devices for health-related applications. Further studies involving larger diverse groups of patients, sampled to account for geographic, racial and gender differences, are needed to add to the existing evidence on the impact of smart technology-based CR although two such studies are currently ongoing[20,21]. In addition to building more evidence to support potential clinical benefits, further research to enhance our understanding of the barriers, our ability to design supportive educational programming and develop protocols that can enable effective and efficient delivery of home-based smart CR are urgently needed.
ARTICLE HIGHLIGHTS
Research background
Newer models of cardiac rehabilitation (CR) delivery are promising and there is increasing evidence that such models can be equally effective and can be used to complement or extend traditional hospital-based CR. Highlighting this opportunity, the American Heart Association issued a presidential advisory emphasizing the importance of adopting these newer models for improving access and utilization of CR. However, effective use of these smart models depends upon patients' ability to use technological media including Internet and smart devices. There is a dearth of knowledge on the availability of internet, ownership of smart devices, usage patterns and barriers to use specifically among CR attendees. CR attendees tend to be older than the general population or patients attending routine chronic disease management clinics. The purpose of this study was to explore the availability of such technology, current utilization and proficiency of use among older CR program attendees. This knowledge can help us understand the feasibility of such smart home-based CR programs in routine clinical practice outside of research trials.
Research motivation
CR is an important component in the management of patients with heart disease. Despite abundant evidence demonstrating its benefits and strong recommendations from multiple international and national associations, it remains underutilized. Potential reasons for this underuse are the need for patients to travel significant distances multiple times in a week, lack of transport, and inflexible schedules. Proposed solutions include newer models of CR delivery such as home-based CR using smart device-based instruction and monitoring. To be able to implement and deliver these home-based CR regimens, we would need to know whether CR attendees who are generally elderly have access to such tools and whether they can use them proficiently. Hence this study was designed to address some of these gaps in knowledge.
Research objectives
The objectives of this study were to assess access to smart devices, predictors of their use and perceived barriers to the use of smart devices among CR attendees.
Research methods
This was an observational study assessing access to internet, smart device ownership and usage among attendees of 4 American Association of Cardiovascular and Pulmonary Rehabilitationcertified, hospital-based CR programs in Omaha, Nebraska, United States. This was a voluntary survey using a pilot survey tool consisting of 28 items. Subjects were recruited over a period of six months in 2018. On-site subject recruitment and survey administration were conducted by a single investigator. The survey was only available in English. Data are described using averages and percentages. Potential relationships between various items were assessed using Chi square tests for categorical data and Pearson's coefficient for continuous data. A significance level of 0.05 was used, and all data analyses and graphics were developed using the STATA14 statistical package (College Station, TX, United States). There has been no such study focusing on CR attendees in United States with most data currently available coming from general population surveys done by the Pew research center.
Research results
We approached 376 attendees of our program, of which 169 responded (45%). Patients as expected were relatively older with a mean age of 71 years, 90% were Caucasians and ≈ 75%were males. Approximately half of the respondents had college education and had a household income of ≥ 40000 USD. Smart device ownership was 84.5% with desktop computer being the most common and preferred device for connecting to the internet. Approximately half of them owned a smart phone and 1/3rdowned multiple devices (phones, tabletsetc.). On average,Internet use was 1.9 h/d. Only about 18% used their smart devices and computers for healthrelated purposes. Utilization of other health information modalities was low, 29.8% used mobile health applications and 12.5% used wearable devices. Of all participants, 72% reported no barriers to using Internet. Education and income were associated positively with measures of utilization and with less perceived barriers while age had a negative correlation. In this survey,we did not address the medical comorbidities that may impact patients' ability to use smart devices for health-related applications and patients' attitudes towards such use.
Research conclusions
Our study demonstrates that most older patients attending CR in an urban metropolitan area have access to Internet/smart devices and do not perceive significant barriers to use. Unlike data from prior decades where elderly patients did not have access to smart devices, our study proves that access is no longer an issue. Despite this, the majority of participants did not utilize these devices for health-related applications. We hypothesize that attitudinal factors such as concern about internet privacy, physical and cognitive impairments that make it difficult to interface with smart devices such as small joint arthritis or memory impairment and lack of education on how to use the devices may be contributing to the low rates of use of smart devices for health related applications. Patient income, educational attainment and age correlated with use of smart devices in our study confirming the findings of prior studies across different age groups. Our findings have significant implications for the efforts to transition CR away from hospitals and closer to home and to create hybrid models of CR. These models not only increase access for patients, increase participation and engagement but may also prove economical and more sustainable for prolonged periods of time. More importantly, the ability to deliver CR in this fashion may be the only way to ensure safety of our patients in this current time of the corona virus 19 pandemic.
Research perspectives
Our study demonstrates that access to smart devices is no longer a limiting factor to the implementation of smart models of home-based CR. Limited use of smart devices for healthcare applications in our elderly patients was likely a result of attitudinal factors, cognitive impairments and lack of proper education. Further research is necessary to confirm our findings in larger diverse groups of patients, sampled to account for geographic, racial and gender differences using validated survey tools. Future avenues for research include investigation into the impact of smart device and apps' design as well as the impact of targeted education to improve technologic proficiency among older adults on the adoption of these technologies. The ultimate success of these smart models of CR will depend on their ability to improve clinical outcomes and their comparative efficacy and cost effectiveness vis-à-vis traditional hospital/center-based CR.
 World Journal of Cardiology2020年5期
World Journal of Cardiology2020年5期
- World Journal of Cardiology的其它文章
- Management of hypertension in COVID-19
- Incidental discovery of right ventricular lipoma in a young female aImaging investigations and diagnosissociated with ventricular hyperexcitability: An imaging multimodality approach
- Preoperative nuclear stress testing in the very old patient population
- Nicotine-induced adrenal beta-arrestin1 upregulation mediates tobacco-related hyperaldosteronism leading to cardiac dysfunction
- Management of adults with coarctation of aorta
- New guidelines for the diagnosis and management of pulmonary embolism: Key changes