
Application of curved ablation in liver cancer with special morphology or location:Report of two cases
2020-05-13 07:34:36NanCaoHuaiJieCaiXiXiSunDeLinLiuBinHuang
World Journal of Clinical Cases 2020年9期
Nan Cao, Huai-Jie Cai, Xi-Xi Sun, De-Lin Liu, Bin Huang
Nan Cao, Huai-Jie Cai, Xi-Xi Sun, De-Lin Liu, The Fourth Clinical Medicine College, Zhejiang Chinese Medical University, Hangzhou 310053, Zhejiang Province, China
Bin Huang, Department of Ultrasound, Zhejiang Hospital, Hangzhou 310013, Zhejiang Province, China
Abstract
Key words: Curved ablation;Ultrasound-guided;Liver cancer;Linear ablation;Case report
INTRODUCTION
Primary liver cancer was the sixth most common cancer in 2018, with incidence and mortality accounting for 6% and 9% of malignant tumors worldwide, respectively.It is the second leading cause of cancer-related death[1,2].Therefore, early detection,diagnosis, and treatment are important means to reduce liver cancer mortality.In recent years, rapid development in the area of imaging intervention, especially ultrasound intervention, has resulted in more minimally invasive techniques for clinical treatment of liver cancer.However, it is difficult to perform ablation with a straight needle guided by ultrasound in some areas of liver cancer.This study reports on two cases of ultrasound-guided curve ablation and introduces detailed indications and points of consideration in the operation of this technique, thus providing new ideas for clinical treatment of liver cancer (Figure 1).
CASE PRESENTATION
Chief complaints and history of present illness
Case 1:A 67-year-old woman was diagnosed with hepatitis and liver cirrhosis for more than five years.In April 2019, enhanced magnetic resonance imaging (MRI) and contrast-enhanced ultrasound (CEUS) showed hypoechoic nodules in the right liver and the patient was diagnosed with liver cancer.
Case 2:A 54-year-old man with abnormal liver function and upper abdominal discomfort presented at our hospital for examination in May 2019.
History of past illness
Case 1:The patient’s history of past illness was unremarkable.
Case 2:The patient underwent a partial hepatectomy procedure for liver cancer five years ago.
Personal and family history
Case 1:The family history was unremarkable.
Case 2:The family history was unremarkable.
Physical examination upon admission
Case 1:No special physical signs were found and the patient did not have any upper abdominal symptoms.
Case 2:There were no other obvious symptoms except slight tenderness in the upper abdomen.
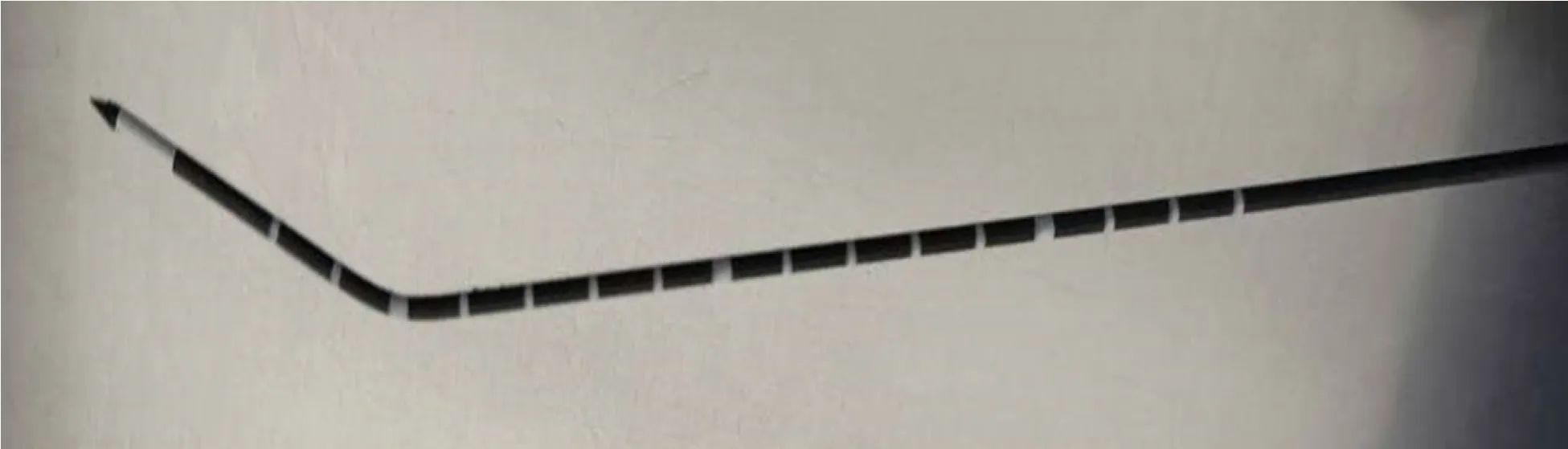
Figure 1 Arc needle image.
Laboratory examinations
Case 1:The serum alpha fetoprotein (AFP) level was 2.43 ng/mL.
Case 2:The serum AFP level was 2.08 ng/mL.
Imaging examinations
Case 1:CEUS of the lesion showed a fast-in and fast-out pattern, while enhanced MRI detected a round long T1 and long T2 signal in the upper posterior segment of the right liver lobe near the liver capsule.The lesion showed a high signal intensity in the diffusion phase, was significantly enhanced in the arterial phase, and was significantly decreased in the portal vein phase (Figure 2).
Case 2:Enhanced MRI and CEUS showed intrahepatic lesions and liver cancer was initially considered (Figure 2).
FINAL DIAGNOSIS
Pathological results for the two patients revealed a hepatocellular carcinoma.
TREATMENT
Case 1:Microwave ablation guided by ultrasound was performed with patient’s informed consent.Since the lesion was near the top of the diaphragm, five surgical schemes were prepared.Scheme 1:Multiple ablations with a single needle.This technique may result in bleeding and needle track implantation, may have insufficient safety boundaries, is time-consuming, and has high requirements for the operator.Scheme 2:Concurrent ablation with multiple needles.The ablation range is sufficient in this technique, but its cost is high and liver tissue injury is too much.Scheme 3:Umbrella needle ablation.Because the focus is in close proximity to the diaphragm,lungs, and large blood vessels, tissue can be easily damaged.Scheme 4:Artificial hydrothorax.The needle path might disappear after the artificial hydrothorax,increasing the difficulty of the puncture.Scheme 5:Ablation with a curved needle(designed by the author and commissioned by the manufacturer, Figure 3).
Under general anesthesia, the patient was placed on the left side.The tissue was sterilized and the condition of the lesion and surrounding tissue was evaluated again.A needle was inserted according to the path set prior to the operation and its direction was regulated in real-time under the guidance of ultrasound (Figure 3).The anterior segment of the arc needle was kept parallel to the long axis of the lesion.When the needle tip reached the anterior segment of the lesion, ablation was initiated with the power set at 60 W.After the lesion was completely vaporized and covered, the cold circulation was closed and the needle was pulled out.The ablation range was evaluated by CEUS after the ablation procedure was completed.
Case 2:Since the lesion was located behind the liver cyst, two surgical schemes were prepared.Scheme 1:The cyst in front of the lesion is extracted and the lesion ablated.However, this method has previously hurt the patient twice.Scheme 2:Curved needle ablation, bypassing the anterior cyst and surrounding blood vessels for ablation(Figure 4).
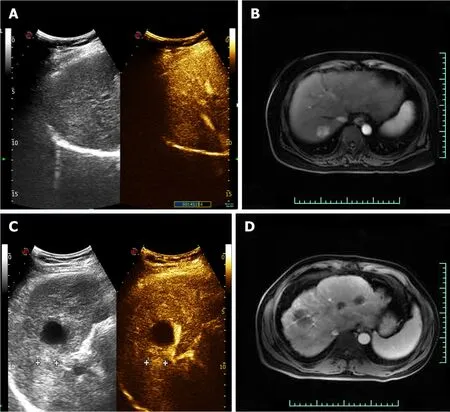
Figure 2 Preoperative contrast-enhanced ultrasound and magnetic resonance imaging findings.
This patient underwent the same procedure as the first patient, following a preoperatively designed arc path and avoiding surrounding vessels and anterior cysts(Figure 4).
One month after the operation, enhanced MRI results for ablation foci and surrounding areas exhibited no enhancement.
OUTCOME AND FOLLOW-UP
Case 1:One month after the operation, CEUS and enhanced MRI results for ablation foci and surrounding areas exhibited no enhancement (Figure 5).
Case 2:One month after the operation, CEUS and enhanced MRI results for ablation foci and surrounding areas exhibited no enhancement (Figure 5).
DISCUSSION
The development of liver cancer is slow, usually accompanied by liver cirrhosis that can cause abnormalities within the liver.A long time is needed to become a pathologically advanced liver cancer such as HCC.However, sometimes HCC growth is very fast.At present, the main methods for the treatment of liver cancer are surgery,local ablation, transarterial chemoembolism, radiotherapy, drug therapy, and immunotherapy.Liver cancer patients generally have partial liver function damage,reduction of coagulation function, and surgery intolerance.However, because of the complex liver cancer blood supply, it is difficult for transcatheter arterial chemoembolization to cause complete tumor tissue necrosis.The statistics for II resection specimens show that the complete death rate is only 22%-72%[3].Chemotherapy, radiotherapy, and immunotherapy have side effects and their cost for patients needing long-term medication is too high[4-6].Microwave ablation causes less trauma and comes at a lower cost[7,8].However, it is difficult to perform ablation of the tumors near the gallbladder, diaphragm, and other organs.In order to solve this problem, the curved ablation technique was designed.
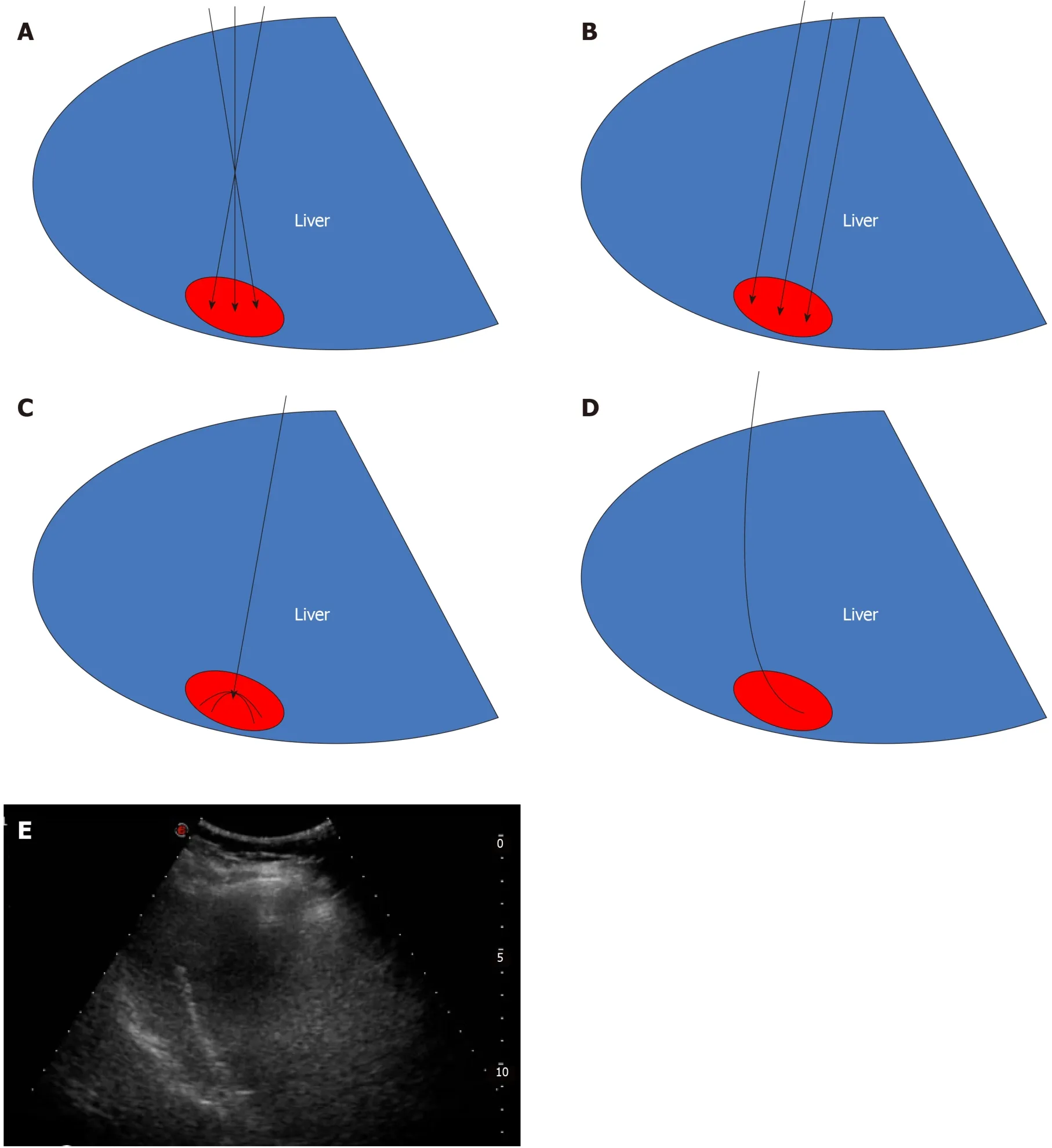
Figure 3 Four pre-operative options and actual ablation path diagram for Case 1.
The curved ablation method has high requirements for the operator who should have several years of experience in the ablation of liver cancer.
Two cases of curved ablation in this study are summarized and the following conclusions are made:(1) Compared to straight needle ablation, curve ablation is more demanding for operators;(2) General patient state has to be assessed prior to operation;(3) Pre-operation needle approach design involves the following steps:Mark the screen according to the straight needle route;draw angle N between the long axis of the tumor and the path of the straight needle, then measure angle N.The incident angle is offset by N degrees in the direction of the original needle;under the guidance of real-time ultrasound, adjust the direction of the needle, so that the needle advances within the design route until the curved end of the needle is parallel to the long axis of the lesion (Figure 6);(4) The surgeon should work closely with the anesthesiologist to control the patient's breathing as needed and, if necessary, carry out one-lung respiration;(5) If necessary, virtual fusion navigation imaging technology has to be used to evaluate the localization navigation and postoperative ablation range;and (6) The ablation range has to be evaluated by CEUS immediately after operation and by enhanced MRI re-examination 1 mo after operation.
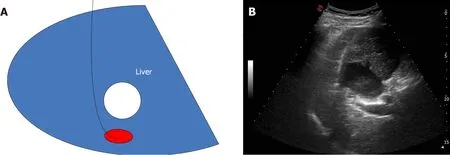
Figure 4 Preoperative ablation path diagram and actual ablation path diagram for Case 2.
Curved ablation has been demonstrated to be feasible, safe, economical, and effective in these two cases, expanding the adaptive range of ultrasound-guided percutaneous ablation of liver cancer.
CONCLUSION
The curved ablation technique has special advantages for the ablation of liver cancer at specific sites.Its effectiveness needs to be confirmed by investigating more cases.
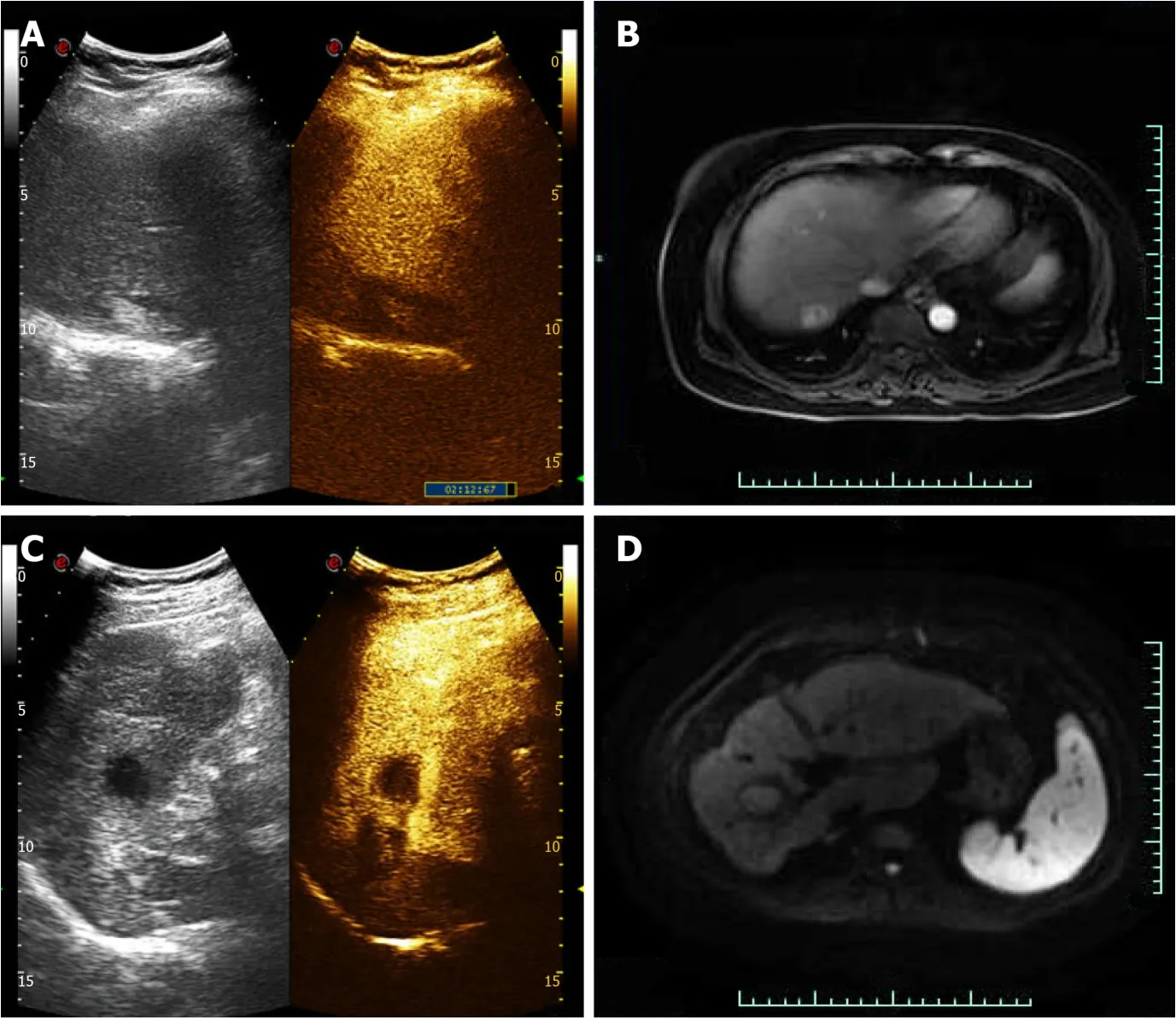
Figure 5 One month after surgery, two patients showed no enhancement on contrast-enhanced ultrasound and magnetic resonance imaging.
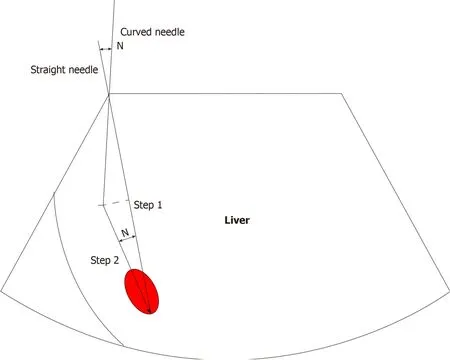
Figure 6 Estimation method for path angle.
 World Journal of Clinical Cases2020年9期
World Journal of Clinical Cases2020年9期
- World Journal of Clinical Cases的其它文章
- Rare primary lymphoepithelioma-like carcinoma of the renal pelvis
- Portal hypertension in a patient with biliary hamartomas:A case report
- Mesonephric adenocarcinoma of the uterine cervix with rare lung metastases:A case report and review of the literature
- Endoscopic ultrasonography elastography in the diagnosis of intrapancreatic ectopic spleen:A case report
- Giant ventral hernia simultaneously containing the spleen, a portion of the pancreas and the left hepatic lobe:A case report
- COVlD-19 managed with early non-invasive ventilation and a bundle pharmacotherapy:A case report