
Risks of incident heart failure with preserved ejection fraction in Chinese patients hospitalized for cardiovascular diseases
2019-12-31 04:45:24JunXiaZHANGYiXianLIUChunLeiXIAPengCHUXinLiangQULinLinZHUShaoLiangCHEN
Journal of Geriatric Cardiology 2019年12期
Jun-Xia ZHANG, Yi-Xian LIU, Chun-Lei XIA, Peng CHU, Xin-Liang QU, Lin-Lin ZHU, Shao-Liang CHEN
Department of Cardiology, Nanjing First Hospital, Nanjing Medical University, Nanjing, China
Abstract Background Endogenous aldehyde damages DNA and potentiates an ageing phenotype. The aldehyde dehydrogenase 2 (ALDH2) rs671 polymorphism has a prevalence of 30%-50% in Asian populations. In this study, we aimed to analyze risk factors contributing to the development of heart failure with preserved ejection fraction (HFpEF) along with the genetic exposure in Chinese patients hospitalized with cardiovascular diseases (CVD). Methods From July 2017 to October 2018, a total of 770 consecutive Chinese patients with normal left ventricular ejection fractions (LVEF) and established CVD (hypertension, coronary heart diseases, or diabetes) were enrolled in this prospective cross-sectional study. HFpEF was defined by the presence of at least one of symptom (dyspnoea and fatigue) or sign (rales and ankle swelling) related to heart failure; N-terminal pro-B-Type natriuretic peptide (NT pro-BNP ≥ 280 pg/mL); LVEF ≥ 50%; and at least one criterion related to elevated ventricular filling pressure or diastolic dysfunction (left atrial diameter > 40 mm, E/E’ ≥ 13, E’/A’ < 1 or concurrent atrial fibrillation). Logistic regression was performed to yield adjusted odds ratios (ORs) for HFpEF incidence associated with traditional and/or genetic exposures. Results Finally, among 770 patients with CVD, 92 (11.9%) patients were classified into the HFpEF group according to the diagnostic criteria. The mean age of the participants was 67 ± 12 years, and 278 (36.1%) patients were females. A total of 303 (39.4%) patients were ALDH2*2 variant carriers. In the univariate analysis, eight exposures were found to be associated with HFpEF: atrial fibrillation, ALDH2*2 variants, hypertension, age, anaemia, smoking, alcohol consumption and sex. Multivariable logistic regression showed that 4 ‘A’ variables (atrial fibrillation, ALDH2*2 variants, age and anaemia) were significantly associated with an increased risk of HFpEF. Atrial fibrillation was associated with a 3.8-fold increased HFpEF risk (95% CI: 2.21-6.61, P < 0.001), and the other three exposures associated with increased HFpEF risk were the ALDH2*2 variant (OR = 2.41, 95% CI: 1.49-3.87, P < 0.001), age (OR = 2.14, 95% CI: 1.27-3.60, P = 0.004), and anaemia (OR = 1.79, 95% CI: 1.05-3.03, P = 0.032). These four variables predicted HFpEF incidence in Chinese CVD patients (C-statistic = 0.745, 95% CI: 0.691-0.800, P < 0.001). Conclusions 4 A traits (atrial fibrillation, ALDH2*2 variants, age and anaemia) were associated with an increased risk of HFpEF in Chinese CVD patients. Our results provide potential clues to the aetiology, pathophysiology and therapeutic targets of HFpEF.
Keywords: Aldehyde dehydrogenase 2; Cardiovascular diseases; Diastolic dysfunction; Heart failure with preserved ejection fraction; Risk factor
1 Introduction
Heart failure is an end-stage syndrome with a high mortality rate due to the deterioration of a variety of cardiac structural and functional abnormalities. In heart failure with preserved ejection fraction (HFpEF), the systolic function assessed by the left ventricular ejection fraction is not reduced; however, the diastolic function is compromised. The disturbed diastolic function raises left ventricular filling pressure and left atrial pressure, leading to pulmonary venous congestion.[1,2]HFpEF is a syndrome related to senescence, and the risk factors for it have not been fully explored.[3]Racial or ethnic differences may exist in the development of HFpEF. As implied in a multiethnic study, lipoprotein (a)-related risk of HFpEF is solely evident in white participants.[4]Conversely, black patients are observed to have higher readmission rates and lower mortality risk compared with white patients.[5]Likewise, black participants with HFpEF in the TOPCAT trial tended to have a higher re-hospitalization risk than white participants.[6]Therefore, racial/ethnical background should be underscored when evaluating risk factors for HFpEF incidence. As the ageing population increases sharply in China, HFpEF represents the dominant phenotype of all patients diagnosed with heart failure. However, the demographic characteristics and risk factors for Chinese patients with HFpEF are still scarce.
In addition, whether genetic risk factors contribute to the development of HFpEF needs to be determined. Moreover, most genetic association studies of HFpEF are unadjusted for clinical predictors.[7,8]A genome-wide association study conducted in Caucasian subjects revealed that a single-nucleotide polymorphism of rs6696224 in the transforming growth factor-beta receptor 3 gene (TGFBR3) was associated with HFpEF. However, the association did not persist when clinical predictors were considered.[9]Congruently, in postmenopausal African American women, high-risk apolipoprotein L1 (APOL1) genotypes were associated with HFpEF hospitalization, but the associations were underpowered when adjusting for baseline eGFR, indicating thatAPOL1increased the risk of HFpEF by aggravating renal function rather than by directly affecting the cardiovascular system.[10]Likewise, few association studies of clinical risk factors have included genetic exposures as covariates to predict risks of diseases. The aldehyde dehydrogenase 2 (ALDH2) gene, which encodes a mitochondrial enzyme that metabolizes acetaldehyde and endogenous lipid aldehydes, assumes a single nucleotide polymorphism (rs671) with a prevalence of approximately 30%-50% in the Asian population. TheALDH2*2variant is involved in left ventricular diastolic dysfunction in animal models[11]and in ageing overweight patients.[12]
In this hospital-based study, we evaluated genetic exposure to theALDH2 rs671polymorphism and other risk factors for HFpEF in Chinese patients hospitalized with cardiovascular diseases (CVD). Our study may provide preventive and therapeutic targets for HFpEF in Chinese CVD patients.
2 Methods
2.1 Study design and population
This is a prospective, single-center, cross-sectional, hospital-based study designed to assess the risk factors for HFpEF incidence in Chinese CVD patients. Subjects were consecutively enrolled from Nanjing First Hospital, a public tertiary care university hospital in Nanjing, China. Patients were recruited for this study if they were (1) ≥ 18 years old; (2) with CVD, defined as a diagnosis of coronary heart disease, hypertension or type 2 diabetes; and (3) had a left ventricular ejection fraction (LVEF) ≥ 50% by echocardiography. The definition of coronary heart disease was stenosis of the main coronary arteries ≥ 50% using percutaneous coronary angiography or coronary computed tomography angiography findings. The definition of hypertension was systolic blood pressure ≥ 140 mmHg, diastolic blood pressure ≥ 90 mmHg or pharmacological treatment. The definition of type 2 diabetes was fasting blood glucose ≥ 7.0 mmol/L, random blood glucose ≥ 11.1 mmol/L and HbA1c > 6.5% or the use of hypoglycaemic medications. Body mass index (BMI) was calculated as weight in kilograms divided by height in metres squared. The main exclusion criteria were primary diagnoses of atherosclerosis (stenosis of the main coronary arteries < 50%), congenital heart diseases, arrhythmia, lung diseases, aortic dissection, peripheral vascular diseases, pericardial diseases, myocarditis, hypertrophic cardiomyopathy, heart valvular diseases, cardiophobia, costal chondritis, shock, thyroid diseases, infection or concomitant liver or renal dysfunction. Of the 2867 CVD patients hospitalized in the Department of Cardiology from July 2017 to October 2018, 664 patients were excluded because they lacked both serum N-terminal pro-B-Type natriuretic peptide (NT pro-BNP) tests and echocardiography records, 433 patients were excluded because LVEF < 50%. Finally, 770 patients were included in this study. The study protocol and informed consent were approved by the institutional review committee of Nanjing First Hospital. Written informed consent for participation was obtained from all enrolled patients.
2.2 Biochemical analyses and genotyping
The patients’ fasting blood samples were collected the morning after admission for routine measurement of haematology, clinical chemistry, biomarkers of heart failure and myocardial injuries. The serum NT pro-BNP assay and the genotyping ofALDH2were described at length previously.[13]
2.3 Cardiac structure and function assessment by echocardiography
The collection and processing of echocardiographic data have previously been described.[13]Briefly, transthoracic echocardiography was performed according to the international accepted guidelines.[14]The Cardiovascular Imaging Core laboratory of the Nanjing First Hospital provided oversight and imaging protocol guidelines to ensure the quality of the echocardiograms. The LVEF was determined either by Simpson’s biplane method or the area-length method using the accepted mathematical models. In line with the current European Society of Cardiology guidelines,[15]we used an LVEF cut-off of ≥ 50% for HFpEF. Left atrial enlargement was evaluated by the left atrial diameter (LAD). To appraise left ventricular structure changes, left ventricular diameter in diastole and left ventricular diameter in systole were examined. To assess systolic function of the left ventricles, LVEF, stroke volume, and fractional shortening (FS) were recorded. To evaluate the diastolic function of the left ventricles, peak E and peak A transmitral flow velocities were obtained by colour flow Doppler mode. Furthermore, peak E’ and peak A’ myocardial tissue velocities of were obtained by tissue Doppler mode. The ratios of E/A, E’/A’ and E/E’ were calculated accordingly.
2.4 Definition of HFpEF
The occurrence of HFpEF was independently adjudicated by two cardiologists who were blind to the result of theALDH2genotyping and demographic information of patients. The diagnosis of HFpEF was based on the following criteria: (1) patients had at least one symptom or sign of dyspnoea, fatigue, rales or ankle swelling; (2) LVEF ≥ 50%; (3) NT-proBNP ≥ 280 pg/mL; and (4) LAD > 40 mm, E/E’ ≥ 13, E’/A’ < 1 or concurrent atrial fibrillation.
2.5 Statistical analyses
We performed baseline descriptive statistics according to the incidence of HFpEF. Continuous values were expressed as the mean ± SD for variables with a normal distribution or medians and 25thto 75thinterquartile range for those with a non-normal distribution. Categorical variables were expressed as numbers and percentages. The threshold for statistical significance was a two-sided significance level of 0.05. Numerical variables were analysed by Student’sttest for normal data and Wilcoxon rank sum scores for non-normally distributed data; categorical variables were analysed by chi-square test or Fisher’s exact test when necessary. Hardy-Weinberg equilibrium was used to assess the representativeness of the patients. The crude laboratory assay variables were adjusted for age using logistic regression analysis except for NT-proBNP, which was adjusted for age and creatinine. A bivariate correlation analysis was used to explore the collinearity of the covariates.
Variables that were significantly associated with HFpEF in the univariate analysis (ALDH2variants, hypertension, atrial fibrillation, age, haemoglobin, smoking, alcohol consumption and sex) were tested by multivariate logistic regression usingP< 0.05 as an entry threshold and HFpEF as the dependent variable; the continuous haemoglobin variable was dichotomized by anaemia (defined as haemoglobin < 120 g/L) or not in this model. Age was dichotomized as ≥ 70 years or not.ALDH2variants, anaemia, age and atrial fibrillation were fitted for model discrimination to predict patients to be diagnosed with HFpEF using C-statistics (Model 1). Model calibration (agreement between observed and expected cases) was tested using the Hosmer-Lemeshow goodness-of-fit test. For assessment of robustness of the risk forALDH2variants, the C-statistics calculated by a model with three traditional variables (Model 2, anaemia, age and atrial fibrillation) were compared with that calculated by Model 1.
A comparison of the C-statistics was conducted with theZtest using Analyse-it 2.0 (Hearne Scientific Software Pty Ltd, Melbourne 3000, Australia). All other statistical analyses were performed with SPSS 16.0 (SPSS Inc., Chicago, IL, USA).
3 Results
After screening according to the pre-specified inclusion and exclusion criteria, a final cohort of 770 patients with CVD and normal LVEF on echocardiography underwent genotyping in Nanjing First Hospital from July 2017 to October 2018. Among them, 92 (11.9%) patients with CVD were classified into the HFpEF group. Overall, the mean age of participants was 67 ± 12 years, and 278 (36.1%) patients were females.
3.1 Traditional and genetic exposures of CVD patients with HFpEF vs. those without HFpEF
Between the HFpEF and non-HFpEF groups, those with HFpEF were older (74 ± 10 yearsvs.66 ± 11 years,P< 0.001) and more often female (51.1%vs.34.1%,P= 0.001). Additionally, the prevalence of hypertension and atrial fibrillation were higher in the HFpEF patients (85.9%vs.75.1%,P= 0.022 and 32.6%vs.9.6%,P< 0.001, respectively). Conversely, the lifestyle exposures, alcohol consumption and smoking, were less frequently observed in the HFpEF patients. There was no statistically significant difference in BMI or the diagnosis of coronary heart diseases and diabetes, as shown in Table 1.
In the 770 recruited patients, the genotype distributions did not depart from the Hardy-Weinberg equilibrium forALDH2(chi-square = 0.587,P= 0.746). The frequencies ofALDH2*1/*1,ALDH2*1/*2,ALDH2*2/*2genotypes were 60.6% (467 of 770), 35.3% (272 of 770), and 4.0% (31 of 770), respectively. The frequency of theALDH2*2allele was 21.7% (334 of 1540) in our study. We combined theALDH2*1/*2andALDH2*2/*2genotypes into theALDH2*2genotype. Finally, as presented in Table 1, among 303 patients with theALDH2*2variant types, 51 (55.4%) patients were in the HFpEF group and 252 (37.2%) patients were in the non-HFpEF group (P< 0.001).

Table 1. Baseline characteristics and genetics of HFpEF vs. non-HFpEF patients.
Considering that lifestyles are external exposures from the environment, even though there are correlations between sex, alcohol consumption and smoking, we kept them, along with atrial fibrillation,ALDH2*2variants, hypertension and age, as risk factors for further logistic regression analysis.
3.2 Laboratory characteristics of CVD patients with HFpEF vs. those without HFpEF
Because the value of NT-proBNP might be influenced by age and renal function, the difference in NT-proBNP between the patients with HFpEF and without HFpEF was adjusted for age and creatinine. All other laboratory assays were adjusted for age.
The cardiac biomarker level of NT-proBNP was higher in the HFpEF patients before and after adjustment, whereas no significant difference was observed in creatine phosphokinase (CPK) or the MB isoenzyme of CPK (CPK-MB). The uric acid level was significantly higher in the HFpEF patients. After adjustment for age, theP-value for uric acid was unexpectedly reduced (Table 2). The bivariate correlation analysis detected collinearity between uric acid and age (r = 0.104,P< 0.001). The incidence of HFpEF was associated with lower haemoglobin levels, and the trend was still obvious after age adjustment. Significant differences in creatinine, triglycerides and alanine aminotransferase between the patients with and without HFpEF were observed, whereas the difference was underpowered when adjusted for age, as shown in Table 2.
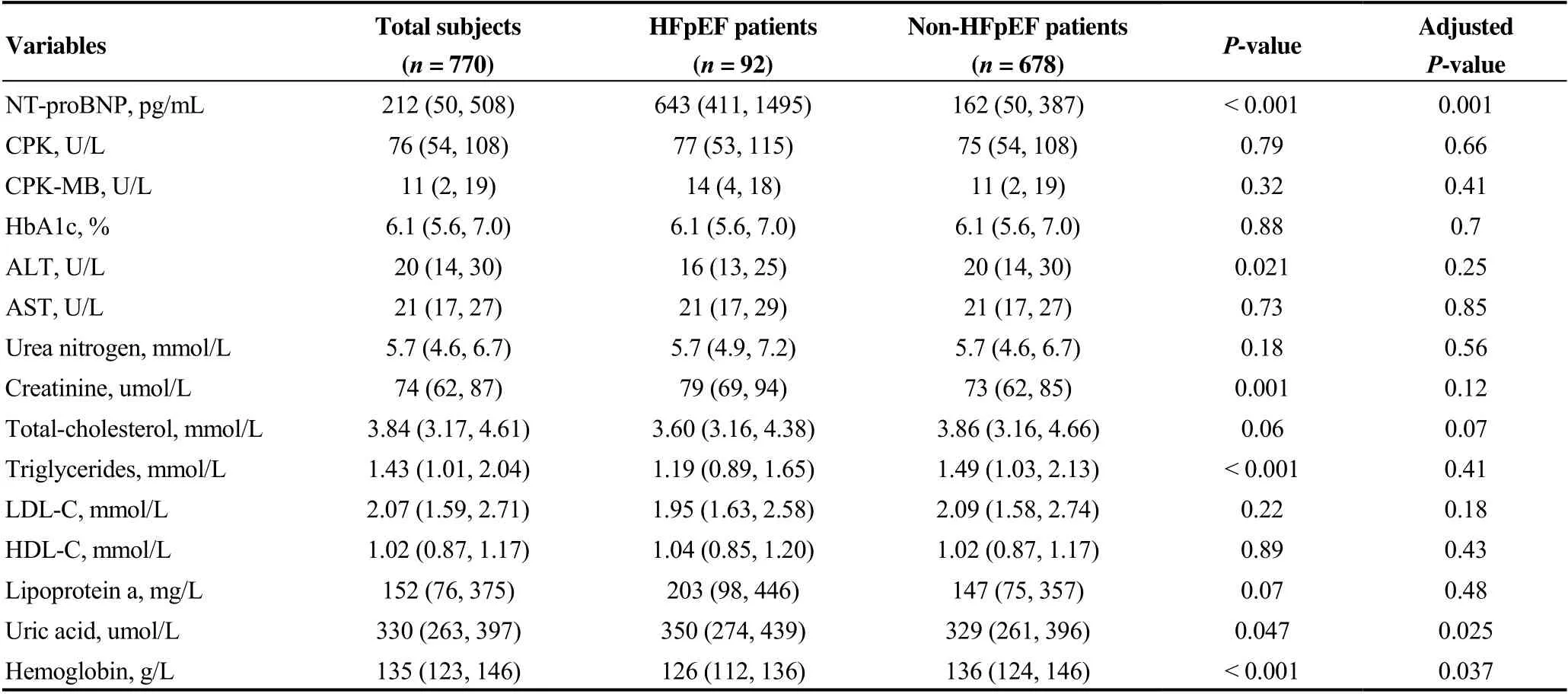
Table 2. Laboratory characteristics of HFpEF vs. non-HFpEF patients.
No other biochemical results regarding lipid metabolism, liver function or renal function were observed to be associated with the incidence of HFpEF (Table 2). Because NT- proBNP is an endogenous neuroendocrinal response of heart failure rather than exposure, NT-proBNP was excluded as a candidate HFpEF risk factor for further study. Therefore, haemoglobin was selected as the only laboratory finding for multivariable analysis.
3.3 Echocardiographic characteristics of CVD patients with HFpEF vs. patients without HFpEF
As for the echocardiography, HFpEF patients had higher left atrial pressure, as demonstrated by larger left atrium size and more frequent pulmonary hypertension [pulmonary artery systolic pressure (PASP) ≥ 35 mmHg]. The median LVEF in the HFpEFvs.non-HFpEF groups was 63% (61%- 65%)vs.64% (63%-66%),P= 0.004, indicating a mild but significant decrease in left ventricular contraction in the HFpEF patients. Consistently, FS was reduced in the HFpEF patients. The transmitral blood flow velocities in early and atrial systole phases were promoted (peak E velocity and peak A velocity), and the E/E’ ratio was elevated, implying the impaired tolerance of the pressure volume response and diastolic dysfunction in HFpEF patients (Table 3).
Because the cardiac structural and functional abnormalities detected by echocardiography reflect the underlying pathophysiology of HFpEF, we did not select echocardiographic results as risk factors for predicting HFpEF incidence except for elevated PASP, since pulmonary hypertension is not merely an index of echocardiography, it might be a clinical syndrome. However, it was excluded because there was collinearity of atrial fibrillation with elevated PASP (r = 0.387,P< 0.001).
3.4 Multivariable logistic regression for predicting HFpEF
After univariate analysis, seven traditional exposures (old age, female sex, atrial fibrillation, anaemia, smoking, alcohol consumption and hypertension) and one genetic exposure (ALDH2*2variants) were included in the multivariable regression analysis. The association of sex, smoking, alcohol consumption and hypertension with HFpEF was attenuated and no longer significant in the adjusted model. The final HFpEF-specific risk model included four variables:ALDH2*2variants, atrial fibrillation, old age and anaemia. The Hosmer-Lemeshow test showed good fitness of the model (χ2= 1.855,P= 0.865). Specifically, atrial fibrillation was associated with a nearly 4-fold risk of HFpEF, as displayed in Table 4. The four variables (Model 1) predicted HFpEF incidence with a C-statistic of 0.745 (95% CI: 0.691-0.800,P< 0.001).
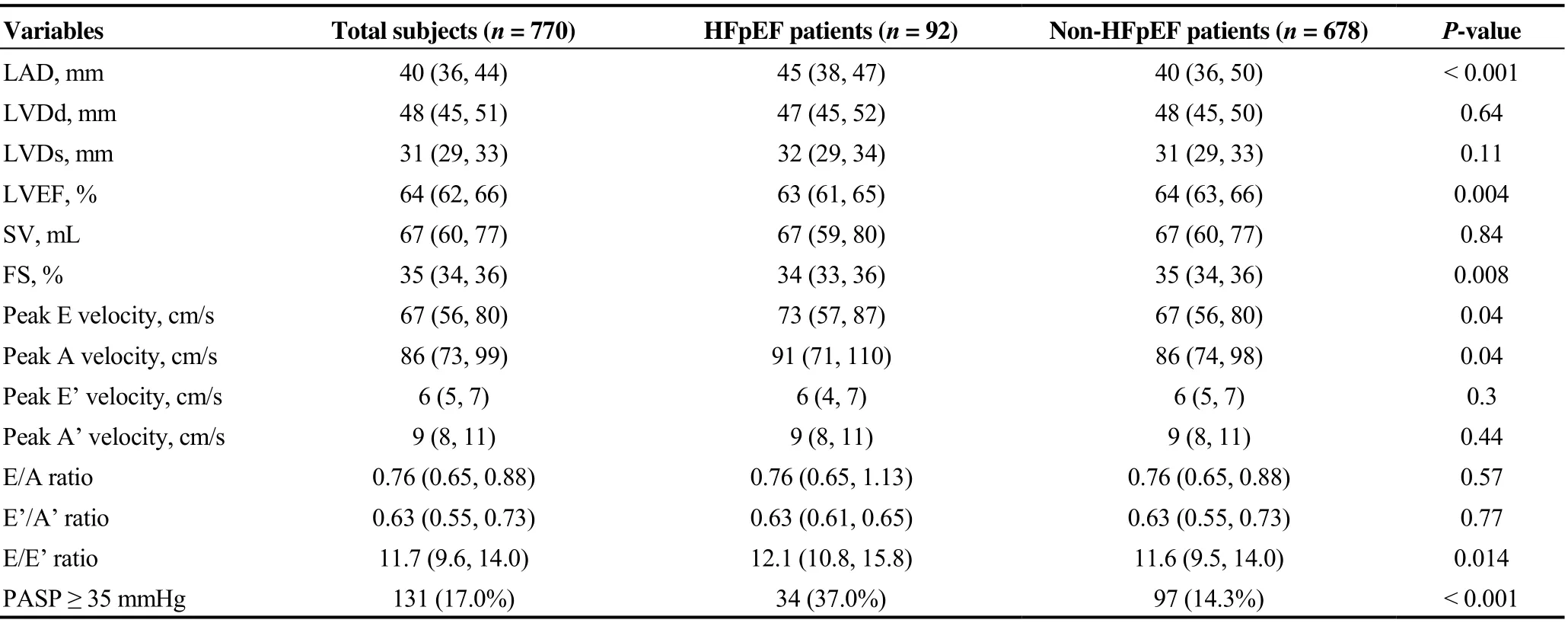
Table 3. Laboratory characteristics of HFpEF vs. non-HFpEF patients.
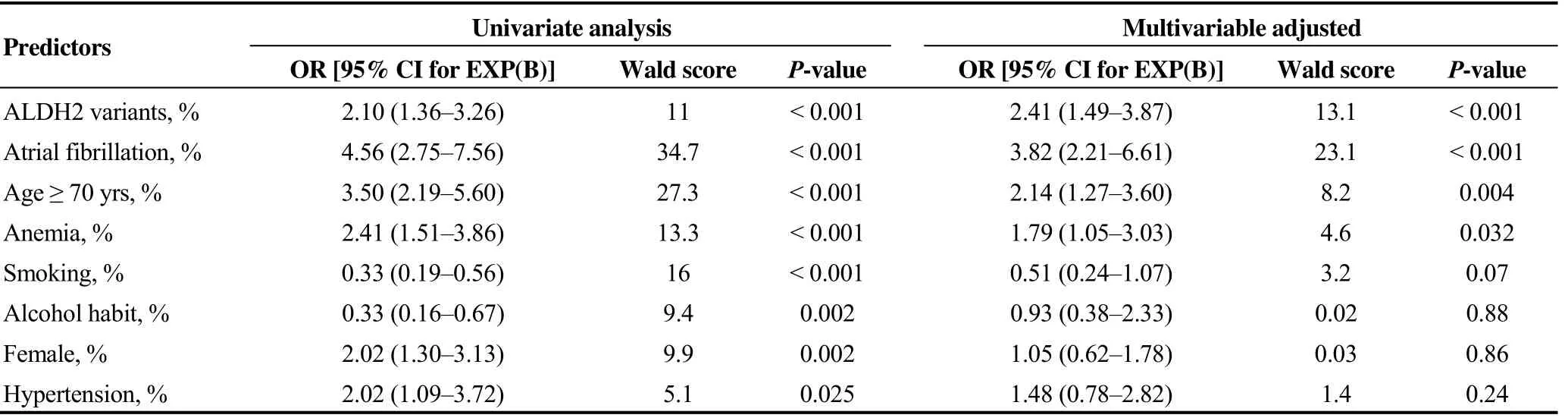
Table 4. Association of genetic and clinical traits with incident HFpEF.
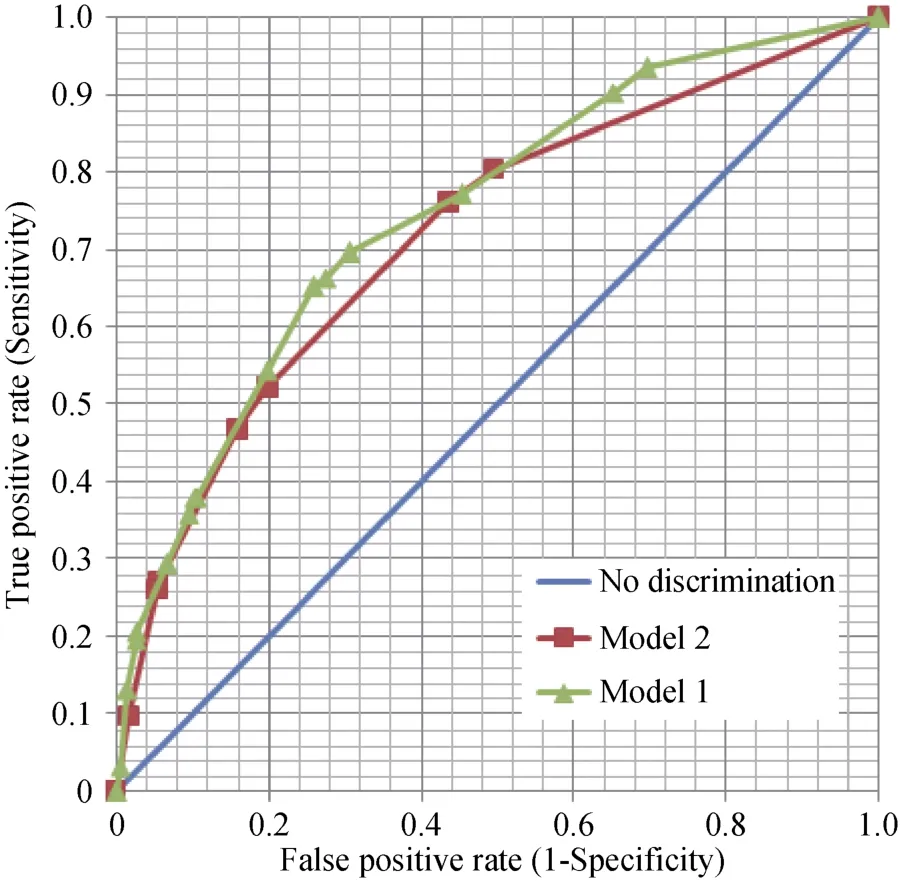
Figure 1. Comparison of the HFpEF incidence ROC areas using Model 1 and Model 2. The ROC area of Model 1 was significantly larger than the ROC area of Model 2 (0.745 vs. 0.719, Z = 1.98, P = 0.048), indicating that ALDH2*2 variants were independently associated with HFpEF incidence. ALDH2: aldehyde dehydrogenase 2; HFpEF: heart failure with preserved ejection fraction; ROC: receiver operating characteristics curve.
To test the robustness of the genetic and traditional risk factors in HFpEF prediction, we compared the receiver operating characteristic curve (ROC) areas between Model 2 (the prediction model with three traditional exposures) and Model 1 using theZtest. The area under the ROC curve for Model 2 was 0.719 (95% CI: 0.661-0.778,P< 0.001). The difference in the areas between Model 1 and Model 2 was 0.03 (95% CI: 0.001-0.05,Z= 1.98,P= 0.048), as shown in Figure 1.
4 Discussion
China has one-fifth of the world’s population, and it is estimated that China would become a moderate ageing country between 2019 and 2020 and a severe ageing country in 2030. Although HFpEF has become a rising social burden and one of the greatest unmet needs in the interdisciplinary fields of cardiology and gerontology, epidemiological studies of risk factors for HFpEF have been conducted mainly in Western countries. In this study, we found that (1) exposure toALDH2*2variants increases the risk of HFpEF even in the presence of clinical predictors; and (2) 4 A traits (ALDH2*2variants, age, atrial fibrillation and anaemia) were associated with incident HFpEF in Chinese CVD patients. To the best of our knowledge, this is the first report including a single nucleotide polymorphisms exposure in the analysis of risk factors for HFpEF in CVD patients.
Risk factors are a variety of exposures that increase susceptibility to diseases. They can be demographic (age, sex, ethnicity,etc.), environmental (lifestyle, professional exposure, air pollution,etc.), genetic or related-disease states (chronic infections, diabetes, hypertension,etc.). It has been demonstrated that older age, female sex, obesity and CVD are highly prevalent in patients with HFpEF,[16]however, in our study, traditional risk factors such as age, anaemia and atrial fibrillation were identified as risk factors for HFpEF. In Japanese HFpEF patients, anaemia has been implicated in poor prognosis.[17]Nearly one-third of HFpEF patients had atrial fibrillation, and atrial fibrillation was independently associated with all-cause mortality in HFpEF patients.[18,19]Similarly, in a multiethnic Southeast Asian Cohort, atrial fibrillation at baseline was a predictor of death or hospitalization in patients with HFpEF.[20]Since anaemia and atrial fibrillation are risk factors that can be modified by treatment, they might be considered therapeutic targets for HFpEF in clinical practice.
It was reported that the rs671 polymorphism in theALDH2gene was associated with the risk of coronary heart diseases,[21,22]hypertension,[23]stroke[24]and diabetes.[25]Nevertheless, none of these studies included theALDH2 rs671polymorphism together with clinical risk factors when exploring the association of these factors with diseases. In our study, we evaluatedALDH2*2variants with seven other risk factors for HFpEF occurrence. Our study sheds insight into the intriguing molecular mechanism underlyingALDH2*2variants in senescent hearts and might provide clues for individualized, targeted HFpEF therapies.
In our study, the association of coronary artery disease and diabetes with HFpEF was not found. The association of hypertension with HFpEF was underpowered in the presence of other risk factors. Although coronary artery disease, diabetes mellitus, and hypertension often coexist with HFpEF,[26]none of them represents a definite risk factor for HFpEF. For example, even though hypertension is a risk factor for HFpEF, it should not be deemed a risk factor for HFpEF, because treatment of risk factors should improve clinical condition, whereas treatment of hypertension fails to ameliorate the clinical outcome of HFpEF. The reason for the high prevalence of CVD in HFpEF patients is that these comorbidities are also related to ageing.
In obese patients, the increase in plasma volume causes a disproportionate increase in cardiac preload and left ventricular filling pressures.[27]Therefore, BMI, the most commonly used parameter of obesity, is proposed to increase the risk of HFpEF.[28]However, in our study, BMI was not significantly different between the HFpEF and non-HFpEF groups. It was implied that Asian HFpEF patients were relatively lean compared with those from Western populations.[29]Racial differences are likely to explain the disparities in BMI among different studies. Sex differences are suggested to contribute to the phenotypic heterogeneity of HFpEF.[30]Thymosin beta-4 is elevated in women with HFpEF.[31]In the TOPCAT trial, women and men had different clinical profiles and experienced different therapeutic effects of spironolactone.[32]Nevertheless, in our study, sex differences did not persist after adjusting for other risk factors. This might be explained by Chinese female patients with CVD adopting a healthier lifestyle, such as less smoking and alcohol consumption, than male patients.
Additionally, it has been suggested that renal dysfunction is a risk factor for HFpEF due to endothelial dysfunction and inflammation.[33]However, in our study, the impact of renal function on HFpEF incidence was not significant when considering age. In fact, renal dysfunction can influence the metabolism of circulating NT-proBNP, leading to HFpEF misdiagnosis.[34]To make the complex clinical background of HFpEF easier to explain, we excluded patients with severe renal dysfunction in this study.
The echocardiographic findings were very interesting in this study. In general, diastolic dysfunction frequently coexisted with systolic dysfunction in patients with HFpEF. Thus, the previous nomination of ‘diastolic heart failure’ was substituted by HFpEF for the type of heart failure with relatively normal systolic function. However, the systolic function in HFpEF patients was preserved only in contrast to that in the heart failure with reduced ejection fraction (HFrEF) subtype; it was indeed impaired when compared with the patients without HFpEF. Our data raise two questions regarding the current conception of HFpEF. The first is whether the cut-off values of the ejection fraction for HFpEF (≥ 50% or ≥ 45%) are optimal. Perhaps a new cut-off value of the ejection fraction should be adopted in future investigations. The second is, whether medications to accentuate heart contraction are appropriate for patients who have symptoms of heart failure because systolic function in HFpEF patients is actually decreased.
There are some limitations of our study. Firstly, exercise echocardiography and heart catheterization might provide more useful information than resting echocardiography in the diagnosis of HFpEF. Secondly, this was a single-centre prospective study, which might have been biased by the willingness of CVD patients to participate in this study. Therefore, the 4 A traits associated with HFpEF should be confirmed by multi-centre, large-scale studies in China. Regardless, with the rise of HFpEF incidence, the need to explore risk factors for HFpEF in the Chinese population is urgent. In this study, we confirmed the association betweenALDH2*2variants and HFpEF risk and proposed 4 A traits associated with HFpEF incidence in Chinese patients with CVD. Our study has important implications for the prevention and management of Chinese HFpEF patients.
Acknowledgments
This study was supported by the he National Natural Science Foundation of China (No. 81770441, No. 81700398, No. 81970309) and Nanjing Municipal Healthcare Grant YKK16127. All authors had no conflicts of interest to disclose.
 Journal of Geriatric Cardiology2019年12期
Journal of Geriatric Cardiology2019年12期
- Journal of Geriatric Cardiology的其它文章
- Quantitative flow ratio and intravascular ultrasound guided percutaneous coronary intervention of left anterior descending lesion concomitant with severe coronary myocardial bridge
- Delayed cardiac tamponade after simultaneous transcatheter atrial septal defect closure and left atrial appendage closure device implantation: a particular case report
- Coarctation of the aorta in twins with severe hypertension
- Pacemaker therapy in very elderly patients: survival and prognostic parameters of single center experience
- Irregular surface of carotid atherosclerotic plaque is associated with ischemic stroke: a magnetic resonance imaging study
- Hypoxia promotes pulmonary vascular remodeling via HIF-1α to regulate mitochondrial dynamics