
Bilateral vs unilateral placement of metal stents for inoperable highgrade hilar biliary strictures: A systemic review and meta-analysis
2019-09-25 08:12:42MunishAshatSumantAroraJagpalKlairChristopherChildsArvindMuraliFrederickJohlin
World Journal of Gastroenterology 2019年34期
Munish Ashat, Sumant Arora, Jagpal S Klair, Christopher A Childs, Arvind R Murali, Frederick C Johlin
Abstract BACKGROUND Bilateral vs unilateral biliary stenting is used for palliation in malignant biliary obstruction. No clear data is available to compare the efficacy and safety of bilateral biliary stenting over unilateral stenting.AIM To assess the efficacy and safety of bilateral vs unilateral biliary drainage in inoperable malignant hilar obstruction.METHODS PubMed, Embase, Scopus, and Cochrane databases, as well as secondary sources(bibliographic review of selected articles and major GI proceedings), were searched through January 2019. The primary outcome was the re-intervention rate. Secondary outcomes were a technical success, early and late complications,and stent malfunction rate. Pooled odds ratio (OR) and 95% confidence interval(CI) were calculated for each outcome.RESULTS A total of 9 studies were included (2 prospective Randomized Controlled Study,5 retrospective studies, and 2 abstracts), involving 782 patients with malignant hilar obstruction. Bilateral stenting had significantly lower re-intervention rate compared with unilateral drainage (OR = 0.59, 95%CI: 0.40-0.87, P = 0.009). There was no difference in the technical success rate (OR = 0.7, CI: 0.42-1.17, P = 0.17),early complication rate (OR = 1.56, CI: 0.31-7.75, P = 0.59), late complication rate(OR = 0.91, CI: 0.58-1.41, P = 0.56) and stent malfunction (OR = 0.69, CI: 0.42-1.12,P = 0.14) between bilateral and unilateral stenting for malignant hilar biliary strictures.CONCLUSION Bilateral biliary drainage had a lower re-intervention rate as compared to unilateral drainage for high grade inoperable malignant biliary strictures, with no significant difference in technical success, and early or late complication rates.
Key words: Metal stent; Hilar biliary stricture; Re-intervention rate; Technical success rate
INTRODUCTION
Unresectable malignant hilar obstruction (UMHO) is associated with very poor prognosis. Five-year survival is < 10% with most patients dying within 1 year of diagnosis[1,2]. Compared to plastic stents, self-expanding metallic stents (SEMS) have shown to be more cost effective and provides advantage with longer stent patency and less re-intervention rate in patients with non-operable malignancy with score of II to IV on Bismuth-Corlette classification and Hilar cholangiocarcinoma who have a predicted the life expectancy of > 3 mo[3-5]. Biliary stenting also plays a role in the management of obstructive jaundice and cholangitis and is important in enhancing the quality of life of patients with UMHO.
Although endoscopic stenting is widely favored in cases of UMHO, there is currently no consensus on whether the placement of bilateral biliary stents has any advantage for these patients over unilateral stenting. Although some experts believe in measuring the volume of the liver to be drained to determine the type of stent to be used, quantification of the liver volume is clinically challenging. Furthermore, there have been conflicting data regarding the technical success and outcomes of bilateral and unilateral stenting. While some authors believe that unilateral stenting renders increased technical success rate with concomitant lower complications[6-8]; bilateral stenting, on the other hand, will drain higher liver volume, may have longer stent patency, and hence may require less re-intervention[9-11].
The aim of the meta-analysis was to systematically review the current literature and compare the efficacy of unilateralvsbilateral stenting in achieving successful stent placement, comparing re-intervention rate, technical success, and early and late procedure-related complications for unresectable malignant hilar strictures.
MATERIALS AND METHODS
Data sources and searches
Search strategies were developed with the assistance of a health sciences librarian with expertise in searching for systematic reviews. Comprehensive search strategies using index and keywords were constructed for PubMed, Embase (Elsevier), and Cinhal (EBSCO). No database filters were used at any time during the searching process. All searches were conducted during January 2019 and the number of citations found in each database can be found in the flow diagram (Figure 1). The searches combined the following concepts: Unilateral SEMS and bilateral SEMS with biliary stents. Within the results for those combined concepts, additional filters, publication types, and keyword strategies were used to identify and exclude the most common articles types that do not report trial results (reviews and case studies). An exhaustive forward search tool was used for the Web of Science database to capture all possible studies of interest. The databases were searched for publications dates 1995 to present.Language limits were applied to search for articles in English only. To identify further articles, references were hand searched. All results were downloaded into EndNote(Thompson ISI Research Soft, Philadelphia, PA, United States), a bibliographic database manager, and duplicate citations were identified and removed. In addition,abstracts from Digestive Disease Week, annual meetings of American College of Gastroenterology, and United European Gastroenterology Week from the last 5 years were also searched.
Inclusion criteria
Prospective studies, retrospective studies, and abstracts published in the English language were included if they compared unilateralvsbilateral SEMS biliary stent placement, for one or more of the clinical outcomes: Re-intervention rate, technical success, complication rate, and stent malfunction.
Exclusion criteria
Studies were excluded when there was no comparison between unilateral and bilateral stents. We also excluded studies that did not evaluate the required predefined endpoints. Furthermore, duplicate studies, case reports, animal studies, and letters to editors were excluded.
Data extraction
Two authors (Ashat M and Arora S) independently extracted the data according to a pre-specified protocol from all the included studies. All discrepancies were resolved after discussion with a third reviewer.
Quality assessment and risk of bias
Cohort studies were assessed using the Newcastle-Ottawa Scale and for randomized control trials, Cochrane tool was used to assess for risk of bias[12,13]. Risk of publication bias for each end-point was assessed using the funnel plots.
Outcome
The data collected from eligible studies included following data points-publication year, authors, country of publication, study design, mean age of study participants, a total number of patients in each unilateral stenting and bilateral stenting category and type of malignancy, complications rates, and type of complications Supplemental(Table 1).
Primary end-point of the study was the re-intervention rate. This was defined as an endoscopic or percutaneous intervention that was done for stent failure and to increase biliary drainage or for recurrent jaundice, or for management of dilated intrahepatic bile duct revealed by imaging or management of immediate adverse event of successfully inserted SEMS. Secondary outcomes were (1) Technical success was defined by the successful placement of bilateral or unilateral SEMS across stricture site, confirmed by the flow of contrast or bile through SEMS; (2) Early adverse event rate- defined as early stent-related complications within 4 wk. Early complications included cholangitis, cholecystitis, pancreatitis, bleeding, and liver abscess; (3) Late adverse events were defined as any stent-related complication that occurred after 4 wk of stent insertion. Late complication included cholangitis, cholecystitis, liver abscess; and (4) Stent malfunction defined as stent obstruction due to sludge or stone formation, cholangitis, tumor in-growth, or development of a liver abscess, or biloma.
Statistical analysis
Review Manager 5.3 (The Cochrane Collaboration, Oxford, United Kingdom) was used to analyze the data for the meta-analysis. Pooled odds ratios (ORs) and 95%confidence interval (CI) of study end-points were calculated using the Mantel-Haenszel method. In order to access of heterogeneity, we usedX2test (Cochran Q statistic). In case there was significant heterogeneity, a random-effect model was used.Funnel plots were obtained to assess the risk of bias.
RESULTS
Using pre-defined parameters and removing duplicate publications our search strategy identified 281 articles. Another 2 articles were identified by manual search. A total of 262 articles were excluded based on our exclusion criterion. Based on our inclusion criterions, 9 studies were selected (Figure 1). Of these 9 studies, 7 were published manuscripts and 2 were published as abstracts. All the baseline characteristics of each individual studies are highlighted in Supplemental Table 1.
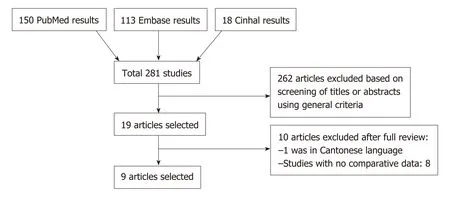
Figure 1 PRISMA diagram of the literature search.
Study characteristics
The characteristics of the studies, and of the patients in the selected studies are shown in Supplemental Table 1. A total of 9 studies were enrolled in the current study of which 2 were randomized control trial’s (RCT), and 7 were retrospective trials (5 complete manuscripts and 2 abstracts). Although the study by Mukaiet al[14]was an RCT, for our analysis we used only bilateral stents subgroup of the study which was not randomized. A total of 782 patients were included in the analysis of bilateralvsunilateral biliary stenting.
Results of meta-analysis
Primary end-point:Re-intervention rate: A total of 7 studies involving 513 patients was included in this analysis[7,10,14-18]. Bilateral stenting required significantly lower reintervention as compared to unilateral stenting (OR = 0.59, 95%CI: 0.40-0.87,P=0.009) (Figure 2). The funnel plot showed no asymmetry (Figure 3).
Secondary end-points:(1) Technical success: A total of 8 studies involving 745 patients was included in this analysis[7,10,14,15,17-20]. There was no significant difference in the technical success rate with bilateral stenting as compared to unilateral stenting(OR = 0.7, 95%CI: 0.42-1.17,P= 0.17) (Figure 4). There was mild heterogeneity; (2)Early complications: A total of 5 studies involving 530 patients were included in this analysis[7,10,18-20]. There was no difference between early complications (OR = 1.56,95%CI: 0.31-7.75,P= 0.0001) (Figure 5); (3) Late complications: A total of 5 studies involving 430 patients were included in this analysis[7,10,15,18,20]. There was no difference in late complication rate (OR = 0.91, 95%CI: 0.58-1.41,P= 0.56) (Figure 6); and (4)Stent malfunction: A total of 4 studies involving 324 patients was included in this analysis[7,10,15,18]. There was no difference in stent malfunction rates (OR = 0.69, 95%CI:0.42-1.12,P= 0.14) (Figure 7).
Quality assessment and funnel plots
The Newcastle Ottawa Scale score has been provided for all retrospective studies in Supplemental Table 1. The Cochrane collaboration tool assessment of bias for the RCT has been provided in Figure 8. Funnel plots to estimate bias revealed no asymmetry(Figure 3).
DISCUSSION
Endoscopic biliary drainage is the intervention of choice in patients with UMHO.Besides providing symptomatic relief to patients with pruritis it also has therapeutic implications with a reduction in total bilirubin which permits the use of subsequent chemotherapy, radiotherapy or photodynamic therapy. This may be important in prolonging the life of patients with unresectable malignant biliary strictures. Over the past decade, multiple studies have found using metallic stents over plastic stents as more cost-effective in hilar cholangiocarcinoma[4,14,21,22]. However, the data comparing bilateralvsunilateral stenting in UMHO is sparse. There has been conflicting data in regards to the outcomes of placement of bilateralvsunilateral SEMS stents[7,8,10,18,23,24].Therefore, we designed this meta-analysis to review the data, thus-far available,comparing bilateralvsunilateral SEMS placement for UMHO. Our meta-analysis shows that bilateral stenting as compared to unilateral stenting is associated with a lower re-intervention rate, but has a comparable technical success rate, early and late complication rates.
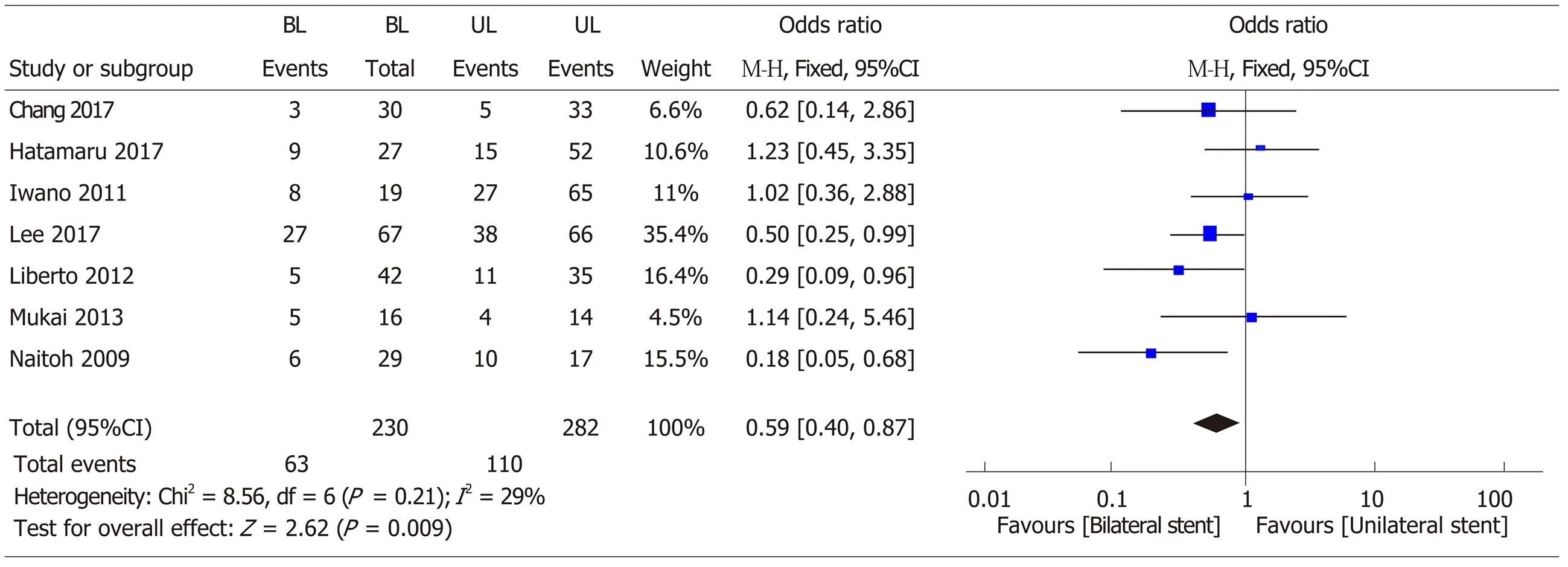
Figure 2 Forest plot of re-intervention rates with bilateral self expanding metal stents vs unilateral stent. SEMS: Self expanding metal stents; OR: Odds ratio;CI: Confidence interval.
Bilateral stenting was associated with a statistically significant 41% reduction in reintervention rate. There has been marked variability in results among published literature. A prospective trial by Mukaiet al[14]demonstrated 50% re-intervention rate in bilateral SEMS group compared to 29% in unilateral SEMS group. However, the study groups were not treated similarly in their study, as patients who received bilateral stent received sphincterotomy while patients receiving unilateral stent did not. In the prospective RCT by Leeet al[10], the authors showed a statistically significant lower re-intervention rate at 3 mo for bilateral SEMS groupvsunilateral SEMS group (10.9%vs33.3%). The ability to reduce the number of interventions is of paramount importance in patients with non-operable malignant hilar strictures and an average life expectancy < 12 mo, thus avoiding multiple hospitalizations, which inreturn could mean an overall more cost-effective approach and also will have an impact on improving the quality of life for patients[18,25]. Further, restoration of bile flow with bilateral stenting is physiologically more superior to unilateral stenting.Approximately 25%-30% liver needs to be drained in order to satisfactorily reduce jaundice[8,26]. Though unilateral stent should be able to drain at-least 25% of the liver,clinical evidence suggests that up to 30% cases of hilar cholangiocarcinoma are associated with hepatic lobar atrophy[27], and thus in such a situation, unilateral stenting may not provide an appropriate therapeutic response and may increase primary re-intervention rates. Furthermore, a study by Vienneet al[28]suggested that draining more than 50% of the liver volume is an important predictor of the effectiveness of biliary drainage especially in malignant hilar strictures.
The conflicting data is further complicated by the technical difficulties associated with the placement of bilateral stents. Thus, multiple newer stent delivery systems have been developed to overcome this technical challenge. In our study, there was no significant difference in the technical success between bilateral biliary stenting and unilateral biliary stenting. A meta-analysis by Hong Wet al[24]concluded higher success with unilateral stenting. However, their meta-analysis included studies involving plastic biliary stents which may have affected the results. Our results are similar to results by Naitohet al[18]and Iwanoet al[7]who had similar technical success for bilateral and unilateral stents. Bilateral stents could be placed by either stent-instent technique (SIS) or side-by-side technique (SBS). Naitohet aluse stent in stent technique and Iwanoet alused SIS technique respectively in their patients Although,this meta-analysis did not specifically compare the two techniques of bilateral stenting, a meta-analysis by Naitohet al[18]showed longer stent patency time with SBS group when compared to SIS group. Provider expertise could also account for the variability in the technical success rate among the studies. Thus, based on our results,we believe that bilateral stenting may be preferable for providers who are technically adept at placing both bilateral and unilateral stent.
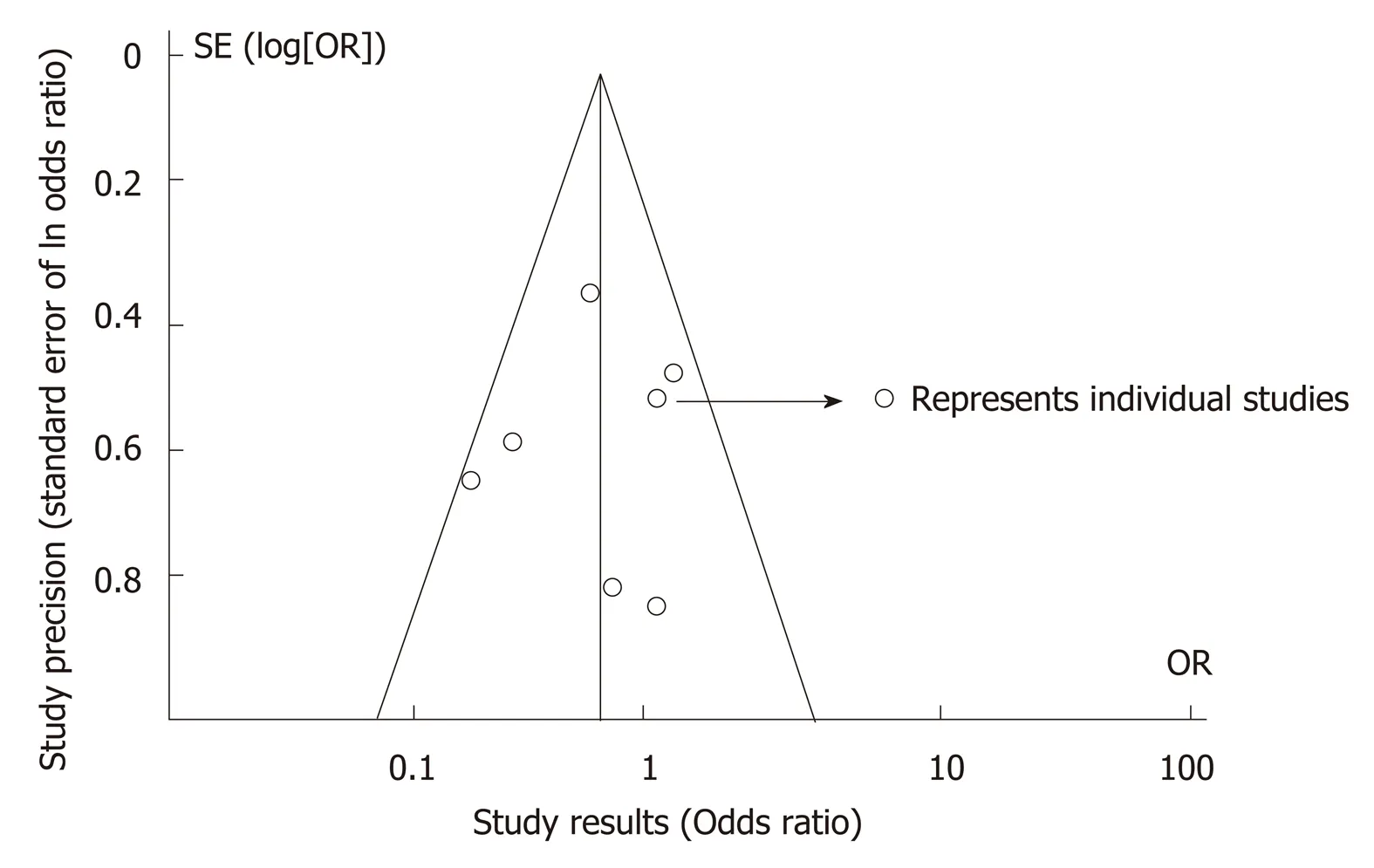
Figure 3 Cochrane collaboration tool. Risk assessment.
Stent malfunction could be driving our primary outcome of stent re-intervention rates. The rate of reintervention was influenced by stent malfunction, however, not all studies defined the cause of stent malfunction clearly (Supplemental Table 2) and hence we only included stent malfunction as a secondary outcome. There was a trend towards decreased stent malfunction with bilateral drainage as compared to unilateral drainage though this was not statistically different. Earlier studies seemed to suggest that bilateral stents could lead to increased stent-related early complications. SBS was associated with increased cholangitis rates and portal vein occlusion because of excessive expansion of the bile duct by parallel stents[18]. SIS deployment could lead to increased sludge formation at the site of stent overlap as a result of a reduction in bile inflow and increase the incidence of tumor ingrowth if the stent mesh is expanded in the area of overlap[17]. In contrast, most recent RCT by Leeet al[10]has shown no difference in rates of cholangitis and liver abscess after bilateral stent placement.Similarly, in our meta-analysis, there was no difference with stent-related early or late complication rates between the two groups.
There are several limitations to this meta-analysis. The main limitation is that only two studies included in our meta-analysis are RCT’s. Most studies are retrospective studies which could have led to selection bias. Nevertheless, the retrospective studies are reasonable quality cohort studies, as determined by the Modified Newcastle Ottawa quality assessment scale of cohort studies. Another limitation is the presence of significant heterogeneity in some of the analysis. This is likely due to the significant clinical heterogeneity among the studies the differences in the study population, the location of malignant strictures, technical expertise of the providers, and the difference in the duration. However, importantly, there was only mild heterogeneity in the analysis of our primary end-point analysis of re-intervention rate and in the analysis for technical success. For analysis with significant heterogeneity, we used a random effects model to partly account for the clinical heterogeneity. This highlights the need for further research on this topic and the importance of our meta-analysis based on available data.
In conclusion, bilateral biliary stenting for UMHO may decrease the re-intervention rate in patients with malignant hilar strictures, without increasing early or late complication rate. To the best of our knowledge, this is the first meta-analysis so far comparing the outcomes of SEMS bilateralvsunilateral stenting. Further RCT’s are needed to confirm our findings.
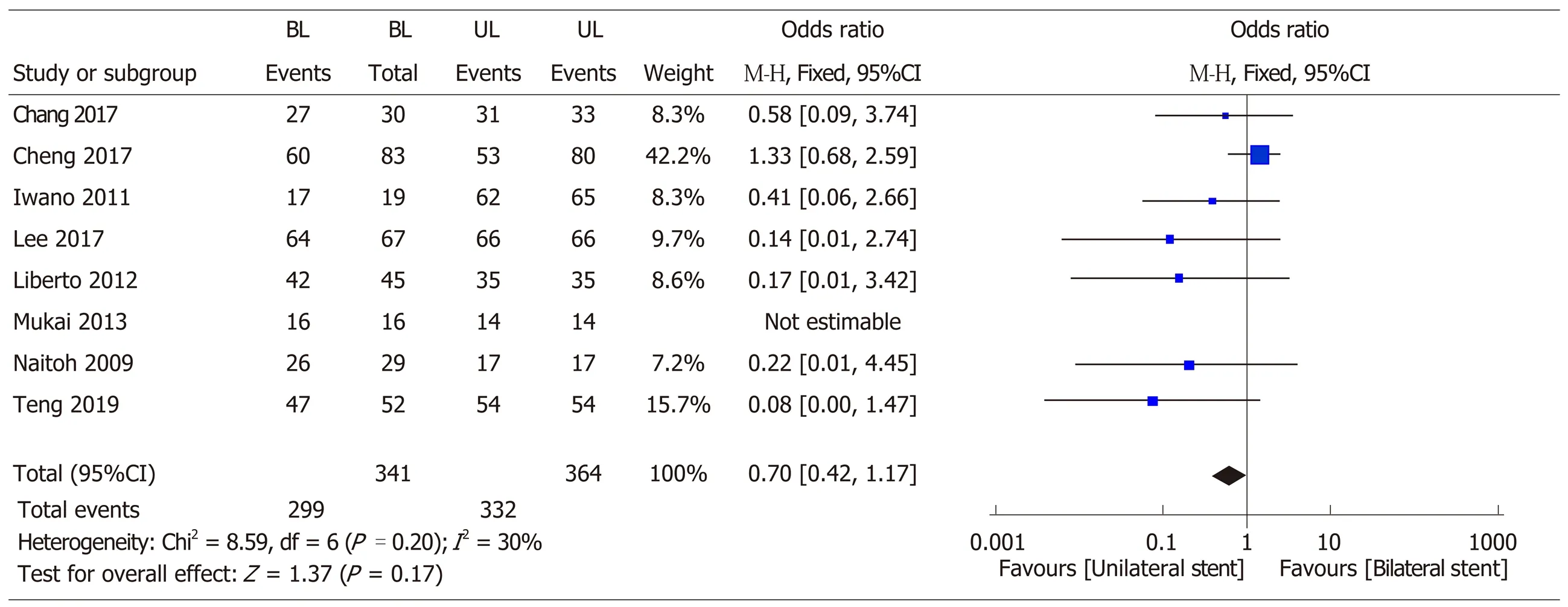
Figure 4 Forest plot of technical success rates with bilateral self expanding metal stents vs unilateral stent. SEMS: Self expanding metal stents; OR: Odds ratio; CI: Confidence interval.
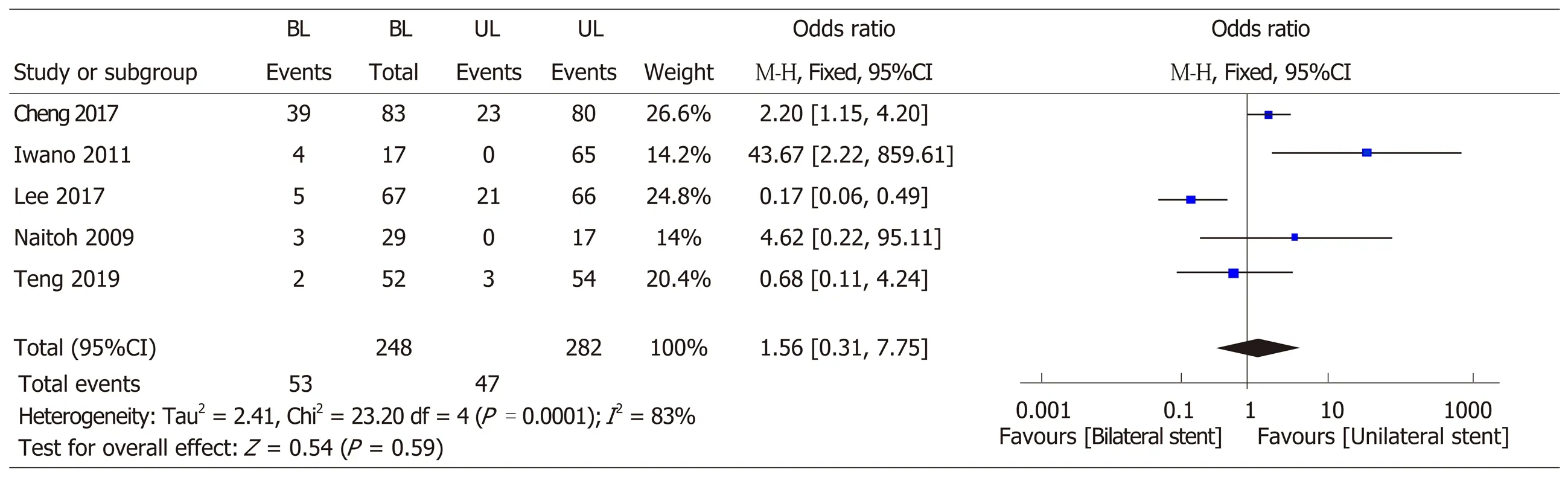
Figure 5 Forest plot of early complication rates with bilateral self expanding metal stents vs unilateral stent. SEMS: Self expanding metal stents; OR: Odds ratio; CI: Confidence interval.
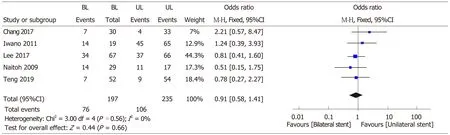
Figure 6 Forest plot of late complication rates with bilateral self expanding metal stents vs unilateral stent. SEMS: Self expanding metal stents; OR: Odds ratio; CI: Confidence interval.
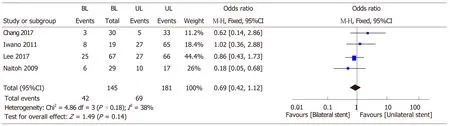
Figure 7 Forest plot of stent malfunction rates with bilateral self expanding metal stents vs unilateral stent. SEMS: Self expanding metal stents; OR: Odds ratio; CI: Confidence interval.
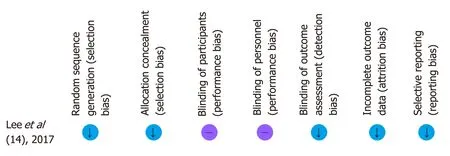
Figure 8 Risk of bias summary: Review authors' judgements about each risk of bias item for each included study.
ARTICLE HIGHLIGHTS
Research background
The background, present status, and significance of the study should be described in detail.
Research motivation
Over the past few years, newer randomized control trials (RCTs have been published showing the overall advantage of bilateral biliary stenting over unilateral stenting in a subset of patients with inoperable hilar malignant strictures. No meta-analysis was done on this topic with newer study data points.
Research objectives
We aimed to conduct a meta-analysis to compare the role of bilateral stentingvsunilateral stenting in inoperable malignant hilar strictures.
Research methods
A detailed literature search was conducted to find all the relevant articles. Two reviewers independently analyzed all the selected studies. All discrepancies were discussed independently with the third reviewer and consensus was achieved. We used Pooled odds ratio (OR) and 95%confidence intervals (CIs) were calculated for each outcome.
Research results
A total of 782 patients form nine studies were included for analysis. Bilateral stenting had significantly lower re-intervention rate compared with unilateral drainage (OR = 0.59, 95%CI:0.40-0.87, P = 0.009). There was no difference in the technical success rate (OR = 0.7, CI: 0.42-1.17,P = 0.17), early complication rate (OR = 1.56, CI: 0.31-7.75,P= 0.59), late complication rate (OR =0.91, CI: 0.58-1.41, P = 0.56) and stent malfunction (OR = 0.69, CI: 0.42-1.12,P= 0.14) between bilateral and unilateral stenting for malignant hilar biliary strictures.
Research conclusions
Older studies that have shown the ease of putting unilateral stenting with fewer complications over bilateral stenting in inoperable malignant hilar strictures. However, with new RCTs showing the higher success of bilateral biliary stenting with lower re-intervention rates, bilateral stenting could offer an overall advantage over unilateral stenting. Our study highlights the overall advantage of bilateral stenting over unilateral stenting.
Research perspectives
Biliary stenting is very important modality in the overall management of inoperable malignant hilar strictures. Bilateral stenting offers an advantage over unilateral stenting, however more RCT is required to further support this conclusion.
 World Journal of Gastroenterology2019年34期
World Journal of Gastroenterology2019年34期
- World Journal of Gastroenterology的其它文章
- Reducing anastomotic leak in colorectal surgery: The old dogmas and the new challenges
- Analysis of 72 patients with colorectal high-grade neuroendocrine neoplasms from three Chinese hospitals
- Overlay of a sponge soaked with ropivacaine and multisite infiltration analgesia result in faster recovery after laparoscopic hepatectomy
- Risk factors for Mallory-Weiss Tear during endoscopic submucosal dissection of superficial esophageal neoplasms
- Timing, distribution, and microbiology of infectious complications after necrotizing pancreatitis
- Association of XPG rs2094258 polymorphism with gastric cancer prognosis