
Correlation between invasive microbiota in margin-surrounding mucosa and anastomotic healing in patients with colorectal cancer
2019-09-19 06:45:30YanDongLiKangXinHeWeiFangZhu
Yan-Dong Li,Kang-Xin He,Wei-Fang Zhu
Abstract
Key words: Intestinal microbiota;16s rRNA gene sequencing;Anastomotic healing;Predictive ability;Colorectal cancer;Radical resection
INTRODUCTION
Colorectal cancer (CRC) is one of the most frequently diagnosed cancers worldwide[1-3].Impaired anastomotic healing is defined as a breach in a surgical join between two hollow viscera,with a leak of luminal contents that may emerge either through the wound or at the drain site,or near the anastomoses[4].As one of the major complications after radical resection for CRC,impaired anastomotic healing may significantly increase hospital costs and prolong the length of hospital stay,and is also linked to cancer recurrence,metastasis,or even tumor-related death[5-11].Clinical symptoms of impaired anastomotic healing often include abdominal pain/distension with fever,pus or fecal excretion,pelvic abscess,peritonitis,and even septic shock[12,13].The International Study Group of Rectal Cancer[13]proposes the following system grading the severity of impaired anastomotic healing:A,no therapeutic intervention;B,active intervention is required but no re-laparotomy;and C,relaparotomy is required.Impaired anastomotic healing rate has been found to vary from 1% to 19% depending on the anatomic location of the anastomosis[9,14-17].Many risk factors have been identified to be associated with impaired anastomotic healing[10,18-20],for instance,a systematic review study[18]suggests that the main preoperative risk factors,which predict impaired anastomotic healing,are sex,age,tumor distal site,tumor size,advanced stage,renal disease,co-morbidity,and history of radiotherapy.Besides,blood loss/transfusion,duration of surgery,rectal contrast by computed tomography (CT),and C-reactive protein (CRP) level are considered as intraoperative risk factors or postoperative factors.The treatment strategies for impaired anastomotic healing after rectal cancer surgery can be divided into three stages according to the disease course as follows:Treatment strategies for the early stage (peritonitis stage,localized intra-abdominal abscess stage,and early stage fistula formation) mainly include identifying the necessity and opportunity of surgery,establishing patency drainage,controlling infection,correcting electrolyte and acidbase imbalance,and providing nutritional support;in addition to the above measures,treatment strategies for the middle stage (fistula formation stage) include fistula management and closure treatment;in the later stage,deterministic remedial surgery is performed for unrecovered patients[13].In terms of severity of specific symptoms,patients were treated either by systemic nutrition support,antibiotics,percutaneous drainage,and transanal revision or by re-laparotomy.Notably,antibiotic treatment should be implemented against Gram-negative bacteria and Gram-positive bacteria,and special attention is required for the anaerobic bacteria[21].
In most cases,the clinical symptoms of impaired anastomotic healing remain insidious,vague,and uncharacteristic,which are typically not recognized until postoperative days 5-8,sometimes even until postoperative day 12[15,22].If not appropriately treated in time,impaired anastomotic healing in patients could easily evolve into severe postoperative complications and therefore affects morbidity,mortality,and functional and oncological outcomes[5-8].Thus,early diagnosis and prediction of impaired anastomotic healing are of great significance.A pilot study suggests that combined changes of interleukin (IL)-4,IL-6,and IL-10 could accurately predict impaired healing of anastomoses[23].Another study conducted on postoperative CRP in elective abdominal surgery shows that impaired anastomotic healing is unlikely to occur in patients with CRP < 135 mg/L on postoperative day 3[24].Daamset al[25]carried out a study,in which peritoneal lactate concentration was continuously monitored by peritoneal microdialysis to characterize the ischemia and inflammation around the anastomosis,and they found a significant change of peritoneal lactate concentration in patients with impaired anastomotic healing.The results suggest that peritoneal microdialysis is predictive of impaired anastomotic healing after colorectal surgery[25-27].However,these results need to be further confirmed by clinical trials.Intestinal microbes were first reported to be associated with impaired anastomotic healing over 60 years ago[28].It is shown that directly using antibiotics on anastomotic tissues could promote the healing process and prevent leak in dogs undergoing colon resection and anastomosis.Recently,the mechanism has been confirmed to be linked to the direct effect of bacterial collagenases[12,29].Pseudomonas aeruginosa,Serratia marcescens,andEnterococcus faecalis,which can express a collagenolytic phenotype,are reported to be associated with the impaired anastomotic healing[30-34].Besides,Shoganet al[12]proved thatEnterococcus faecalisis involved in the pathogenesis of impaired anastomotic healing by enhancing collagendegrading activity and activating intestinal tissue matrix metalloproteinase 9 (MMP9).Preliminary evidence suggests that intestinal microbiota contributes to the occurrence and development of impaired anastomotic healing.Thus,it could be used as a potential predictor[12,20,29-34].Recently,researchers reported the role of intestinal microbiota in the development of impaired anastomotic healing in the “donuts’’,in which a stapled colorectal anastomosis was made.Their results showed that a high abundance ofLachnospiraceaeandBacteroidaceaeis strongly related to the impaired anastomotic healing,and the bacterial composition that consisted of 60% or more of these two families might be predictive of impaired anastomotic healing[35,36].It can be seen that intestinal microbiota is emerging as a potential predictive factor for anastomotic healing.Nonetheless,it still lacks extensive clinical data and strong statistical evidence on the effect of intestinal microbiota on postoperative anastomotic healing.In this study,margin-surrounding mucosa samples derived from seven CRC patients with impaired anastomotic healing and 30 well-healed CRC patients were collected and the bacterial community was characterized by using 16s rRNA gene sequencing,with an aim to identify the specific bacteria related to the impaired anastomotic healing and to evaluate the ability of the selected taxa in predicting the healing status of anastomoses.
MATERIALS AND METHODS
Participant recruitment and sample collection
Thirty-seven patients with primary CRC who received surgical treatment from January 2017 to December 2018 at the First Affiliated Hospital,Zhejiang University School of Medicine were recruited to the study,and informed consent was obtained from all participants.The exclusion criteria for all participants were as follows:(1)Aged above 90 years old;(2) History of using antibiotics (excluding prophylactic antibiotic usage through intravenous infusion during the preoperative period) within two months;and (3) History of receiving chemotherapy or radiation treatments prior to the study,or personal history of chronic bowel disorders or metabolic diseases such as cirrhosis and diabetes.Specimens of mucosa tissues adjacent to surgical margin derived from the participants were collected,immediately frozen in liquid nitrogen,and then stored at -80 °C for future DNA extraction and 16s rRNA gene sequencing.The study protocol was approved by the Medical Ethics Committee of the First Affiliated Hospital,Zhejiang University School of Medicine.
Anastomotic leak evaluation and confounders
Clinical manifestations of impaired anastomotic healing after rectal cancer surgery are diverse but could be roughly divided into two categories according to whether the clinical manifestations are typical[13,22]:(1) Typical manifestations:fever,which is defined as decline or rise of body temperature or persistent high fever during postoperative day 3-5;signs of rectal stimulation and acute diffuse peritonitis;increased pelvic drainage and changes in characteristics (i.e.,drainage of gas,mucilage,or feces);leak detected by digital rectal examination;severe paralytic intestinal obstruction and infectious shock;elevated levels of white blood cells,neutrophils,and CRP detected by laboratory examination;impaired anastomotic healing and surrounding fluid found by CT and magnetic resonance imaging examination through the anus or abdominal drainage tube angiography;and impaired anastomotic healing found on colonoscopy;and (2) Atypical manifestations:irregularly low or medium fever,frequent bowel movements,tenesmus,and gradually appearing local peritonitis and (or) paralytic intestinal obstruction in the hypogastria,showing flocculent matter by pelvic drainage.In this study,the impaired healing of anastomoses was defined according to the following clinical manifestations in patients who received radical resection for CRC:Abdominal or pelvic pain,fever (>37.5 °C),discharge of feces,pus,or gas from pelvic drain,and discharge of pus from the rectum[13].It should be noted that fever was not considered as impaired anastomotic healing in this study,as it is difficult to distinguish the clinical symptoms between postoperative infections from impaired anastomotic healing[15].However,fever with abnormal drainage fluid (purulent,fecal,and long-term non-reduction) or with intestinal and abdominal abnormalities (such as abdominal pain without farting for a long time) was considered as impaired anastomotic healing.
According to the above indexes,the 37 patients were divided into two groups,namely,well-healing group (n= 30) and impaired-healing group (n= 7).The clinical characteristics (including age,sex,body mass index,tumor location,tumor size,TNM stage,tumor morphology,differentiation degree,intestinal obstruction,transfusion,blood loss,operation time,CRP,hemoglobin,and albumin) of the patients were recorded.
DNA extraction and characterization of bacterial community structure
Total DNA from the mucosa tissue samples was extracted using SDS/CTAB method.The purity and concentration of DNA were monitored on 1% agar gels (Thermo Fisher Scientific,Waltham,United States).The DNA sample was diluted into 1 ng/μL with sterile water and amplified using primers targeting the V4 region of the 16s rRNA gene (515F:5’-GTGCCAGCMGCCGCGGTAA-3’ and 806R:5’-GGACTACHVGGGTWTCTAAT-3’)[37].Cycling conditions included preheating at 98°C for 1 min,followed by 30 cycles of denaturation at 98 °C for 10 s,annealing at 50 °C for 30 s,elongation at 72 °C for 30 s,and final heating at 72 °C for 5 min.
PCR products were cleaned up using a GeneJETTM Gel Extraction Kit (Thermo Fisher Scientific,Waltham,United States).Sequencing libraries were constructed using an Ion Plus Fragment Library Kit (Thermo Fisher Scientific,Waltham,United States) following the manufacturer's instructions.The library quality was assessed on the Qubit@ 2.0 Fluorometer (Thermo Fisher Scientific,Waltham,United States).Finally,the library was sequenced on an Ion S5TM XL platform (Thermo Fisher Scientific,Waltham,United States).
Single-end reads were assigned to samples according to their unique barcodes and truncated by cutting off the barcodes from primer sequences.Qualities filtering on the raw reads were performed under specific filtering conditions to obtain the highquality clean reads according to the Cut adapt quality controlled process (v1.9.1).The reads were compared with the Silva database (version 123) to detect the chimera sequences using UCHIME algorithm[38],and the chimera sequences were then removed to obtain the final clean reads[39].
Sequences analysis was performed with Uparse software (v7.0.1001).Sequences with a similarity ≥ 97% were assigned to the same OTUs.Representative sequence for each OTU was screened.The Silva database (version 123)[40]was used based on the MOTHUR algorithm to annotate taxonomic information.In order to study the differences of the dominant species in different samples (groups),multiple sequence alignment was conducted using the MUSCLE software (version 3.8.31).OTUs abundance information was normalized using a standard of sequence number corresponding to the sample with the least sequences.Subsequent analyses of alpha diversity and beta diversity were all performed based on this output normalized sequencing data.Alpha and beta diversity analyses were calculated with QIIME software (version 1.7.0) and demonstrated with R software (version 2.15.3).
Statistical analysis
Statistical calculations were performed using SPSS (version 19.0).Wilcoxon test and chi-squared test were employed to analyze the correlation between the intestinal microbiota and anastomotic healing.The ability to discriminate impaired-healing and well healing was evaluated using the area under the receiver operator characteristic(ROC) curve (AUC).AP-value < 0.05 was considered statistically significant.
RESULTS
Characteristics of patients in well-healing and impaired-healing groups
A total of 37 CRC patients (age 67.97 ± 12.27 years old,51.35% of males) were included in this study,and seven (18.9%) patients developed impaired anastomotic healing.Although it seemed to be a high rate of patients with impaired anastomotic healing,this is mainly because the method we adopted was more sensitive in order to ensure the minimum loss of impaired healing cases.The clinical characteristics of the patients are presented in Table 1.The patients were significantly older in the impaired-healing group (P< 0.05),and most of the tumors were found in the right colon (57.1%),while tumors located in the left colon and rectum were more commonly found in the well-healing group (36.7% and 46.7%,respectively).Patients in the impaired-healing group largely had stages I and III CRC (42.9% and 42.9%,respectively),while those in the well-healing group mainly had stage II CRC (50%).The differentiation degree concentrated in the moderate degree and mainly polyp adenocarcinoma and ulcerative adenocarcinoma were diagnosed in both groups.Intestinal obstruction occurred in two (28.6%) patients in the impaired-healing group and three (10%) patients in the well-healing group.Besides,no significant differences in operative time,blood loss,transfusion,CRP level,hemoglobin level,or albumin level were identified in the two groups.
Community structure shifts and correlation of intestinal microbiota with anastomotic healing
The structure shifts of microbiota in mucosa tissue were analyzed by 16s rRNA gene sequencing.A total of 4527 OTUs in all samples were identified,of which 1874 were common in the two groups.Besides,the results found 2293 unique OTUs in the wellhealing group and 360 unique OTUs in the impaired healing group (Figure 1A).Rarefaction curve and species accumulation boxplot are shown in Figure 1B and C.The value of Good’s coverage for each group was higher than 99.6%.Alpha diversity analysis was conducted to examine the estimators of community richness,diversity,and evenness by observed species index,Shannon index,Simpson index,Chao1 index,Goods coverage index,and PD whole tree index between the two groups(Figure 1D),however,no significant difference was detected.For beta diversity analysis,microbial community and composition were analyzed by using weighted UniFrac distance matrix for each group,and a significant difference was found between the two groups (Figure 1E,P< 0.01),suggesting that the community compositions of the two groups were different.LEfSe analysis showed thatPorphyromonasgenus andPorphyromonadaceaefamily were highly abundant in the impaired healing group (Figure 1E).Ten highest dominant phyla of the two groups are shown in Figure 1F.The dominant phyla of the impaired-healing group wereProteobacteria(33%),Bacteroidetes(25%),andFirmicutes(17%),which were same as those in the well-healing group (31%,24%,and 21%,respectively).Figure 1G displays the ten highest dominant genera of the two groups.The dominant genera of the impaired-healing group wereIgnatzschineria(11%),Acinetobacter(11%),andBacteroides(11%),whileBacteroides(14%),Stenotrophomonas(9%),andIgnatzschineria(8%) were the dominant genera in the well-healing group.
To determine the association between the intestinal microbiota and anastomotic healing,Wilcoxon test was performed to analyze the abundance of bacteria species and genera in the two groups.Species and genera with significantly different abundances between the two groups are shown in Table S1 (P< 0.05).Thirty-three species and forty-five genera were found to be associated with the healing of anastomoses.Besides,six species (Alistipes shahii,Dialister pneumosintes,Corynebacterium suicordis,Porphyromonas asaccharolytica,Vibrio diazotrophicus,andClostridium leptum) had a difference of carrier rate > 40%.As shown in Figure 2,Alistipes shahiiandDialister pneumosinteswere significantly enriched in the well-healing group (P< 0.05).However,the high abundance ofCorynebacterium suicordis,Porphyromonas asaccharolytica,Vibrio diazotrophicus,andClostridium leptumwas significantly correlated with the impaired anastomotic healing (P< 0.05).
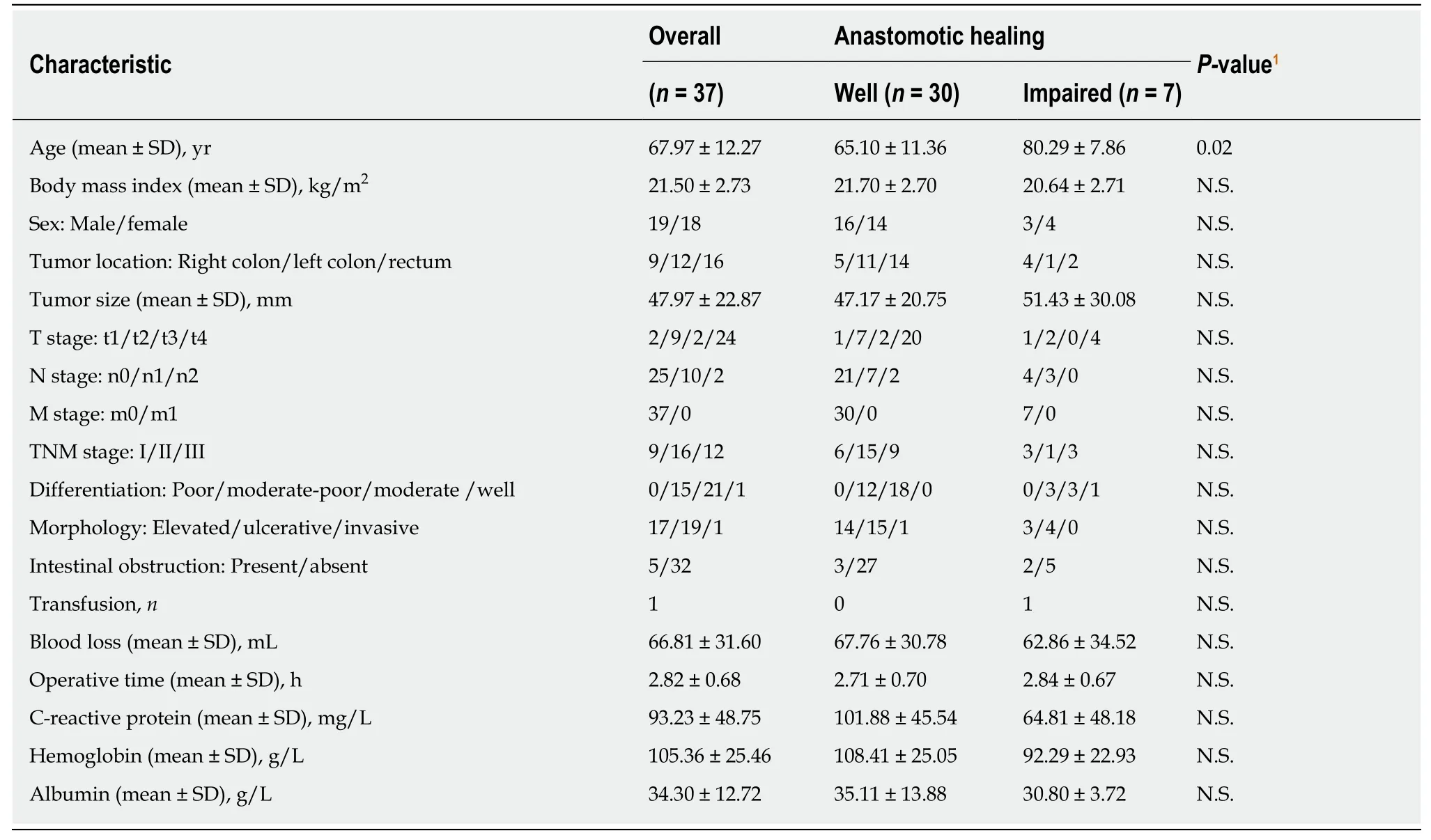
Table1 Clinicopathological characteristics
Predictive ability of selected bacterial taxa assessment for healing status of anastomoses
Univariate analysis and multivariate analysis showed that age was the only significant clinical variable for anastomotic healing (OR [odds ratio] = 1.223;95%confidence interval [CI]:1.032-1.449;P= 0.020),and age could be used as an independent factor predictive of the healing status of anastomoses (Figure 3,AUC =0.838;95%CI:0.697-0.979;P= 0.006;the optimum cut-off value was 69.5).Six species(Alistipes shahii,Dialister pneumosintes,Corynebacterium suicordis,Porphyromonas asaccharolytica,Vibrio diazotrophicus,andClostridium leptum) were selected as the potential predictive factors.Chi-squared analysis showed no correlation between these six bacteria and age.The 95%CIs of three bacteria (Porphyromonas asaccharolytica,Vibrio diazotrophicus,andClostridium leptum) ranged from 0 to 1 in the ROC curve and were therefore excluded.In predicting the healing status of anastomoses in the two groups,we found that usingAlistipes shahii,Dialister pneumosintes,andCorynebacterium suicordiswere less useful than age (Figure 3,AUC = 0.824;95%CI:0.691-0.957;P= 0.008).However,the predictive ability was significantly improved if age was in combination with the three bacteria species,compared with the predictive model containing age only (age andAlistipes shahii,AUC = 0.886;95%CI:0.774-0.998;age andDialister pneumosintes,AUC = 0.912;95%CI:0.807-1.000;age andCorynebacterium suicordis,AUC 0.874;95%CI:0.735-1.000) (Figure 3,P< 0.01).The predictive model combining age withDialister pneumosintesproved to have the highest discriminatory ability (AUC = 0.912;95%CI:0.807-1.000;P= 0.001,the optimum cut-off value was 0.143),which was even higher than the model combining two bacterial species with age (age,Alistipes shahii,andCorynebacterium suicordis,AUC= 0.886;95%CI:0.774-0.998) (Figure 3,P< 0.01).Besides,age in combination with three bacterial species had a relatively equal predictive ability to the model in which age was combined withDialister pneumosintes(Figure 3).
DISCUSSION

Figure1 Structural change of the intestinal microbiota between impaired-healing group (n = 7) and well-healing group (n = 30).
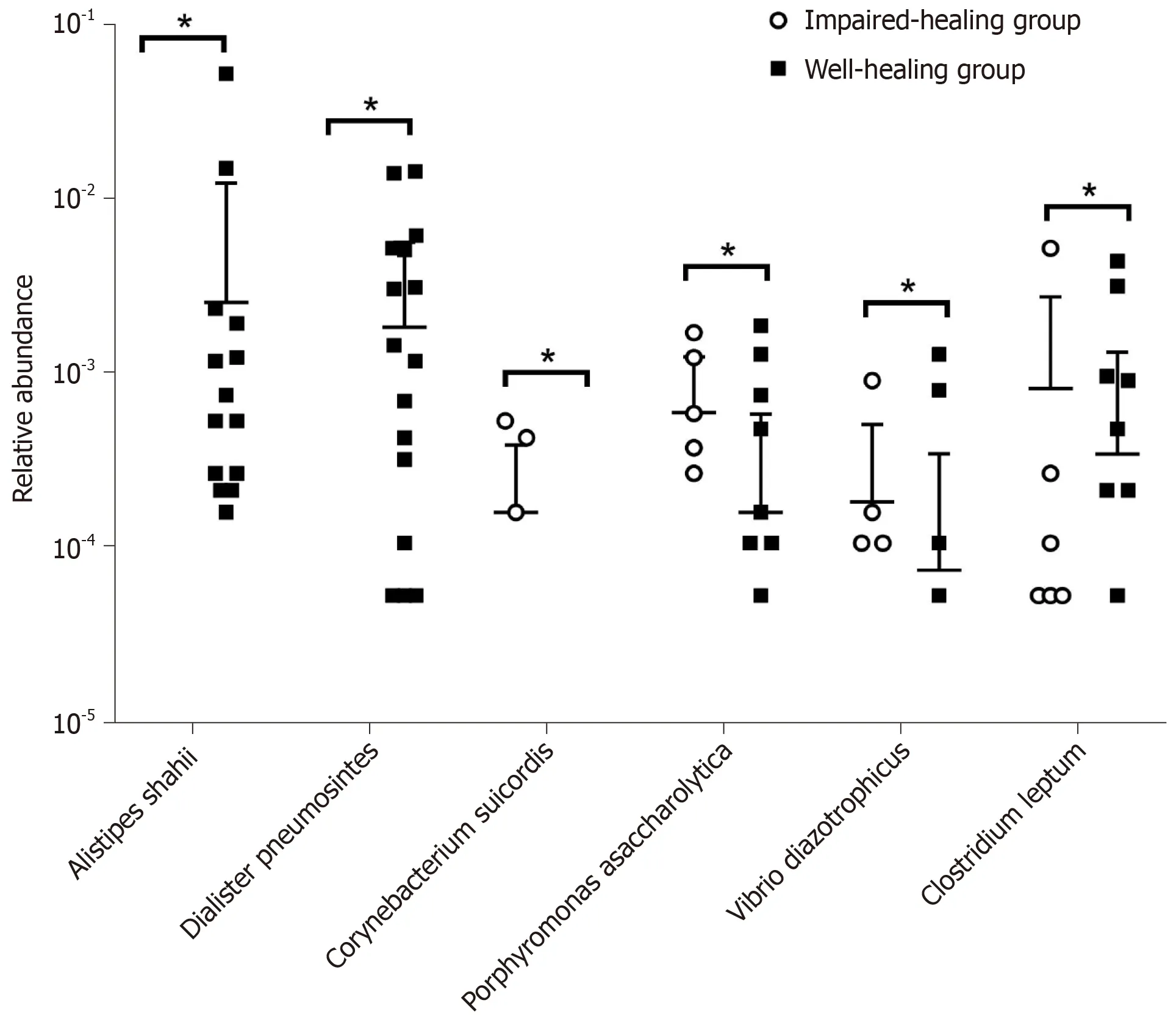
Figure2 Correlation of intestinal microbiota with anastomotic healing.
This study showed that the community structure was different between the impairedhealing group and the well-healing group.Six bacterial species were significantly correlated with anastomotic healing.Alistipes shahiiandDialister pneumosinteswere significantly enriched in the well-healing group,which were not identified in the impaired-healing group,indicating thatAlistipes shahiiandDialister pneumosintespossibly contribute to anastomotic healing.However,the high abundances ofCorynebacterium suicordis,Porphyromonas asaccharolytica,Vibrio diazotrophicus,andClostridium leptumwere strongly correlated with impaired anastomotic healing.Corynebacterium suicordiswas only detected in the impaired-healing group,suggesting that it might be positively associated with impaired anastomotic healing.Alistipes shahiiis a Gram-negative,strictly anaerobic,and rod-shaped bacterium[41].Dialister pneumosintesis an obligate anaerobic Gram-negative rod associated with periodontal diseases and other oral infections[42].Recently,it was reported thatDialister pneumosinteswas related to hepatic abscess and bacteremia[42,43].Corynebacterium suicordisis a Gram-positive,non-motile,non-spore-forming,catalase-positive,and rod-shaped bacterium[44].Porphyromonas asaccharolyticahas been previously reported to be associated with CRC and was correlated with lipopolysaccharide and energy biosynthetic pathways[45].Vibrio diazotrophicusis a Gram-negative,facultatively anaerobic,halophilic,motile,and slightly curved rod-shaped bacterium[46].Clostridium leptumis closely related to ulcerative colitis and significantly different in the ulcerated and the nonulcerated regions[47].However,only a few studies investigated the role of these bacteria in anastomotic healing.To the best of our knowledge,this is the first report that these bacteria species were studied with the anastomotic healing in CRC patients.Based on our research and literature data,we speculated that these bacteria affect anastomotic healing through invasive ability and inflammatory mechanisms.It was revealed thatEnterococcus faecaliscontributed to the pathogenesis of impaired anastomotic healing by enhancing collagen-degrading activity and activating intestinal tissue MMP9[12,34].Pseudomonas aeruginosa,Serratia marcescens,andEnterococcus faecalis,which express the collagenolytic phenotype,were reported to be associated with the impaired anastomotic healing[30-34].Although there is a lack of direct evidence of the effects of intestinal microbes on anastomotic healing,several previous studies suggested that a correlation might exist between microbes and MMP activation.Fusobacteria(especiallyFusobacterium variumandFusobacterium necrophorum) were found to stimulate the secretions of MMP-9,MMP-13,and IL-8 from epithelial cells[48],whilePorphyromonas endodontaliscould produce lipopolysaccharides to induce the expression of MMP-9 through NF-κB signaling[49].The mechanism by which these microbes affect anastomotic healing is worth further studying.

Figure3 Microbial factors combined with clinical factor improve accuracy of predictive models for anastomotic healing.
van Praaghet al[36]found that impaired anastomotic healing was linked to the intestinal microbiota,particularly to a higher abundance of mucin-degrading members of theBacteroidaceaeandLachnospiraceaefamilies.Besides,a lower microbial diversity was found to be related to the impaired healing of anastomoses.Researchers speculated that a disturbed microbial composition could affect the metabolic balance and weaken colonization resistance to pathogenic bacteria involved in the occurrence and development of impaired anastomotic healing.The result was obtained from 123“donuts” in which a stapled colorectal anastomosis was made.It was different from our sampling site (mucosa tissue adjacent to the surgical margin).Intestinal microbiota near the anastomotic site has been proved to interact with intestinal tissue and is likely to affect the healing[50].Our study found that fewer OTUs were identified in the impaired-healing group,and the microbial diversity was lower,although the result was not statistically significant (which could be explained by the small sample size in this study).Patients might have a higher risk of developing impaired anastomotic healing when their microbial diversity was low[36],thus a full awareness of the role of intestinal microbiota in anastomotic healing is helpful in identifying high-risk patients and contributes to mitigating the potential severe clinical outcome caused by impaired anastomotic healing.
Sciutoet al[20]identified that older age (hazard ratio,2.42),male sex (hazard ratio,3.03),and lower anastomosis level (hazard ratio,2.68) were the risk factors for impaired anastomotic healing.Consistent with the findings from previous reports,we also found that age (OR = 1.223) was significantly associated with the impaired healing of anastomoses and could be used as an independent risk factor to predict the healing status of anastomoses.We found that patients older than 69.5 years were more prone to develop impaired anastomotic healing.Notably,our results suggested that three associated bacteria species,especiallyDialister pneumosintes,in combination with age significantly improved the predictive ability,compared with the model containing only age.van Praaghet al[36]suggested that samples were more likely to have impaired anastomotic healing if the total sum ofLachnospiraceaeandBacteroidaceaein them was higher than 60% and the Simpson diversity score was <0.75.Thus,the effect of the intestinal microbiota on the predictive value of anastomotic healing is positively useful in clinical nursing and postoperative surveillance.
Technical factors such as the tension on the suture line,accurate suture placement,and blood supply were vitally important in ensuring the optimal healing of anastomoses[51].Unfortunately,it was difficult to be controlled precisely,and this is true to the most experienced and technically proficient surgeons.Besides the preventive measures implemented during the bowel resection,the early detection and diagnosis were equally important to prevent the patients from developing complications and severe clinical outcome caused by impaired healing of anastomoses.Our findings provided new clinical evidence for the theory that intestinal microbes are involved in the anastomotic healing and might contribute to the screening of the potential targets for the early diagnosis and treatment of impaired anastomotic healing.
In conclusion,the mucosa-invasive microbiota is associated with the impaired anastomotic healing in the patients enrolled in this study.Alistipes shahii,Dialister pneumosintes,andCorynebacterium suicordis,which are not related to age,could be used as the supplementary factors in the prediction of the healing status of anastomoses in CRC patients after radical resection of CRC.
ARTICLE HIGHLIGHTS
Research background
The clinical symptoms of impaired anastomotic healing are typically not recognized.However,if not appropriately treated in time,impaired healing could easily evolve into severe postoperative complications.Thus,early diagnosis and prediction of impaired anastomotic healing are highly necessary.
Research motivation
A large number of studies reported that intestinal microbiota contributes to the development of impaired anastomotic healing.A full understanding of the role of intestinal microbiota in anastomotic healing can help identify high-risk patients and alleviate the potentially serious clinical outcomes caused by impaired anastomotic healing.
Research objectives
To identify the specific bacteria related to impaired anastomotic healing and to evaluate the predictive ability of the microbiota taxa for the healing status of anastomoses.
Research methods
Margin-surrounding mucosa samples derived from seven colorectal cancer (CRC) patients with impaired anastomotic healing and thirty well-healed CRC patients were respectively collected and the bacterial community was characterized by 16s rRNA gene sequencing.Wilcoxon test and chi-squared test were performed to analyze the statistic differences of bacterial taxa in the two groups.The predictive ability of the bacterial taxa for the healing status of anastomoses was evaluated by the area under the receiver operator characteristic curve.
Research results
The community structure was different between the impaired-healing and the well-healing groups.Six bacteria species (Alistipes shahii,Dialister pneumosintes,Corynebacterium suicordis,Porphyromonas asaccharolytica,Vibrio diazotrophicus,and Clostridium leptum) were significantly correlated with anastomotic healing.Age was highly associated with the impaired healing of anastomoses.Three bacteria species (Alistipes shahii,Dialister pneumosintes,and Corynebacterium suicordis) in combination with age noticeably improved the accuracy for predicting the healing status of anastomoses.
Research conclusions
The mucosa-invasive microbiota was associated with the anastomotic healing in the research subjects.Alistipes shahii,Dialister pneumosintes,and Corynebacterium suicordis could be used as the supplementary factors in the prediction of the healing status of anastomoses in CRC patients after radical resection of CRC.
Research perspectives
Our findings provided new clinical evidence for the theory that intestinal microbiota is involved in the anastomotic healing,and it contributes to the screening of potential targets for the early diagnosis and treatment of impaired anastomotic healing.
 World Journal of Gastrointestinal Oncology2019年9期
World Journal of Gastrointestinal Oncology2019年9期
- World Journal of Gastrointestinal Oncology的其它文章
- Gallbladder cancer harboring ERBB2 mutation on the primary and metastatic site:A case report
- Clinical characteristics and surgical treatment of schwannomas of the esophagus and stomach:A case series and systematic review
- Detection and management of oligometastatic disease in oesophageal cancer and identification of prognostic factors:A systematic review
- Colorectal cancer fecal screening test completion after age 74,sources and outcomes in French program
- MicroRNA-331 inhibits development of gastric cancer through targeting musashi1
- Tumor progression-dependent angiogenesis in gastric cancer and its potential application