
Mindfulness-based cognitive therapy for university students with depression,anxiety,and stress symptoms:a randomized controlled trial
2019-09-16 03:40:56AlessandraAlmeidaAssumpCarolinaSilvaPenaCarmemBeatrizNeufeldMaycolnTeodoro
Alessandra Almeida Assump??o ,Carolina Silva Pena,Carmem Beatriz Neufeld,Maycoln M.Teodoro
1 Department of Psychology,Federal University of Minas Gerais,Belo Horizonte,Brazil
2 Department of Statistics,Federal University of Minas Gerais,Belo Horizonte,Brazil
3 Department of Psychology,State University of S?o Paulo,Ribeir?o Preto,Brazil
Abstract
Key words:mindfulness;university students;college students;depression;anxiety;stress;self-esteem;quality of life;randomized controlled trial
INTRODUCTION
High prevalence rates of depression,anxiety and stress symptoms in college/university are a growing concern in the literature.These psychopathological symptoms in university students represent a health problem,often neglected and with serious implications for Higher Education Institutions that impact on education and prospective career.This problem reinforces the need for specific intervention and prevention measures for students in this context.Supporting student's health and wellbeing is an investment that results in considerable economic,academic,social and personal benefits.
Comorbidity among depression,anxiety,and stress is common (Kang et al.,2009;Lamers et al.,2011;Lai et al.,2015).Depression is a disease linked to a decrease in quality of life,increased self-injurious behaviors,physical illness,drug dependency and risk of suicide (Buchanan,2012).Depressed students report significant academic problems (lower grades,inability to concentrate,absenteeism,and interpersonal difficulties).Anxiety and stress are associated with lowered academic performance,increased professional misconduct,decreased empathy and an increase in substance abuse and suicide (Shiralkar et al.,2013;Takebayashi et al.,2018).
Two national studies show this association between depression,anxiety,and stress in university students.According to College Health Assessment Survey in the US (American College Health Association,2018),18.1% of students had been either diagnosed or treated for depression,and 22.1% of students had been either diagnosed or treated for anxiety disorders.The students reported that stress was the primary reason they performed poorly in a course,exam,or project (33.2%);and 50.2% reported that academics were “very difficult” to handle.In the Brazilian report FONAPRACE (2014),60.49% of the students sought psychological attention at some time during the undergraduate course,and 80% of the students interviewed reported emotional difficulties to perform their academic activities,and at least 30% of the participants used a psychiatric medication.Concerning mental suffering,the data collected showed that:almost 60% of the sample had anxiety symptoms,20% persistent sadness,10% fear or panic,32% insomnia,6% suicidal ideation and 4% suicidal thoughts.According to the report of the authors,the suicidal ideation and thoughts are important indexes because in absolute terms it can be said that almost 60 thousand students had suicidal ideation and that approximately 40 thousand had thought about suicide in the year surveyed.
There is an increasing interest in integrating meditation interventions into university contexts aiming to treat,to prevent and to teach new coping strategies to students deal with stress (Gallego et al.,2014),anxiety (Song and Lindquist,2015) and depression (Shapiro et al.,1998).Mindfulness has been found to improve coping skills and reduce emotional distress in college students (Rosenzweig et al.,2003;Beddoe and Murphy,2004;Kang et al.,2009).The leading representative of this approach,Kabat-Zinn (1982) defines mindfulness as the ability to draw attention to the experiences that occur in the present moment accepting them without judgment.Bishop et al.(2004) distinguished two components of mindfulness:(1) self-regulation of the attention paid to immediate experience;and (2) an orientation to self-experience of the present moment,characterized by curiosity,openness,and acceptance.The practice of mindfulness emphasizes observing present events rather than comparing them,evaluating them,or ruminating them with past or future experiences (Brown and Ryan,2003).Mindfulness-based interventions (MBIs) are mental trainings for the cultivation of mindfulness states that serve as a coping strategy for stressful situations (Bowen et al.,2015).MBIs have seen exponential growth over the past three decades.Interest in the area comes from the promising results of scientific studies as well as extensive media coverage of these findings through publications on the potential benefits of mindfulness interventions (Creswell,2017),related to physical and mental health (Ludwig and Kabat-Zinn 2008) or positive cognitive,affective and interpersonal outcomes (Brown et al.,2015).
Contemporary approaches based on mindfulness began in the United States in the late 1970s with the creation of the Mindfulness-Based Stress Reduction Program (MBSR),developed by Kabat-Zinn.Since that time,research with MBSR has shown good efficacy in treatment for different clinical conditions and psychiatric disorders (Ludwig and Kabat-Zinn,2008).In the early 1990s,John Teasdale,Mark Williams,and Zindel Segal hypothesized that mindfulness training could have positive effects in preventing relapse in patients with recurrent depression.Influenced by the MBSR program,they created an 8-week intervention that contained beyond Mindfulness the underlying theory of Cognitive-Behavioral Therapy and gave rise to Mindfulness-Based Cognitive Therapy (MBCT).MBCT is recommended by the UK National Institute for Health and Clinical Excellence (2009) as a standard intervention to prevent recurrence of depression for those with a history of three or more crises in their Guidelines for the Management of Depression.In the present study,we will use an abbreviated version of MBCT.
Early detection and intervention of depressive,anxiety and stress symptoms during college can reduce the incidence,severity,and duration of future mental health problems (Cuijpers et al.,2008).It is also evident that effectively treating these symptoms in college positively impacts in quality of life,better academic performance (Einsenberg et al.,2009) and prospective career (Franco,2010;Franco et al.,2010).The positive effects of mindfulness suggest the pertinence of including this intervention in the university contexts.Besides,the efficacy of psychological interventions for stress,depressive,and anxiety symptoms for this population is understudied,and there is a need to develop feasible evidence-based interventions (Gawrysiak et al.,2009;Lee,2015).The primary aim of this study was to address a gap in the literature by conducting and evaluating the efficacy of an abbreviated MBCT program for mild and moderate depressive,anxiety,and stress symptoms in university students.The primary study hypotheses were:(1) to obtain clinical and statistically significant improvement in the reduction of depression,anxiety,and stress symptoms;(2) to achieve an increase in positive measures (self-esteem and quality of life);(3) to find clinically and statistically significant differences in depression,anxiety,and stress symptoms maintained three months after the end of the intervention.

Strengths and limitations
PARTICIPANTS AND METHODS
Study design
This is a randomized parallel-controlled trial.As indicated on the CONSORT (Figure 1),if included following the screening based on a randomization table,participants were assigned to MBCT (n= 63),or the wait-list control (control) (n= 62).We delivered 10 MBCT subgroups.The principal investigator used a computer number random generator and concealed the randomization table.The training was delivered in groups and consisted of 5-11 participants with duration of 6 sessions of 90 minutes each.The symptoms were assessed at baseline,2 weeks and 3 months after the intervention.Pre-test and posttest measurements were performed by research assistants who were previously trained,and the follow up was completed by participantsviaemail.

Figure 1:Consort diagram flow.
The nature of psychological intervention does not mask or blind patients and therapists;however,some procedures were adopted to mask some stages of data collection and analysis:(1) the statistician who was involved in the statistical analysis was blind to treatment allocation;(2) only undergraduates performed data collection;(3) we collected the post measures before the session beginning to avoid bias induced by the meditative state of the session.A critical factor is that the loss of participants in psychological intervention studies is due to several reasons,among them the lack of adherence to the interventions.One measure used to minimize the decrease of participants throughout the study was to contact them (by phone or e-mail) before each group session to remind them of the meeting.This strategy has shown good results in group interventions (Neufeld,2015).This trial was registered in the Brazilian Clinical Trial Registry (http://www.ensaiosclinicos.gov.br) (registration No.RBR-4mmvpc) on July 21,2017.
Participants
The inclusion criteria were:(1) being regularly enrolled at the university;(2) men and women aged ≥ 17 and ≤ 60 years;(3) depression symptoms (mild and moderate) measured by the Beck Depression Inventory-II (BDI-II) (scores ≥ 14,≤ 28);(4) anxiety symptoms measured by Beck Anxiety Inventory (BAI) (scores > 0) and (5) stress symptoms measured by Perceived Stress Scale (PSS) (scores > 0).The exclusion criteria were:(1) no recent history (past 12 months) of severe psychopathology (psychosis,suicide attempt and risk,panic disorder and posttraumatic stress disorder);(2) having epilepsy or some neurocognitive disorder;and (3) practice mindfulness meditation frequently (in the last 6 months).
In the study,we accepted participants who were using psychotropic drugs for depression and anxiety.We considered this variable in the data analysis as a possible confounding variable and weekly,additions or suspension of psychotropic drugs were noted for both participants who start the study using medication as well as participants who start using during the programme.However,we verified that the ones who started with a medication finished with the same medication,and those who did not use any medication continued not to use them.Participants were screened at the university in two phases (1) between August and September 2017;and (2) between February and March 2018.
Recruitment
The research was widely advertised at the Federal University of Minas Gerais by (1) putting up posters in the university buildings,(2) using Social Media,(3) using the institutional website and (4) circulating e-mails presenting the study and inviting students to attend the research.Advertising focused on letting students know about the study directing them to a dedicated e-mail (atencaoplenaufmg@gmail.com) for more information (e.g.,the nature of the research and its procedures).There were no restrictions regarding gender,course or area of studies.Those interested in participating in the research were scheduled to perform an interview.Informed consent was obtained from all participants included in the study and all of them were submitted to an interview to verify sociodemographic variables and medical and psychiatric conditions through a battery of tests to evaluate the inclusion and exclusion criteria.Assessment measures were administered and collected by a trained undergraduate research assistant not involved in the design of the research or the intervention to avoid experimenter effects.
Ethical considerations
The students were informed of the purpose of the research,how long the study would take,that they were free to decide whether to participate and that they could withdraw at any time.We explained that the questionnaire used in this study would not disclose the name of the respondent but would instead use serial numbers.All participants provided written informed consent (Additional file 1).The study protocol was approved by the Ethics Committee of Federal University of Minas Gerais,in Belo Horizonte,Brazil (approval No.2.025.573) on April 20,2017 (Additional file 2).The randomized clinical trial was enrolled on the REBEC Platform (http://www.ensaiosclinicos.gov.br) on July 21,2017,under registry RBR-4mmvpc.We published the study protocol elsewhere (Assump??o et al.,2018).
Intervention
The programme was adapted,maintaining the main structure and components of MBCT.The developed program was based mainly on “Mindfulness-Based Cognitive Therapy” by Segal et al.(2002) and in explanations,activities,and practices proposed in subsequent books “Mindfulness:Finding Peace in a Frantic World” by Williams and Penman (2015) and “Practical Mindfulness Handbook” by Teasdale et al.(2016).These books addressed not only depressive symptoms,but also included anxiety and stress symptoms.Among the modifications in the program,there was:(1) a decrease in time from 120 minutes to 90 minutes,(2) a decrease from eight to six sessions,(3) an exclusion of a full-day retreat,(4) a decrease in proposed home practice time of 45 minutes to a progressive increase of the practice from 10 to 25 minutes and (5) the home practice frequency suggested was five times instead of six times.We based these changes on the literature that points out that there is no data on optimal session time or home practice for MBIs (Creswell,2017).A viability study was done to analyze the program feasibility (Assump??o et al.,2019).
All sessions were conducted by a licensed psychotherapist (the first author) with 4 years of personal mindfulness practice and were also supervised bi-weekly mindfulness certified instructor (Oxford Mindfulness Centre and Mente Aberta,UNIFESP).The same group of psychotherapists conducted the sessions for all groups to ensure consistency in procedures and information receipt.We recorded all intervention groups sessions and,subsequently,discussed with the supervisorviaSkype.
In the mindfulness intervention group,various types of mindfulness practices were introduced to the participants,starting with simple ones,and then progressing to the more complex mindfulness practices.For example,during the first session,the meditation on breath was presented and practiced.We introduced meditations on senses,such as sound and taste,and meditation on walking in subsequent sessions.The sessions were divided into activities as follows:The first session:(1) introduction to mindfulness and autopilot,(2) body scan,and 3-minute meditation.The second session:(1) appreciation of here and now,(2) breathing,and 3-minute meditation,(3) learning about feelings and thoughts.The third session:(1) staying in the present moment,(2) working with the body and the breathing,and 3-minute meditation.The fourth session:(1) recognizing aversion,(2) sound and thought mediation.The fifth session:(1) let it be,(2) exploring difficulties,(3) loving-kindness meditation.The sixth session:(1) recalling training,(2) relapse prevention strategies,and (3) body scan.
The MBCT took place in a weekly meeting within 6 weeks and was delivered in groups constituted by 5-11 participants.Each session took 90 minutes.The sessions followed a standard format in which began by discussing the homework of the previous session (frequency of meditation,any obstacles to completion,and the meditation experience).Subsequently,a brief exposition on the theme of the week was carried out accompanied by one or two activities to reinforce the presented content.Then the participants practiced one or two meditations.At the end of each meditation exercise,the therapist and the participants discussed emotional,physiological,and cognitive experiences.After these activities,the tasks of the next week were explained,and the meeting ended.At each session,handouts were given to illustrate concepts and provide reflections on home activity.
Homework was considered an important element of treatment,and participants were encouraged to spend some minutes daily practicing mindfulness activities,often using guided meditation recordings.The daily practice of mindfulness was highly recommended but was not required to continue participation in the training.In the present study,it was decreased the home practice time from 40 minutes to a progressive increase of the practice from 10 to 25 minutes,and the home practice frequency suggested was five times per week instead of six times.The homework corresponded to the weekly meeting,reinforcing techniques used in class.To guarantee that participants observed their home practice,they were asked to complete a short form in each session.The participants were asked to compile in a journal any significant information related to their depression,anxiety and stress symptoms.
The controls waited for 6 weeks.After this period,they also received the MBCT intervention.
Outcome assessment
The participants in all groups completed five short questionnaires.As primary outcomes,the participants were asked to complete the BDI-II (Arnau et al.,2001),BAI (Beck et al.,1988),PSS (Reis et al.,2010),and as secondary outcomes the Rosenberg Self-Esteem Scale (RSES) (Martín-Albo et al.,2007),and the 12-item Short-Form Health Survey (SF-12) (Ware et al.,1996).We obtained the copyright permission to use SF-12.The questionnaires were completed three times in the study:pre-intervention (1 week),post-intervention (8 weeks),and follow-up (3 months after the intervention) and the estimated time to complete all study instruments was about 20 to 25 minutes.The instruments to evaluate primary and secondary outcomes were presented and published elsewhere (Assump??o et al.,2018).
Sample size calculation
The sample calculation was performed using the G Power 3.1 software (Faul et al.,2007).A priori type of power analysis was based on repeated measures ANOVA 2 × 3,in which “2” represents the number of groups and the “3” are related to time repetitions.We considered the effect size (f= 0.25),with a type I error of 5% (α= 0.05) and 90% power (β= 0.10),and reached the minimum number of 36.However,we decided to consider a minimum sample size of 48 subjects (24 required per group),considering a 30% drop-out rate as indicated previously (Bastelaar et al.,2008).
Statistical analysis
The R software version 3.5.1 (https://www.R-project.org/) was used to analyze the data.Descriptive statistics were used to describe the sociodemographic characteristics of participants and to examine the distribution and frequency of scores on the instruments.Chi-square,Fisher Exact,and Mann-WhitneyUtests were employed to compare the baseline measurements of the demographic and dependent variables between the two groups.A Linear Mixed Effects (LME) model was adjusted to compare the repeated measures of depression,anxiety,stress,self-esteem,and the quality of life scores within and between the MBCT and control groups.The Tukey's test was applied as apost hocof the LME's significant coefficients.P-values less than 0.05 (two-sided) were defined as statistically significant.
RESULTS
Sample description
Table 1 shows sociodemographic variables of university students;there were no significant differences between the MBCT and control groups regarding age,education degree,marital status,working status,and drug use.There was a significant difference regarding gender (P= 0.03) since the control group had 74% (n= 25) of females and the MBCT group 93% (n= 39).The mean age was 25.1 ± 6.9 years in the MBCT group and 24.5 ± 4.6 years in the control group.Most participants were single (85.5%) and married (8%).The sample was represented by 69.7% of graduates and 30.3 % post-graduates.There were 21 categories of courses and the most common fields of study were Psychology (27 students),Phono-audiology (13 students),and Engineering (7 students).Regarding working status,59% (n= 45) of the students did not work,20 students worked under 20 hours per week and had a scholarship,and 11 students worked between 20 and 30 hours per week.About drug use,93% (n= 71) did not smoke,57% (n= 43) drank periodically (36% of them among 1 to 3 times per week and 36% monthly),and 4% (n= 3) reported using marijuana sometimes.
There was no significant statistical difference in BAI,PSS,RSES,and SF-12 (subscale PCS) scores.In the pre-test,the MBCT sample could be categorized as moderately depressed (BDI-II:21.5 ± 7.7),and the control group mildly depressed (19.0 ± 7.8) besides,24% (n= 18) of the sample was diagnosed with MDD as assessed by MINI major depression module.There were no significant differences in the proportion of individuals diagnosed with MDD across conditions (MBCT = 21%;control = 26%) (P> 0.05).The MBCT and the control sample could be categorized as mildly anxious respectively (18.5 ± 10.6) and (17.4 ± 10.3).The MBCT sample could be categorized as more stressed than the mean (21.37) respectively (35.6 ± 7.3) and (33.4 ± 10.3).The levels of self-esteem in the MBCT group were (26.2 ± 4.9),the control sample (RSES:M = 27.4,SD = 6.2).The levels of quality of life in the MBCT group were (PCS:53.6 ± 7.0;MCS:34.2 ± 8.2),and the control sample (PCS:52.5 ± 9.8;MCS:37.5 ± 7.7).
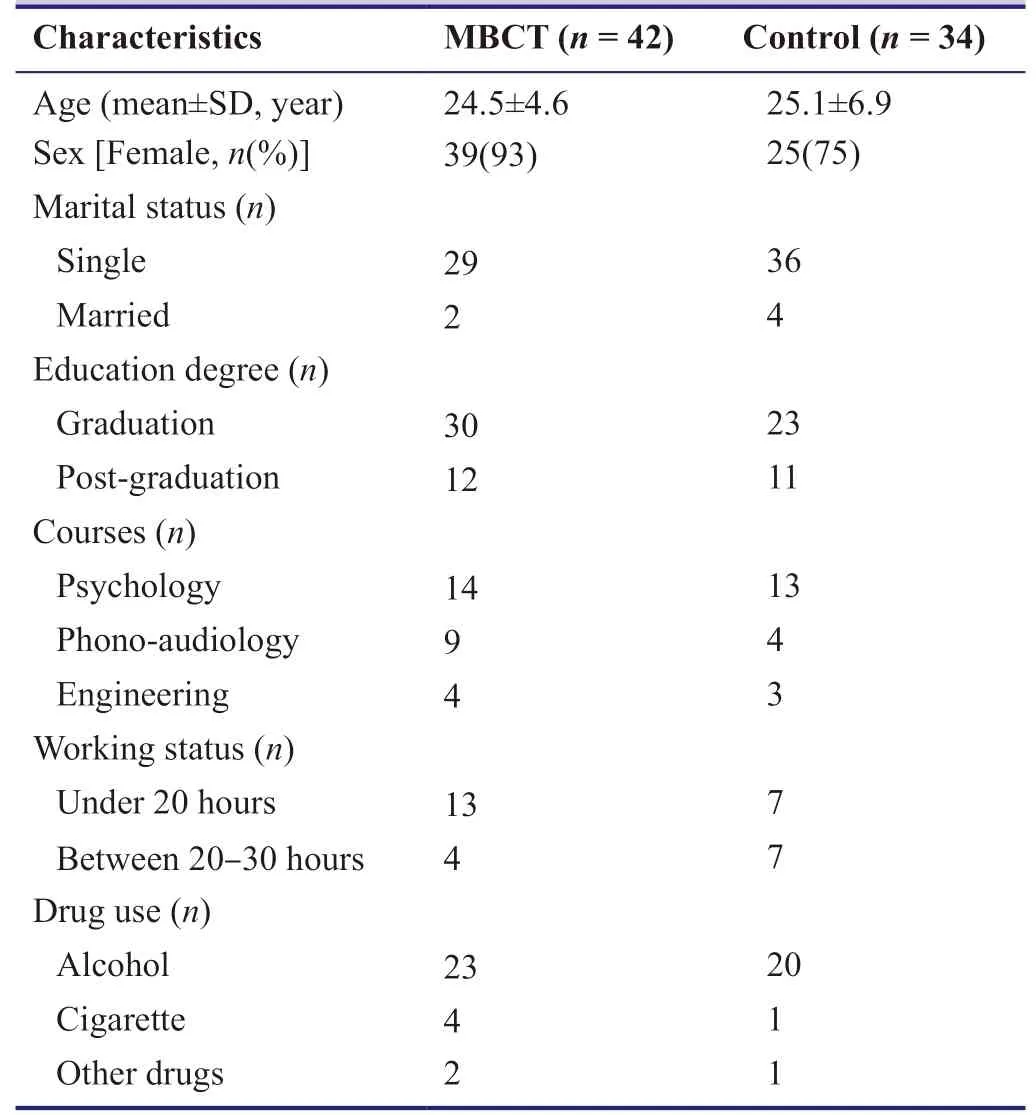
Table 1:Participant characteristics across treatment conditions
Some participants (n= 5) were taking psychiatric medications (MBCT group = 3 and control group = 2),and a total of 21 (28%) students stated that they were receiving therapy during the study (MBCT group = 12 and control group = 9).Ten students had started therapy 1 month before the study;eight received therapy once a week,and three every other week.Important to note that a series of chi-square analyses indicated that treatment response and remission did not differ as a function of gender,whether participants were using medication at pre-treatment,or whether participants were on psychological treatment.
The final count of participants was 76,consisting of 12 males and 64 females (84%).Out of the 125 students who were qualified,49 (39.2%) students did not complete the study due to schedule conflicts,heavy load of academic work,or other personal reasons.Twenty-nine of them left the intervention before starting it,ten students left after the first session,and after the second session,five students started working after the study started which interfered with the training schedules.Five students felt overwhelmed with university work and did not complete the last session.Fifteen students did not complete the questionnaires for the follow-up.
Outcomes of pre-tests and post-tests between the two groups
Regarding outcomes of pre- and post-tests between the MBCT and control groups,it is possible to verify in Table 2 the mean and standard deviation of all responses of interest for the control and MBCT groups at baseline,post-test,and follow-up.

Table 2:Mean and standard error of interest responses by group and time
To evaluate the treatment effect,an LME was fitted for each response of interest.This model can adjust unbalanced data and includes the student and the workgroup as a random effect component.The variables:“Education degree (Graduation or Post-Graduation),” “Gender” and “Age” were inserted in the adjustment of all models as fixed control effects.The variables “Time (baseline,post-test and follow-up),” “Group (Control and MBCT)” and the interaction between them are the fixed effects of the model that allow testing the effect of the treatment applied.If the interaction is significant,it means that the response of interest varied in different ways (baseline,post-test,and follow-up) for the control and MBCT groups,suggesting that the applied treatment affected the variables.However,the interaction is not significant,but the “Time” variable is significant,it indicates that there was a significant change in the interest response after participating in the research,but there is no difference between the MBCT and control groups.To test the significance of the fixed effects of the model,we used the backward variable selection method.Table 3 shows theP-values associated with each coefficient.
As shown in Table 3,considering the 5% level of significance,it can be concluded that the observed changes in baseline,post-test and follow-up within the MBCT group differ to that observed in the control group for the variables BDI-II and MCS.If we adopt the 10% level of significance,this conclusion could also be extended to the PSS and RSES variables.This result can be understood visually from the analysis of Figures 1 and 2.
Figures 2 and 3 show,respectively,that for the BDI-II and MCS responses the mean and standard error estimated by the LME model for the control and MBCT groups at the three measurement moments.As displayed in Figure 2,it is possible to observe that the reduction in BDI-II,in the baseline,was more pronounced within the MBCT group than in the control group.Figure 3,however,shows that the increase in MCS,relative to the baseline,was more pronounced within the MBCT group than within the control group.Visually,the presence of interaction can be confirmed in both graphs,because the lines of the control and MBCT groups intersected,indicating different levels of slope in the observed change within the groups.

Table 3:P-value of each coefficient of LME models

Figure 2:Mean and standard error for the LME model of BDI-II response,by group and time.

Figure 3:Mean and standard error for the LME model of MCS response,by group and time.
Where interaction was significant,Tukey'spost hoctest was also applied to confirm the statistical significance of the results discussed from the graphic visualization.The results are shown in Table 4.
In Table 4,it is possible to verify for the MBCT group that there was a significant change in BDI-II in both Post-test and Follow-up,to its Baseline.For the control group,however,it is considered that the difference was only significant in the results of Follow-up in relation to its baseline.Regarding MCS,there was a significant change in the post-test and follow-up,to the baseline,only for the MBCT group.The baseline,post-test,and follow-up comparison between the control and MBCT groups was not significant,yet the effect of the treatment can be confirmed by the fact that only within the MBCT group,a significant difference was detected between the baseline and the post-test in the two variables.
Table 5 shows the coefficients of all adjusted final models,in which the significant variables were maintained by the backward selection method.From the coefficients,it is possible to observe the size of the increase or reduction expected in the average of each response of interest,according to the category analysed.The table also shows the 95% confidence interval of each coefficient generated by the bootstrap method.For example,in the case of the BAI variable,there was an average reduction of 3.2 in the post-test to the baseline,and of 7.3 in the follow-up to the baseline.For this variable,there was no significant difference between the observed behavior in control and MBCT groups.For the variable BDI-II,in turn,if the student belongs to the MBCT group,it is expected that in the post period there is an average reduction of (0.6 + 8.3 = 8.9) to the baseline.Nevertheless,if the student belongs to the control group,the expected reduction in the BDI-II variable in the post-test will be only 0.6.For the Follow-up time,the expected reduction to the baseline for the control group is equal to 5.9 and for the MBCT group equal to (5.9 + 5.2 = 11.1).
DISCUSSION
In this study,we aimed to address a gap in the literature by conducting and evaluating the efficacy of an abbreviated MBCT program for mild and moderate depressive,anxiety and stress symptoms in university students relative to a control.The treatment was designed specifically for implementation on a college campus (i.e.,uncomplicated,brief,feasible).The significant findings were that MBCT effectively reduced depression at post-treatment,and the treatment gains were maintained in follow-up.Besides the intervention increased the quality of life (MCS component) in post-test and follow-up.
According to the primary study hypothesis “after the intervention,the participants will obtain clinical and statistically significant improvement in the reduction of symptoms of depression,anxiety and stress,” we observed that the hypothesis was partially corroborated since only depression had a statistically significant improvement.The intervention did not affect the BAI and PSS.The second hypothesis “the intervention will lead to an increase in the scores of the positive measures (self-esteem and quality of life)” was moderately corroborated since the intervention effect was observed MCS component (SF-12).Moreover,the last hypothesis “clinically and statistically significant differences related to the reduction of symptoms of depression,anxiety,and stress will be maintained 3 months after the end of the intervention” was also partly corroborated since the intervention decreased depression effectively in follow up.
Studies that explore the effects of mindfulness on university students differed in designs and type or length of interventions.However,there were sufficient similarities in the literature to support the current study.The results of this trial are consistent with the findings in Gallego et al.(2014) which was a 3-armed randomized controlled trial comparing MBCT intervention with a Physical Education Condition and control.The authors found a decrease in depression scores (comparing the control group) but in their study,the scores of anxiety and stress were also decreased.In comparison to our study,one possible explanation is that in Gallego et al.'s study,the intervention was delivered in 8 weeks and our study was abbreviated to 6 weeks.Their study did not have a follow-up;consequently,it is not possible to know if the results would be maintained.
Another similar study design using MBIs was delivered by Mcindoo et al.(2016),and aimed to evaluate the effectiveness of two interventions (MBI and Behavioural Activation) for university students with major depressive disorder.The intervention was delivered in an individual format.The study was performed with 50 undergraduate students who presented the diagnosis.It was observed that both treatments presented better efficacy when compared to the control.Interventions lasting 4 days had a median effect size (d= 0.68-0.77) for depression symptoms and between 56% and 79% of the patients showed significant clinical improvement.Among the statistically significant benefits were the decrease in depression (between 75% and 85%),rumination and stress scores and increased levels of mindfulness were also found.The positive results were observed in the 1-month follow-up after treatment.The other studies found in the literature with similar design did not use MBCT but used MBSR instead.The findings were also congruent to the present study,regarding decreased levels in depression (Shapiro et al.,1998;Song and Lindquist,2015).Regarding stress in de Vibe et al.(2013) did not find significant differences in comparison to the control.However,significant decreases in stress scores were found in other studies (Oman et al.,2008;Kang et al.,2009;Erogul et al.,2014;Song and Lindquist,2015).
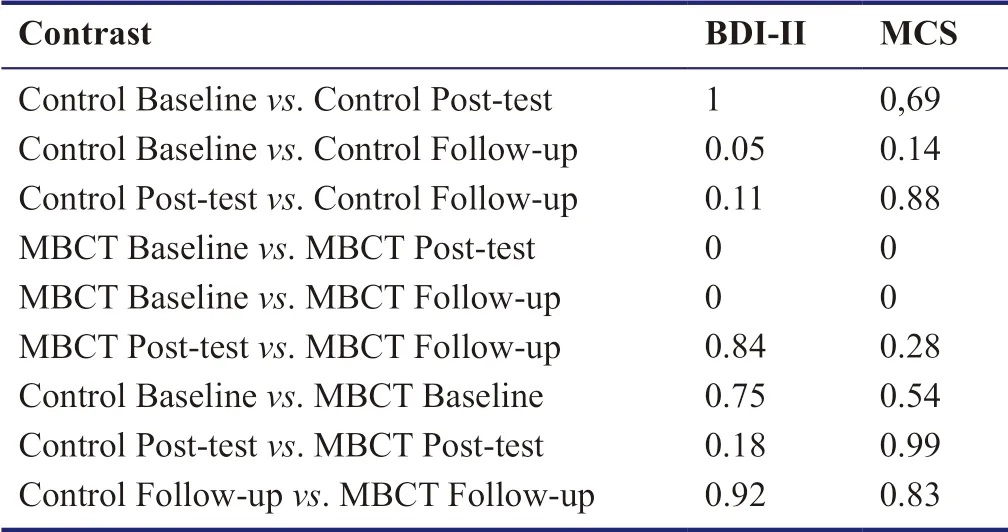
Table 4:Tukey's post hoc test for significant interaction between group and time

Table 5:Coefficients and 95% confidence interval for the adjusted final LME model of each response variable
MBCT training has two components (1) a didactic classroom element and (2) an experiential and embodied component that comes about through meditation.Although there is some meditation that takes place in class,the most part of meditation is a homework.Among our study participants,the mean meditation per week was 2.27 (SD = 0.5),it was advised 5 times per week for the participants.Given the relatively low home meditation practiced in our study,we speculate that the learning that occurs as part of the classroom training may play an important role in effecting positive change.Better adherence to home meditation would likely have produced a more robust effect,but this will always be challenging to achieve in this specific population given their academic burden.
The present study is associated with some significant limitations,and we will discuss seven of them.The first limitation is regarding our small sample which was homogeneous demographically and clinically,pointing out that these variables can decrease external validity and generalizability of the findings.Besides from the randomization phase to the conclusion of the intervention,39.2% of the students randomized did not start the intervention,and 35.5% of the students that participate did not complete the follow-up phase.The second problem was that no active treatment (i.e.,cognitive behavior therapy,physical activity) was included in comparison to MBCT,which limits our conclusions regarding the effectiveness of the intervention.The third restraint observed was that we did not measure the level of mindfulness,and thus could not determine whether the intervention increased it.Another limitation was that the data were obtained based on self-report,which is subjected to recall bias and not very reliable.A fifth problem was that we did not check contamination that might have occurred between the two groups (e.g.,control participants observing or participating in MBCT homework or conversations related to the intervention).An additional limitation is a short period of follow-up applied in this study which may limit conclusions on the utility of the intervention.The last restriction is that the abbreviated MBCT version was performed for 6 weeks.However,the current study outcomes appear to be affected regarding stress and anxiety symptoms.
Further research is needed to confirm these findings,and future research can be improved using (1) more participants and a more diverse sample;(2) adding active treatments;(3) measuring dispositional mindfulness;(4) measuring biological markers (brain scanning and cortisol level) which may make the results more affirmative;(5) checking contamination between groups;and (6) adding more follow-ups.
Despite the limitations,the results suggest that MBCT helps university students learn how to manage adverse emotional states,especially,depression and to improve their quality of life.The study has implications for cost-effective treatment of depression symptoms since this time-efficient treatment may serve as effective and proactive interventions for students at the risk of experiencing increased depression and poor quality of life.The findings from this study can yield useful information to university counselling centers and might be more feasible in university/college clinics that typically have a high volume of students with psychological needs associated with time constraints and a shortage of mental health professionals to support the demands.
Additional files
Additional file 1:Informed Consent Form.
Additional file 2:Ethical approval documentation (Portuguese).
Author contributions
Concept and design of study protocol:AAA and MMT;data collection and analysis,drafting of the manuscript:AAA and CSP;revision of manuscript:CBN and TMM.All authors approved the final manuscript for publication.
Conflicts of interest
The authors have no conflicts of interest to declare.
Financial support
This study was supported by Coordena??o de Aperfei?oamento de Pessoal de Nível Superior (CAPES).
Institutional review board statement
The study protocol was approved by Ethics Committee of Federal University of Minas Gerais,in Belo Horizonte,Brazil on April 20th,2017 (approval No.2.025.573).This study was performed according to the statement of theDeclaration of Helsinki,and informed consent of the study procedure was obtained from all participants.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient and their legal guardian consent forms.In the forms the patients have given their consent for their images and other clinical information to be reported in the journal.The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity.
Reporting statement
This study followed the Consolidated Standards of Reporting Trials (CONSORT) 2010 guidelines.
Biostatistics statement
The statistical methods of this study were reviewed by the biostatistician of University of Minas Gerais.
Copyright license agreement
The Copyright License Agreement has been signed by all authors before publication.
Data sharing statement
For data sharing,individual participant data will not be available.However,the study protocol and informed consent form will be made available beginning 3 months and ending 5 years following article publication to investigators whose proposed use of the data has been approved by an independent review committee identified to achieve aims in the approved proposal.In order to gain access,data requestors will need to sign a data access agreement.Proposals should be directed to alesump@gmail.com.
Plagiarism check
Checked twice by iThenticate.
Peer review
Externally peer reviewed.
Open access statement
This is an open access journal,and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License,which allows others to remix,tweak,and build upon the work non-commercially,as long as appropriate credit is given and the new creations are licensed under the identical terms.
 Asia Pacific Journal of Clinical Trials:Nervous System Diseases2019年3期
Asia Pacific Journal of Clinical Trials:Nervous System Diseases2019年3期
- Asia Pacific Journal of Clinical Trials:Nervous System Diseases的其它文章
- Effectiveness of inpatient alcohol detoxification and psychotherapeutic support program:a prospective self-controlled study at a tertiary hospital in Nepal
- Bacteriological profile of endotracheal tube aspirates in head injury patients admitted in Neurosurgical Intensive Care Unit:a cross-sectional study from a tertiary care hospital of Central Nepal
- Treatment with a halved dose of antipsychotics in patients with schizophrenia who relapse while receiving high-dose antipsychotic therapy