
Dry cupping therapy and the wellness management of health travelers
2019-01-09 03:31:42SalmanMajeedMahwashMajeedMoshoodAmeenatAjike
Traditional Medicine Research 2019年1期
Salman Majeed*, Mahwash Majeed, Moshood Ameenat Ajike
1School of Management, Fuzhou University, Fujian, China. 2Government College University, Faisalabad, Pakistan.3Clinical Medicine and Therapies, Fujian Medical University, Fujian, China.
Background
Individual’s health and wellness are shaped by the woven notions of biology, spirituality, emotionality, and lifestyle associations [1]. Despite the remarkable advancement of the 100 years old traditional western system of medicine,which diagnoses diseases and offers medical treatments through drugs, surgeries or other applicable modalities,the risk of side-effects and inefficacy in diagnosing and treating diseases, sometimes, are also acknowledged [2].This dilemma has adversely impacted the health and wellness desires of people when countries across the globe recently reporting expectations of their individuals for a healthy and active lifestyle [3]. Recently, it has been noted that people expect to avail health and wellness treatments by experiencing alternative treatments, for example, acupuncture, dietary supplements, herbal therapy, and cupping therapy (CT) [4]. The tradition of cupping therapy is centuries old [5]. CT stands among one of the ancient methods of alternative medical treatments across different civilizations [6]. It is noted that the introduction of cupping therapy was first mentioned inEber’s papyrusin the ancient Egypt, which is considered an oldest medical book published in 1550 B.C. [7]. There are also numerous shreds of evidences in the history including Herodotus (a Greek historian, 400 B.C) which documents the use of cupping therapy in treating different diseases, for example, appetite disorder,headache, fainting,etc.[8].Historical perspective of cupping therapydocuments its existence in central Europe, the Middle East, and other Asian countries [6, 9].The importance of CT can be ascertained from the fact that it has been acknowledged and accepted as official therapeutic practice in the Chinese hospitals since 1999[10]. Although the popularity of CT as a method of improving individuals’ health and wellness conditions is in its embryonic stage within the Pakistani context, CT treatments exist and still contribute to the nation’s alternative and complementary medical system.
CT is a non-drug therapy just like scraping therapy,massage, and acupuncture. Several techniques are involved in it, for example, skin-lacerated traditional wet cupping therapy (WCT), dry cupping therapy (DCT)without skin-laceration, and moving cupping therapy which is often termed as cupping massage [11].
Despite promising effects and worthy contributions made by CT to achieve its medical objectives, CT yet suffers from some societal concerns for their general application and acceptance [12]. For example, reported skin burn incidents due to CT in Africa and China question the applicability of CT in general practices [13,14]. Moreover, WCT (Hejama/Hijama) is often associated with unhygienic procedural arrangements and the risk of infection transmission into the human body [15]. WCT and its associated infection risk have been proved in transmitting Hepatitis B, C, and HTLV-1 [16, 17]. These reasons are contradicting to the promising notions of wellness and its management through WCT in order to bring an overall improvement in the quality of life of health care consumers. However, this dilemma could be managed by hiring trained CT professionals and using sterilized CT tools in order to ensure health, safety, and wellness management practices through alternative therapies. From this perspective, DCT has been found safe and helpful in achieving its desired medical objectives.
Hence, the concept of wellness management revolves around the dimensions of individual’s physical health, for example, body pain (BP), bodily movement (BM),psychological states, and quality of life in tandem with the satisfied levels of individuals’ expectations in this overall phenomenon,etc., mental state, and interaction with the society and its environment [18]. However,wellness management is disturbed when an individual’s body meets with certain physical dysfunctions which negatively influence human stature. This further leads to impact the energy production and consumption functions in the human body in tandem with the complexities of social, emotional, and psychological roles performed by individuals [19].
It is noted that health tourism involves traveling of all kinds linked to health enhancement [20]. Moreover,health tourism involves the concept of wellness tourism in its breadth and scope in tandem with the overlapping notions of medical tourism [21]. It is documented that one of the recent trends in cross-border tourism is the human’s traveling quest to pursue health and wellness for bringing improvement in the quality of life [21-23].Hence, people attempt to travel both locally and internationally to search relevant health and wellness treatments with or without the interventions of surgical procedures. Thus, the research on traditional and complementary medicine (T&CM) is gaining the attention of the scholars and professionals of the health,wellness, and medical industries recently. It is noted that T&CM practices have been observed with the unprecedented attention of the residents and travelers/tourists of both developed and developing countries [24]. It has been estimated that T&CM method of treatment has been favored by about 80% of the population of the developing countries where CTs are also considered as one of the main components of T&CM[24]. It has been observed that the impact of DCT and its association with other traditional and conventional treatment methods have been discussed and clinically trialed in order to treat different medical reasons [9, 25,26]. However, a majority of studies lack sufficient evidence to document the effectiveness of DCT in improving the overall health, wellness, and the quality of life preferences of individuals, including patients or those individuals who desire to live quality life better than before.
Some scholars conducted small-scale research on the use of T&CM in Pakistan. These scholars focused on student population, patient population, and other specified adults in their research [27-29]. However, T&CM research in Pakistan focusing on the perceptions and responses of the population from different cohorts of life is yet succinct. Moreover, many research studies on CTs and DCT have been conducted in different countries.However, the research on DCT in Pakistan is also on its lower empirical grounds. Hence, the present study attempts to examine and empirically elucidate the effects of DCT on the health status (HS) of the travelers in Faisalabad (Pakistan).
The notions of health and wellness were depicted in Figure 1 in order to examine the associations among health travelers’ perceptions of their health and quality of life, which are directly concerned with the notions of wellness concept. Additionally, it proposes that:
Hypothesis 1 (H1):Health perceptions have a significantly positive influence on the HS of travelers.
Hypothesis 2 (H2):DCT has a significantly positive influence on the HS of travelers.
Hypothesis 3 (H3):DCT significantly mediates the relationship between the health perceptions of travelers and their HS.
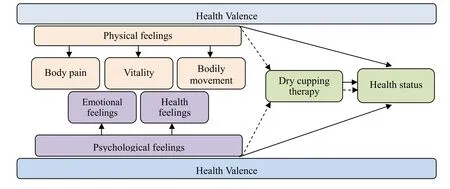
Figure 1 Health valence: the associated framework of DCT and health status
Methodology
Research design, settings, and ethics
In order to achieve the study objectives, the present study incorporates quasi-experimental (pre-post assessment)design. Nevertheless, this research is also accompanied by examining the direct influence of health perceptions about the quality of life and the mediating role of DCT in this overall phenomenon. The study was conducted in Coural Wellness Center (CWC) Faisalabad, Pakistan, a non-profit health care center that purposefully serves patients with Pakistani herbal medicine, Unani medicine,Chinese traditional medicine, and homeopathy in tandem with various therapies including yoga, acupuncture,warm-baths, and gymnasium which are managed under the patronage of Coural Associates. Necessary official approval was sought prior to conducting the study from the resident officer of CWC.
Subjects
Study subjects were recruited via advertising banners for preventive and wellness CT at different squares of main Faisalabad city. Faisalabad city has a mixture of different attractions, that is, culture, business, food, and heritage tourism attracting travelers from different parts of the country. Hence, the likelihood of a variety of sample was present in Faisalabad population. In order to assess the eligibility of interested subjects, a research assistant first screened subjects over the telephone. Inclusion criteria of the study was based on facts that participants should be between 18 and 80 years of age, not suffering from any serious mental or physical disease, not taking phenytoin,codeine, chemotherapy, immunosuppressive drugs, or anticoagulants, as well as residents or travelers in Faisalabad, and willing to participate in DCT study with their written informed consent. Additionally, it was also considered that female participants should not be breastfeeding, pregnant, or menstruating. Among 357 phone-calls’ screening interviews between October 19,2017, and November 7, 2017, 321 subjects were finally invited and requested to confirm their participation in DCT sessions scheduled between December 10, 2017,and December 31, 2017, at CWC Faisalabad.
Materials and procedures
This study will report results from two perspectives. The first perspective is based on two sub-dimensions, that is,whether health perceptions, physical states, psychological states, directly influence the HS/quality of life of individuals or not, and whether DCT has any of its mediating role in influencing the relationship between the health perceptions and the HS of study respondents.Second, the response of study subjects will be examined in order to note their feelings about the quality of life before and after DCT interventions following the quasi-experimental design.
In order to collect data on health perceptions, wellness,and quality of life outcome in tandem with the role of DCT intervention, a questionnaire was developed. BP variable was measured by adopting the validated instrument of Pain Perception Scale [30], vitality (V) was measured by adopting items from short form 36 (SF-36)health survey questionnaires [31], and general BM/function was measured by adopting validated instruments from Pain Perception Scale and SF-36 [30,31]. Psychological feelings constructs were also measured by adopting validated instruments, emotional feelings (EF) were measured by adopting the validated instruments of HADS scale (hospital anxiety and depression scale) [32], and physical feeling scale [33]because of its certain physiological premises, health feelings (HF) were measured by adopting the validated scales of SF-36 and physical feeling scale [31, 33]. HS outcome was measured by adopting the validated instruments of SF-36, while questions on DCT interventions were added. Physical, mental, and general health and wellness perspectives were made part of the questionnaire in tandem with questions on the evaluation of physical problems and functioning, mental health and functioning, social functioning, vitality, and pain sensation in the body [34]. Moreover, all validated instruments were little adjusted according to the nature of the present study. Study subjects were requested to rate responses about their feelings of health, wellness, and the quality of life on a seven-point Likert scale of 1-7; where lowest score was given number 1, while the most ideal situation was given number 7. The questionnaire also incorporated questions to collect demographic information about subjects, for example, gender, age,educational level, and occupation. The questionnaire was completed in three parts, the first response was taken immediately following the first DCT intervention, second response was taken after 48 hours of the first DCT intervention, and the third part was completed by contacting study participants over the telephone after 30 days from the second DCT intervention. Data on complications, feelings of wellness, better physical and mental health, and improvement in the quality of life were gathered by asking questions to individuals who participated in the present study.
Before DCT interventions, researchers of the present study made sure that inclusion criteria had been met by the study subjects. This was done by conducting a brief interview prior to DCT interventions. Additionally, an oral explanation was provided to subjects about DCT and a printed questionnaire was handed over to them.Questionnaires were filled by the subjects and mentioned their present states prior to first DCT intervention, and thereby confirming their informed consent in writing.Questionnaires were filled under the supervision of researchers and the presence of professional trainers with DPT certifications. Study subjects also agreed to revisit CWC Faisalabad within 48 - 72 hours from the first DCT intervention, and provided their telephonic responses after 30 days from the second DCT intervention about changes in their body and health as well as about the feelings of wellness and quality of life. However, 24 of the participants were excluded before proceeding to first DCT interventions due to their scheduling and follow up reasons.
A total of 297 subjects were then directed towards the designated experimental DCT rooms and requested to lie down in a prone position. After cleaning the area between shoulders and middle of the back, DCT was performed at the back of subjects through disposable cupping glasses by inverting 3-5 glasses, each with a 25-50 mm diameter.A manual hand pump was handled in order to create a vacuum and suction inside the cups. The created vacuum drew up the skin of subjects inside each cup [35]. The created vacuum was directly associated with the tolerance level of subjects. Cupping glass suction was gradually increased which further expanded skin inside the glass and turned skin color into red. It has been noted that increased blood circulation, autohemolysis, and muscle tension are further associated with the reasons of changing skin color [36]. DCT was performed for 15-20 minutes up to two times in 72 hours (allowing 48 hours in between the first and second DCT interventions) with the assistance of seven CT therapist. After DCT sessions, the participants were allowed to rest for a while and then requested to leave DCT experimental room. After experiencing DCT, the participants were further advised to refrain from bathing for a couple of days.
Statistical design
Gathered responses were statistically analyzed through partial least square structural equation modeling (SEM)technique using Smart partial least square-SEM in order to measure the direct/indirect significance levels of health perceptions and DCT intervention on the HS of travelers in Faisalabad. SEM was additionally considered appropriate in order to examine the results of pre-post assessments of DCT interventions by calculating mean and standard deviation. An alpha coefficient of 0.05 at 95% confidence interval was considered effective for all statistical measurements. Descriptive analysis was performed by calculating percents, cumulative percents,minimum and maximum levels of the mean and standard deviation.
Results
A total 297 subjects filled questionnaires before and after first DCT intervention, however, 26 of the subjects did not provide full information. Hence, considered their responses as incomplete, 63 subjects are excluded because subjects did not visit therapy clinic for second DCT intervention. 21 subjects were excluded because no telephonic response was received after a couple of attempts made by the researchers for the final response of study participants. Finally, 187 subjects’ data were retained (Figure 2) and statistically analyzed in the system. Table 1 results show the demographic profiles of study respondents. Results show that 126 of study participants (67.38%) were females and 61 were males(32.62%) with mean ± standard deviation age as 35.62 ±8.89. Majority of the participants were the residents of Faisalabad city (54.55%) followed by travelers from other cities. Majority of the participants were between age cohorts of 18 and 50 years. Only 28 (14.96%) subjects were having the college or above level of educational background. 74 (39.57%) subjects were having contractual nature of work.
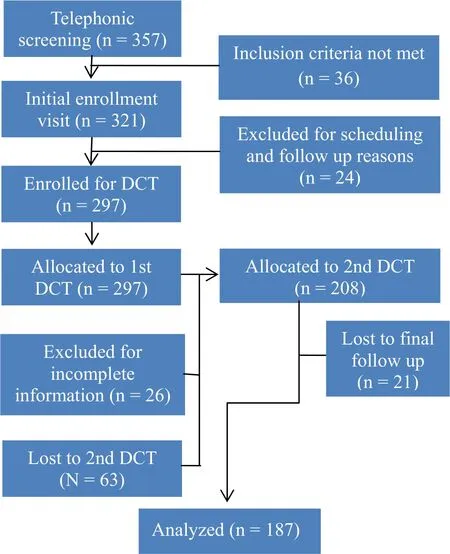
Figure 2 The screening and recruitment of participants
Measurement model results
The questionnaire, which is developed by adopting items from different standardized tools and adjusted according to the context of the study, including three questions for BP, three questions for V, three questions for BM, three questions for EF, three questions for HF, four questions for DCT, and five questions for HS. These questionnaire items are presented by calculating loading values (LV).LV are helpful to evaluate and explain various constructs in tandem with their reflective and latent meanings impartial least square -SEM analysis. Moreover, LV are considered important to analyze the associations of reflective and latent variables. It is noted that LV should be more than the threshold level of 0.70 in order to show the 0.50 level of variance in latent variables [37, 38].
Table 2 results show that all LV of this study were significant at 0.05%, and greater than 0.70, showing convergent validity. Composite reliability, Cronbach’s alpha values (for internal consistency measures), and construct level average values were found appropriate,i.e., > 0.60, > 0.70, and > 0.50 respectively [38, 39].Constructs’ level average square root were found greater than reflective items correlations, hence, showing discriminant validity [38, 40]. Heterotrait-monotrait results (Table 3) were further supporting to discriminant validity as well [40], i.e. < 0.85 or 0.90.
Structural model evaluation
Co-efficient of determination (R2) value for endogenous variables was over 0.1 % level, and found appropriate as presented in Table 2 and Figure 3 [40]. The values of f2and Q2, showing effect sizes, were found fluctuating(Table 4), from lower to maximum limits, i.e. 0.02(lower), 0.15 (medium), and 0.35 (maximum) limits [37].β andPvalues (Table 4) were supporting significantly positive relationships of BP (β = 0.192,P= 0.003),vitality (β = 0.138,P= 0.001), BM (β = 0.207,P= 0.001),and EF (β = 0.169,P= 0.004) at 0.05 level with HS except for general HF (β = 0.093,P= 0.065). Moreover,β andPvalues for dry cupping therapy were found having significantly positive influence on the quality of life outcome (β = 0.213,P= 0.002).
Mediation testing
In order to examine the mediating role of DCT, a non-parametric bootstrapping method was used [38, 41].Table 5 shows that DCT had a significant positive influence in mediating the relationship between all the constructs of physical feelings and psychological feelings with the HS (t > 1.96,P= 0.05). The indirect effect of lower beta values for each construct as compared to direct beta values were supporting to note that DCT absorbed a certain percentage of direct impact [41].
Table 6 results further show the detailed results of the constructs of physical feelings and psychological feelings,by taking a comparative analysis of subjects’ pre and post assessment with DCT interventions. Paired t-test results show that health and wellness status of study participants significantly improved after 1st and 2nd DCT interventions for general physical health, general mental health, emotional balance, and expressions, feelings of relaxation, inner peace, vitality, sleeping, movement out of bed, sitting, or working, and good mood along with DCT satisfaction, and were found significant (AllP<0.05). It is also found that subjects reported their social functioning improvement after 1st and 2nd DCT interventions; however, paired t-test results show that the differences between pre and post assessments of social functioning after 48 hrs from the 1st DCT, and 30 days from the 2nd DCT intervention, were not statistically significant (P= 0.057). By analyzing study’s results, it has also been found that health and wellness status of participants significantly improved through the quality of life measures after 1st and 2nd DCT interventions.However, all health and wellness items in tandem with DCT satisfaction were found better at their mean and standard deviation values after 2nd DCT intervention as compared to 1st DCT intervention except for social functioning. These results are presented in Table 6.
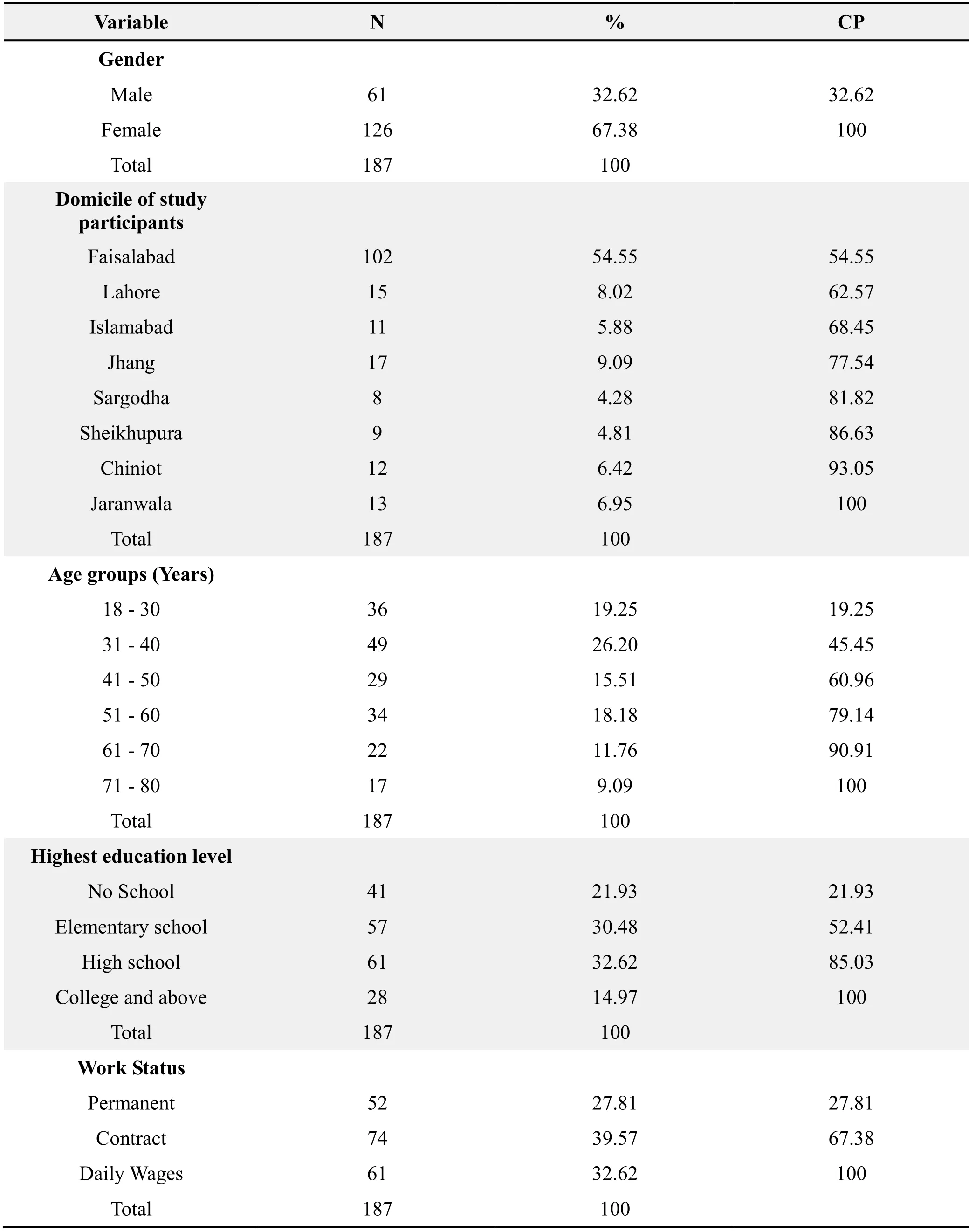
Table 1 Socio-demographic profiles of study respondents
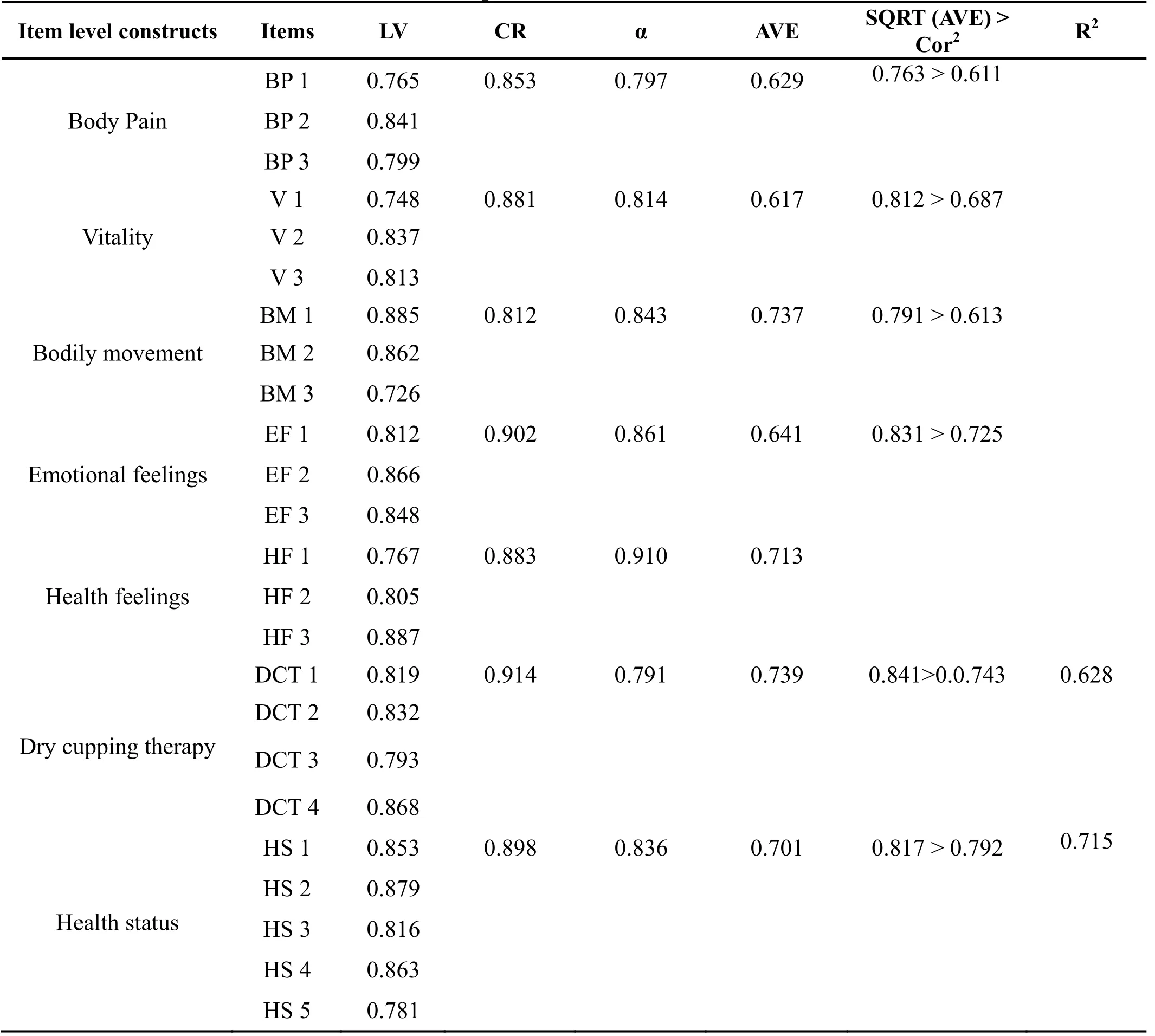
Table 2 Results presented for measurement model
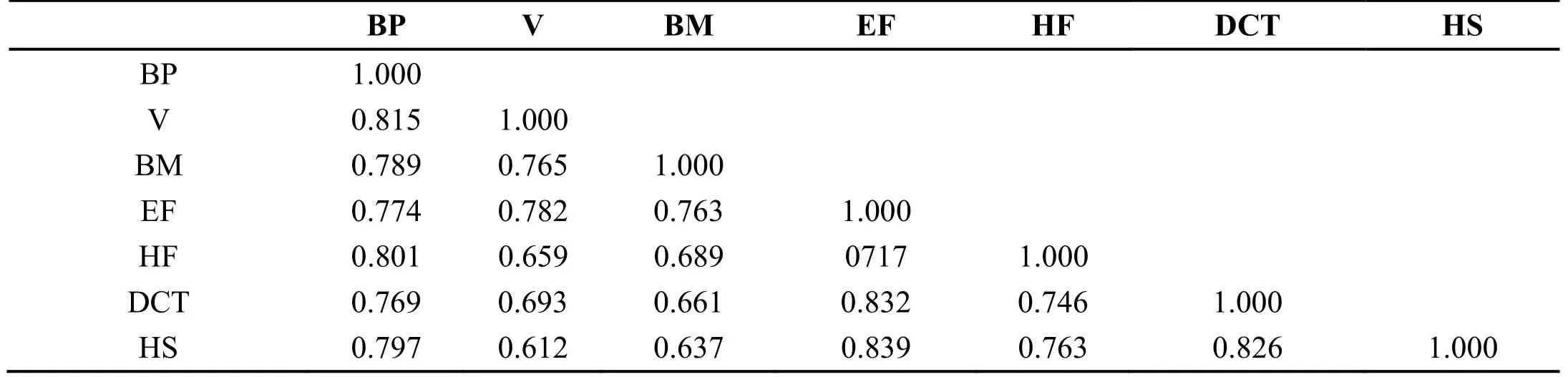
Table 3 Results presented for heterotrait-monotrait (HTMT) analysis
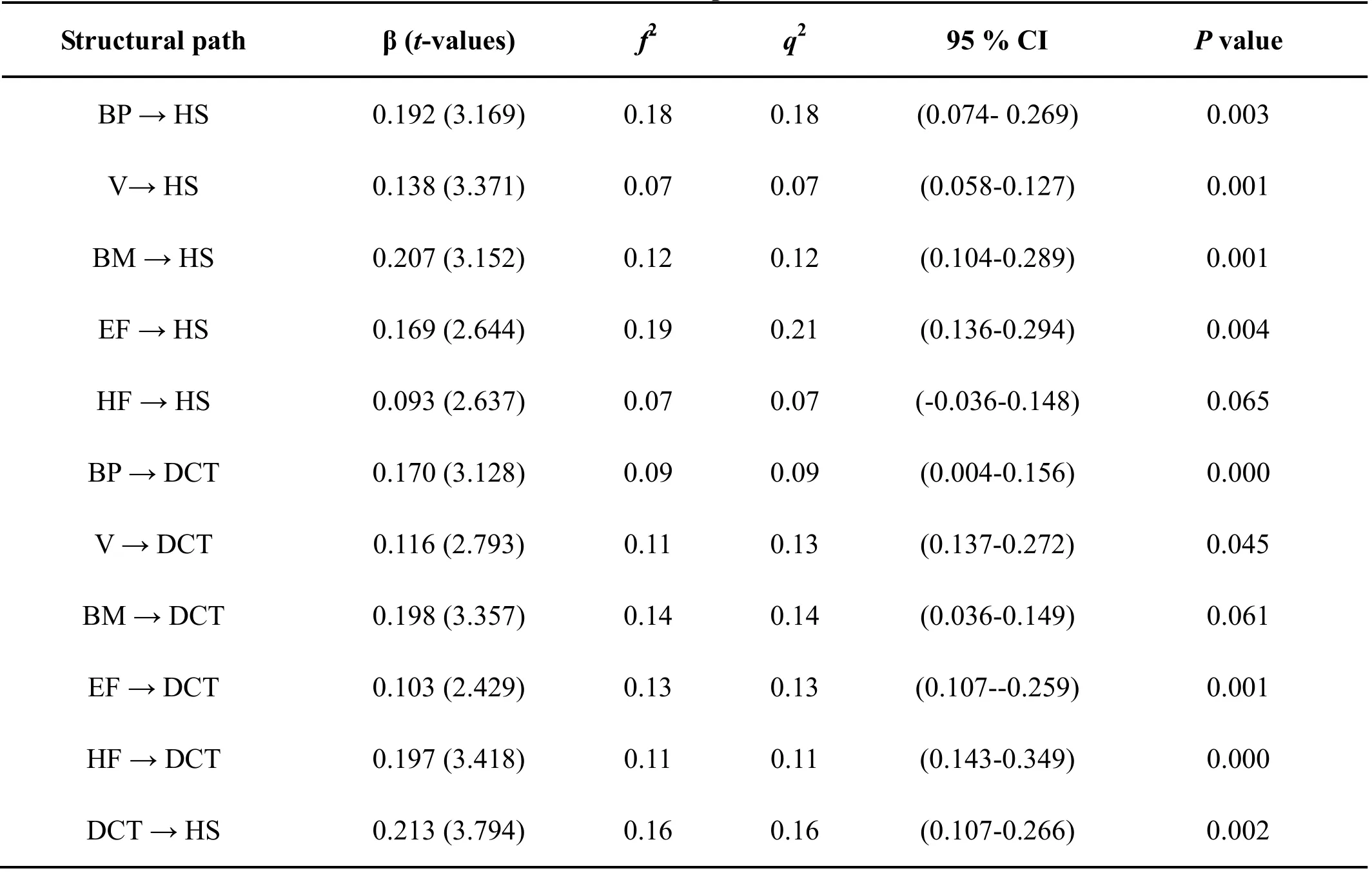
Table 4 Direct-effect path coefficients
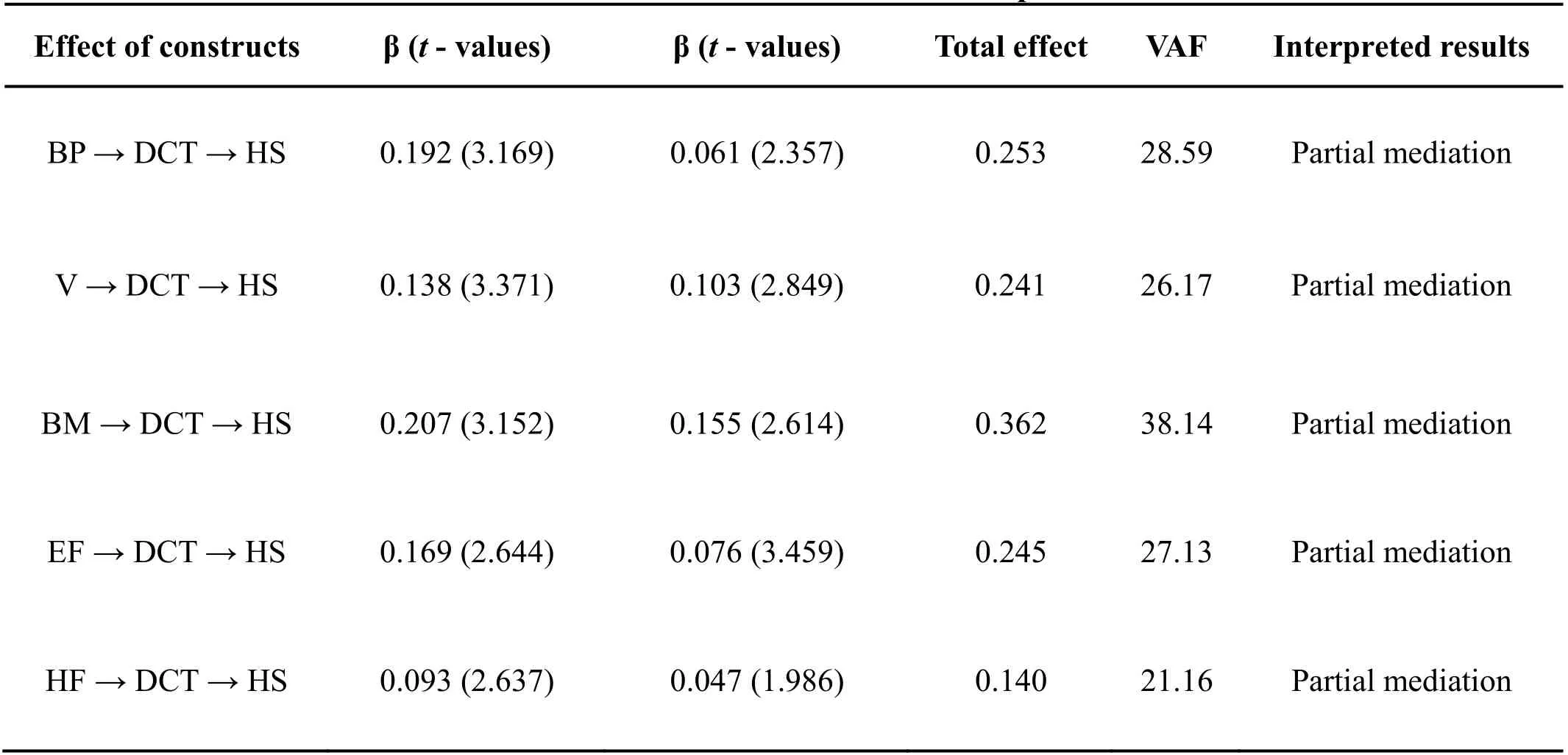
Table 5 Mediation/indirect effect and relationship verifications
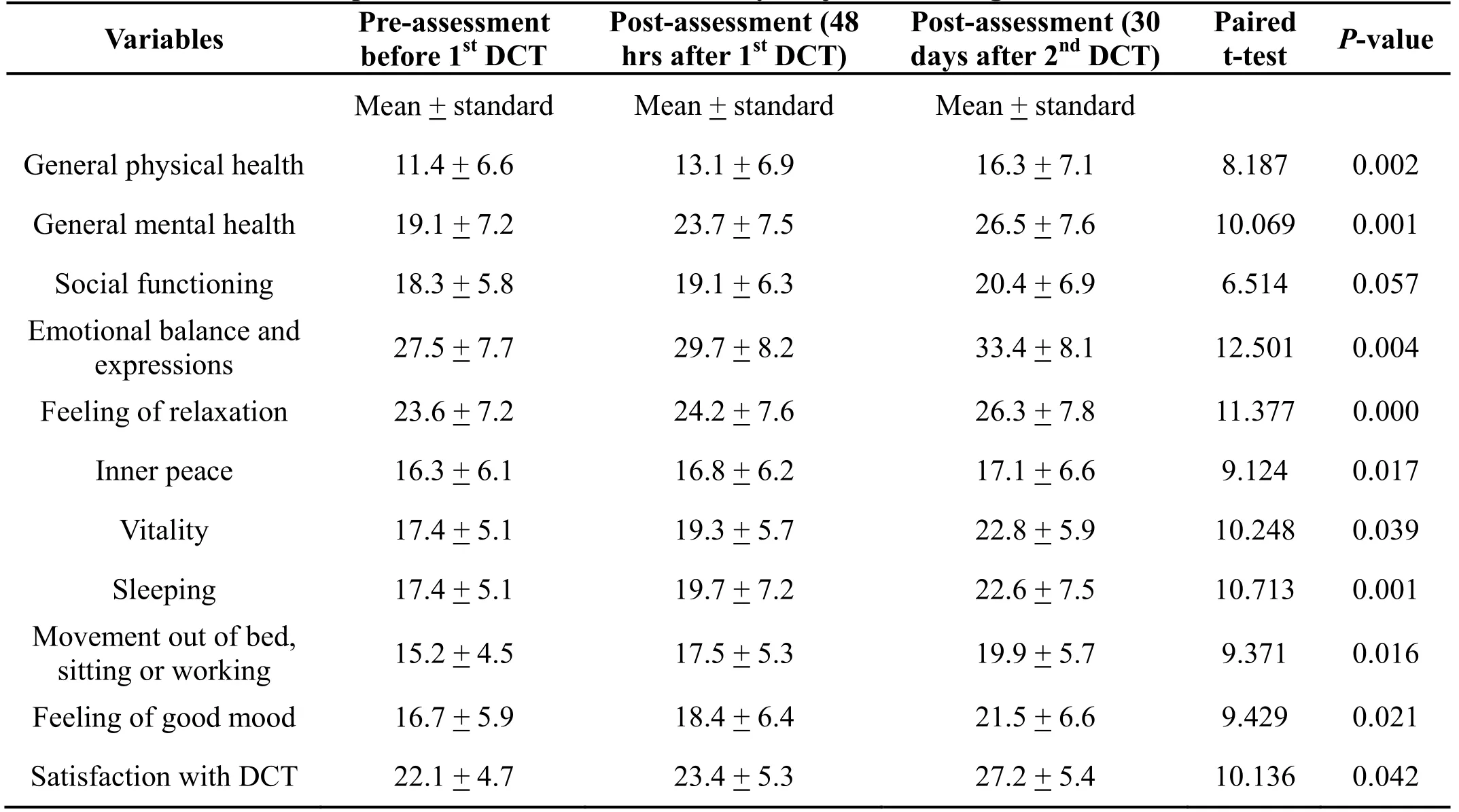
Table 6 Pre-post wellness assessment of study subjects receiving DCT interventions
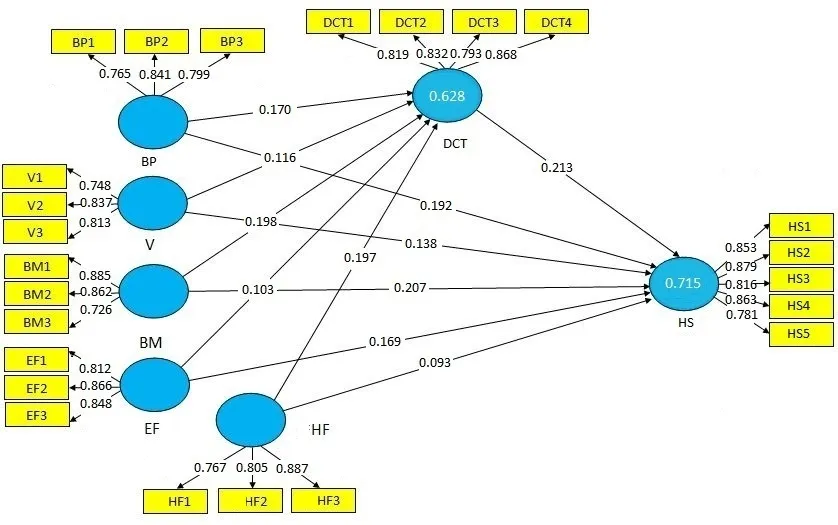
Figure 3 Structural model: Results for DCT and health status
20.33% of the participants reported post DCT complications. Among thirty eight participants, who reported post DCT complication, pain on cupping area was reported by thirteen participants, followed by six participants with restlessness and five participants who reported itchiness due to cupping. However, among remaining fourteen persons who reported complications after DCT interventions, four participants felt discomfort,three participants felt muscle tenderness, two participants felt a light headache, two participants felt dizziness, one participant felt fatigue, and one participant reported low blood pressure and eating problem.
Discussion
Present study’s results show that health perceptions with the sub-constructs of physical feelings and psychological feelings are significantly related to the HS of individuals.These associations are further solidified with the DCT interventions. The present study results show that the health and wellness status of study respondents were improved after receiving DCT treatments. It has been noted that the participants reported significantly positive impacts of DCT interventions on their overall health and wellness which helped them to manage their other daily functions. More precisely, significantly positive improvements are observed for general physical and mental health, emotions and expressions, relaxation,quality of sleep, inner peace, and satisfaction after receiving second DCT intervention as compared to first DCT intervention. Social functioning is not found statistically significant as being reported by the study’s participants; however, it still shows improvement after 1st and 2nd DCT interventions. Hence, the overall quality of life in terms of health and wellness of individuals improved after receiving DCT treatments. These results are in line with some existing studies [42], and wellness notions noted in other literature [43]. After pre and post analysis, the findings of the present study show that movement out of bed, sitting, and working also significantly were improved after 1st and 2nd DCTs.Since these aspects come under routine matters, the present study’s findings support results and discussions in some studies where it is noted that CTs improve clients’management of their daily life matters [44]. However, it is to be noted that the number of DCT interventions and the time period to feel its effects may be helpful in order to appropriately examine the overall health and wellness of people. Participants of the present study were recruited from different places in Faisalabad city for a period of consecutive nineteen days. Hence, this eliminated time and place biases which may improve the efficacy of CTs[42].
DCT interventions and post-assessments show that health and wellness status were positively improved.However, overall health and wellness were improved and reported by the majority of study participants without severe muscle tenderness, discomfort, or restlessness problems. These results are in line with a study conducted by Markowskiet al.[45]. However, a total of thirty eight participants reported minor post DCT complications.More precisely, subjects reported pain on cupping area,restlessness, itchiness, discomfort, and muscle tenderness.Some participants felt light headache, dizziness, and low blood pressure as well as eating problems. These complications might be due to more vacuum pressure inside cups or hard movement of cupping glasses.Although these are minor complications, the physicians and DCT experts need to minimize the side effects of DCTs, which will consequently help to satisfy subjects in tandem with improving their health and wellness.Nevertheless, DCTs were found helpful in bringing overall improvements in respondents’ emotions,behaviors, and other daily activities. WCT was been associated with bringing improvement in the peripheral nervous system by drawing blood flow in order to stimulate skin and muscles which ultimately results in comfort and relaxation [46]. Vacuum generation, skin suction and holding blood flow inside cups under the skin without laceration also proved rest, relaxation, and overall feeling of wellness among present study participants. Hence, the present study’s results extend scientific research from WCT interventions to DCT interventions and proved WCT notions of comfort, rest,and relaxation in order to bring overall health and wellness among healthcare seekers.
Research on T&CM is gaining enormous attention.This is because of the changing interests and preferences of individuals across the globe struggling to improve their quality of life and avoid threats of non-communicable diseases [21]. The research on dry cupping therapies as a part of T&CM has not been fully explored especially in some untapped markets like Pakistan. This research extends the application of T&CM with the help of DCT among the Pakistani health enhancement seekers, i.e.residents, tourists, travelers, visitors, and endeavors to fill theoretical and empirical research gaps in the relevant fields.
Conclusion and recommendation
In conclusion, findings of the present study are found promising by documenting that DCT has a significant importance in order to improve the health perceptions and quality of life preferences of health enhancement seekers.The residents and tourists/travelers in the city of Faisalabad positively reported improvement in their HS after experiencing DCT interventions. DCT interventions are noninvasive with minor post-procedure complications as compared to WCT or other therapies/procedures in the conventional western medical system. Hence, the role of DCT should further be investigated in order to examine behavioral changes among different study population and by conducting multicenter studies. The association of DCT with allopathic treatments should be investigated in order to develop a better understanding and the conceptualization of wellness with alternative therapies.This will ensure to deliver a high quality of life which healthcare consumers endeavor to find across the world.This will help to draw firm evidence of DCT in recent medical systems where some scholars note that alternative health and wellness treatments are preferred by medical tourists and other health travelers in order to manage a healthy lifestyle and live a better quality of life[21]. Moreover, DCT is safe and can easily be managed in clinical trials and home-based settings. Considering the benefits and efficacy of DCT, CTs should not only be practiced by eastern traditional medicine practitioners but allopathic practitioners may benefit from its healing powers. DCT may help allopathic practitioners to treat and satisfy their patients with alternative therapies. It may strengthen the notions of better health and quality of life with the integrated focus of eastern and western medical systems.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. NHS research ethics committee number: 10/H1202/69.
Informed consent
Informed consent was obtained from all individual participants included in the study.
1. Patwardhan B. Ayurveda and integrative medicine:Riding a tiger. J Ayurveda Integr Med 2010, 1:13-15.
2. Nandha R, Singh H. Amalgamation of Ayurveda with allopathy: A synergistic approach for healthy society. International J Oncol Pharm 2013, 7:173-176.
3. Majeed S, Lu C. Changing preferences, moving places, and third party administrators: A scoping review of medical tourism trends (1990-2016).Almatourism 2017, 8: 56-83.
4. Kessler RC, Daris RB, Faster DF. Long term trends in the use of complementary and alternative medical therapies in the US. Ann Intern Med 2001, 135:262-268.
5. Cao H, Han M, Li X,et al.Clinical research evidence of cupping therapy in China: A systematic literature review. BMC Complement Altern Med 2010, 10: 70.
6. Al Bedah AMN, Khalil MKM, Posadzki P,et al.Evaluation of wet cupping therapy: systematic review of randomized clinical trials. J Altern Complement Med 2016, 22: 768-777.
7. Al-Bedah AM, Shaban T, Suhaibani A,et al.Safety of cupping therapy in studies conducted in twenty one century: A review of literature. Br J Med Med Res 2016, 15: 1-12.
8. Mehta P, Dhapte V. Cupping therapy: A prudent remedy for a plethora of medical ailments. J Tradit Complement Med 2015, 5: 127-134.
9. Teut M, Kaiser S, Ortiz M,et al.Pulsatile dry cupping in patients with osteoarthritis of the knee: a randomized controlled exploratory trial. BMC Complement Altern Med 2012, 12: 184.
10. Rozenfeld E, Kalichman L. New is the well-forgotten old: The use of dry cupping in musculoskeletal medicine. J Bodyw Mov Ther 2016,20: 173-178.
11. Al-Bedah AM, Aboushanab TS, Alqaed MS,et al.Classification of cupping therapy: A tool for modernization and standardization. J Complement and Alternative Med Res 2016, 1: 1-10.
12. Nimrouzi M, Mahbodi A, Jaladat AM,et al. Hijamat in traditional Persian medicine: risks and benefits. J Evid Based Complementary Altern Med 2014, 19:128-136.
13. Michael A, Akande TO. Cupping therapy burn in an African. Niger J Plastic Surg 2016, 12: 26-27.
14. Zhao JC, Yu JA, Xian CJ,et al.Burns induced by cupping therapy in a burn center in northeast China.Wounds 2014, 26: 214-220.
15. Al-Balawi AM, Almutairi AH, Alawad AO,et al.Public perceptions of cupping therapy in Tabuk city,Saudi Arabia. Int J Med Sci Public Health 2015, 5:529-533.
16. Rafatpanah H, Hedayati-Moghaddam MR,Fathimoghadam F,et al.High prevalence of HTLV-I infection in Mashhad, Northeast Iran: a population-based seroepidemiology survey. J Clin Virol 2011, 52: 172-176.
17. Fathimoghaddam F, Hedayati-Moghaddam MR,Bidkhori HR,et al.The prevalence of hepatitis B antigen-positivity in the general population of Mashhad, Iran. Hepat Mon 2011, 11: 346-350.
18. Noroozi Seyed Hoseini R, Fathi H.Comparison of mental health, quality of life and emotional intelligence of physical education teachers and other teachers of Kermanshah province. J Sports Manag 2012, 11: 53-75.
19. Davoodi A, Reza Zadeh H, Soomi MH,et al.The impact of self care education on the quality of life in gastric cancer patients after gastrectomy surgery.Med J Tabriz University Med Sci 2012, 1: 48-55.
20. Majeed S, Lu C, Majeed M,et al.Health resorts and multi-textured perceptions of international health tourists. Sustainability 2018, 10: 1063.
21. Majeed S, Lu C, Javed T. The journey from allopathic to naturopathic treatment approach: A scoping review of medical tourism and health systems. Eur J Integr Med 2017, 16: 22-32.
22. Li Z. Attractive forces and risks of international medical tourism: A study based on India. J Chem Pharm Res 2014, 6: 125-127.
23. Qureshi NA, Ali GI, Abushanab TS,et al.History of cupping (Hijama): A narrative review of literature. J Integr Med 2017, 15: 172-181.
24. Saad A. Reviving the cupping therapy “Al-Hijama”through the framework of developing health care tourism in Egypt. J Tour Hosp 2015, 4: 178.
25. Ge W, Leson C, Vukovic C. Dry cupping for plantar fasciitis: a randomized controlled trial. J Phys Ther Sci 2017, 29: 859-862.
26. Farhadi K, Choubsaz M, Setayeshi K,et al.The effectiveness of dry-cupping in preventing post-operative nausea and vomiting by P6 acupoint stimulation. Medine 2016, 95: e4770.
27. Khimani F, Mahmud H, Majeed K,et al.Complementary and alternative medicine:perceptions of medical students in Pakistan. Med Educ Online 2007, 12: 9.
28. Tovey P, Broom A, Chatwin J,et al.Patient assessment of effectiveness and satisfaction with traditional medicine, globalized complementary and alternative medicines, and allopathic medicines for cancer in Pakistan. Integr Cancer Ther 2005, 4:242-248.
29. Shaikh BT, Hatcher J. Complementary and alternative medicine in Pakistan: prospects and limitations. J Evid Based Complementary Altern Med 2005, 2: 139-142.
30. Geissner E. Die Schmerzempfindungsskala-SES.Hogrefe: Go¨ttingen 1996.
31. Bullinger M, Kirchberger I. SF-36 Fragebogen Zum Gesundheitszustand. Handanweisung, Hogrefe,Go¨ttingen, 1998.
32. Herrmann C, Buss U, Snaith RP. Hospital anxiety and depression scale- Deutsche version (HADS-D).1995. HansHuber, Bern.
33. Kolip P, Schmidt B. Der Fragebogen Zur Erfassung ko¨rperlichen Wohlbefindens (FEW16),Konstruktion und erste Validierung. Zeitschrift fu¨r Gesundheitspsychologie 1999, 7: 77-87.
34. Gordon DB, Polomano RC, Pellino TA,et al.Revised American pain society patient outcome questionnaire (APS-POQ-R) for quality improvement of pain management in hospitalized adults: preliminary psychometric evaluation. J Pain 2010, 11: 1172-1186.
35. Lauche R, Cramer H, Choi KE,et al.The influence of a series of five dry cupping treatments on pain and mechanical thresholds in patients with chronic non- specific neck pain--a randomized controlled pilot study. BMC Complement Altern Med 2011, 11:63.
36. Hong SH, Wu F, Lu X,et al.Study on the mechanisms of cupping therapy. Zhongguo Zhen Jiu 2011, 31: 932-934.
37. Chin WW. The partial least squares approach for structural equation modeling. Mahwah, New Jersey,London, 1998.
38. Majeed S, Lu C, Usman M. Want to make me emotional? The influence of emotional advertisements on women’s consumption behavior.Front Bus Res in China 2017, 11: 16.
39. Hair JF, Anderson RE, Tatham RL,et al.Multivariate Data Analysis (5th ed.). 1998.Prentice-Hall International Inc.
40. Fornell C, Larcker DF. Evaluating structural equation models with unob-serviable variables and measurement error. J Mark Res 1981, 18: 39-50.
41. Hair JF, Hult GT, Ringle C,et al.A primer on partial least squares structural equation modeling(PLS-SEM). 2013. Inc: Sage Publication.
42. Lauche R, Langhorst J, Dobos GJ,et al.Clinically meaningful differences in pain, disability and quality of life for chronic nonspecific neck pain - a reanalysis of 4 randomized controlled trials of cupping therapy. Complement Ther Med 2013, 21:342-347.
43. Avicenna. Qanun fi al-Tib Canon of Medicine.Dar-ol-maktab-ol-Elmiyah Press, Beirut 1999,289-301.
44. Lauche R, Cramer H, Hohmann C. The effect of traditional cupping on pain and mechanical thresholds in patients with chronic nonspecific neck pain: a randomised controlled pilot study. Evid Based Complement Alternat Med 2012: 429718.
45. Markowski A, Sanford S, Pikowski J,et al.A pilot study analyzing the effects of Chinese cupping as an adjunct treatment for patients with subacute low back pain on relieving pain, improving range of motion, and improving function. J Altern Complement Med 2014, 20: 113-117.
46. Kim JI, Kim TH, Lee MS,et al.Evaluation of wet-cupping therapy for persistent non-specific low back pain: a randomised, waiting-list controlled,open-label, parallel-group pilot trial. Trials 2011, 12:146.
 Traditional Medicine Research2019年1期
Traditional Medicine Research2019年1期
- Traditional Medicine Research的其它文章
- In vitro evaluation of transdermal permeation effects of Fu’s cupping therapy via six diffusion kinetics models
- A multi-center randomized controlled clinical trial of three-step acupuncture and cupping therapy for cervicogenic headache
- The effect of hot intermittent cupping on pain, stiffness and disability of patients with knee osteoarthritis
- A clinical study on medical cupping for metabolic syndrome with abdominal obesity
- Three-step acupuncture and cupping therapy:an effective approach to treat cervicogenic headache
- Stir up a fire and burn oneself:the secret of fire therapy