
Efficacy of arthroscopic surgery for discoid lateral meniscus injury in knee joint:a self-control study
2019-01-07 09:09:36JianJunMaiBinXuJunTuLeiWu
Jian-Jun Mai ,Bin Xu ,Jun TuLei Wu
1 Department of Sports Trauma and Arthroscopy,First Affiliated Hospital of Anhui Medical University,Hefei,Anhui Province,China
2 Department of Orthopedics,Maanshan People’s Hospital,Maanshan,Anhui Province,China
Abstract
Key words:discoid lateral meniscus; chondral lesion; arthroscope; Lysholm score; knee joint function; adverse reaction; self-control study
INTRODUCTION
Discoid lateral meniscus(DLM)is a rare form of abnormal meniscal morphology with unknown pathogenesis.1-3Congenital developmental stagnation has been widely accepted as the etiology of DLM.4The most common classification of DLM,the Watanabe system,subdivides DLM into three types according to the coverage of the lateral tibial plateau(complete or incomplete type)and whether the meniscus has an abnormal posterior attachment to part of the posterior cruciate ligament(Wrisberg type).The incidence of complete or incomplete type DLM is very high.5-7
If meniscal tearing or instability exists,8patients with DLM injury often have clinical symptoms such as pain,clicking,skelasthenia,muscle-specific atrophy of the quadriceps femoris,and/or joint swelling.9-11DLM is diagnosed if bowtie-like or butter fly knot-like changes of anterior and posterior horns of the meniscus appear on three or more contiguous,5-mm-thick sagittal magnetic resonance images(MRI).12DLM generally has no clinical manifestations and surgical treatment is unnecessary,but surgery should be performed as early as possible if a meniscal tear exists.13-15There is evidence that complete meniscectomy inevitably leads to an increased incidence of osteoarthritis and lateral instability of the knee joint.14At present,meniscal plasty with a preserved stable peripheral edge has been considered effective for DLM repair.16This method can determine the size of repair according to the range of the tear.17Arthroscopic meniscus surgeries aim to create a stable meniscus that provides sufficient cushioning pressure,thus avoiding the recurrence of a tear.18
In the clinic,complete DLM is more prone than incom-plete DLM to tearing19-22and adverse reactions such as joint degeneration and osteochondritis23.Older adult patients with DLM who have chondral lesions often have unsatisfactory therapeutic effects.
The three latest retrospective studies24-26listed in Table 1 were retrieved by thefirst author using an electronic search of the PubMed database for analyzing risk factors of DLM from January 2018 to August 2018.
Study objective
Based on a previous small-sample-size study,this single-center self-control study will include a larger sample size to analyze the efficacy of arthroscopic meniscus surgery in patients and potential risk factors that in fluence surgical efficacy through a 6-18-month follow-up.
SUBJECTS AND METHODS
Study design
A single-center,self-control study(Figure 1).
Study setting
Department of Sports Trauma and Arthroscopy,First Affiliated Hospital of Anhui Medical University of China.
Study population
Data collection
Baseline data(age,sex,course of disease,and lesion region),disease classification(Watanabe classification:complete type,incomplete type; Outerbridge grade of chondral lesion),imaging data(MRI of the knee joint),Lysholm score,and adverse reactions will be collected from patients who will receive treatment at the Department of Sports Trauma and Arthroscopy,First Affiliated Hospital of Anhui Medical University,China from December 2018 to December 2019.Case Report Forms containing these data will be input to a secure computer for later use.
Eligibility criteria
Inclusion criteria
Patients presenting with all of the following criteria coassented by experts will be considered for inclusion:
·One or more symptoms of discoid meniscus injury,such as knee joint swelling and discomfort,joint clicking,limping,and noose;
·Meniscal injury confirmed by MRI of the knee joint; grade 2 and grade 3 injury described by Stoller et al.; grade 2 injury exhibiting a linear high-intensity signal that does not extend to the articular surface; or grade 3 injury exhibiting linear or diffuse high-intensity signal that extends to the articular surface.All these indicate meniscal tear27;
·Arthroscopic meniscus surgery reveals DLM with meniscal tear that needs surgical treatment.
Exclusion criteria
Patients meeting any of the following conditions assented by experts will be excluded:
·Bilateral knee joint needs surgical treatment;
·Severe osteoarthritis(obviously narrow joint space);

Table 1:Three latest retrospective studies regarding risk factors of discoid lateral meniscus(DLM)published in 2018

Figure 1:Study flow chart.
·Ligament injury and intra-articular valgus deformity that leads to instability or imbalance of soft tissue of the knee joint,which in fluences motion scoring;
·Fracture,bone disease,or malignant tumor that in fluences motion scoring.
Grouping and blinding
Double-blind grouping and allocation concealment will not be used in this study.Instead,a self-control design will be used.Lysholm scores will be used to evaluate surgical efficacy.Patients will be assigned to an excellent-and-good group(Lysholm score ≥ 85)and a poor group(Lysholm score < 85)according to surgical efficacy.Subjects who are responsible for arthroscopic examination and radiologists who read MRI will be blinded to the study protocol.
Arthroscopic meniscus surgery
Preoperative preparation
Before surgery,patients presenting with DLM tear confirmed by MRI of the knee should be ensured not to have rheumatism,rheumatoid diseases,or septic arthritis.Patients should be instructed to strengthen the function of the knee muscle with exercise.
Surgical method
The patient will be asked to lie supine on the operating table.After tracheal intubation and general anesthesia,a pneumatic tourniquet will be in flated.The skin will be dissected at a site 1.5 cm below the patella on the lateral side of the knee joint and 1 cm from the bilateral patellar tendon.An arthroscope will be inserted into the incision at an angle of 30° from the skin.The superior sac,patellofemoral joint,lateral crypt,lateral joint space,intercondylar fossa,and medial joint space will be sequentially explored.DLM will be identified.Watanabe classification,region and type of meniscal tear,and degree of lateral femoral condyle cartilage injury will be determined.A stable meniscal peripheral edge with a width of 6-8 mm and stable meniscal anterior and posterior horns will be preserved,as possible.Softened articular surface will be trimmed.The articular cavity will befinally rinsed.All residual debris will be aspirated.After incision suture,two ampules of sodium hyaluronate(Shandong Bausch & Lomb Pharmaceutical,Shandong Province,China; Specification:20 mg in 2 mL)will be injected.Finally,a sterile dressing will be placed on the incision and a pressure bandage will be used.If the lesion is located in the anterior body,it will be sutured.If the meniscal tear extends to the posterior horn of the meniscus,subtotal meniscectomy will be performed(Figure 2).
Postoperative management
After returning to the ward,the patient will wear a knee joint brace and apply ice packs to the affected limb.After 24 hours,patients will be asked to perform active and passive knee flexion,and extension exercise under brace protection.Starting from 1 week after surgery,sodium hyaluronate will be injected into the articular cavity(Shandong Bausch & Lomb Pharmaceutical),one ampule per day for four successive days.Sutures will be removed 2 weeks after surgery.The time until weight-bearing walking will be determined according to the degree of chondral lesion.All surgeries will be performed by senior orthopedic surgeons titled Associate Chief Physician or higher.Patients will be periodically followed up for 6-18 months through clinic visits.
MRI examination of the knee

Figure 2:Morphological change in discoid lateral meniscus(DLM)observed under the arthroscope.
Before surgery and at the last follow-up,the knee will be scanned using a 3.0-T MRI scanner(Signa HDx 3.0 T,GE Healthcare,Milwaukee,WI,USA)with the following MRI parameters:echo train length index = 16; repetition time/echo time = 2360/62.2 ms; flip angle = 90°;field of view = 15 cm ×15 cm; layer thickness = 6.0 mm; layer spacing = 2.0 mm; number of scanning layers = 15; sampling bandwidth = 41.7 kHz.
Outcome measures
Primary outcome measure
Change in excellent-and-good rate of Lysholm score that reflects knee joint function measured at the last follow-up:knee joint function will be evaluated before surgery and at the last follow-up according to the Lysholm knee scoring scale.The total score ranges from 0-100,with a score of > 95 indicating excellent,94-85 good,84-65 fair,and < 65 poor.Excellentand-good rate = number of patients with excellent or good knee joint function(Lysholm score > 85)/ total number of patients × 100%.28
Secondary outcome measures
·Lysholm score of knee joint measured before surgery and at the last follow-up:scoring criteria are the same as above.
·Outerbridge grade of chondral lesion before surgery and at the last follow-up:grade I,cartilage with local softening and swelling; grade II,a partial-thickness defect with vertical “shark scorpion”-likefissures on the surface that exceed 1.25 cm in diameter; grade III,fissuring to the level of subchondral bone,similar to “crab meat” with a diameter of approximately 1.25 cm; grade IV,early osteoarthritis,exposure of subchondral bone with invasive change,joint involvement(in most cases involving the lateral side).29
·Knee joint morphology by MRI before surgery and at the last follow-up:knee joint will be scanned using a MRI scanner to observe the morphology of the meniscus.All patients will be scanned using the same MRI scanner.
·Changes in age,sex,lesion region,and course of disease before surgery:prior to surgery,mean age,sex(male/female),lesion region(left or right side),and course of disease(main record of patient's complaints from medical records)will be recorded.
·Incidence of adverse reactions at the last follow-up:postoperative adverse reactions include knee joint degeneration,osteochondritis,meniscal cyst,reactive synovitis,and knee stiffness.The incidence of adverse reactions will be calculated.
Timing of primary and secondary outcome measures is shown in Table 2.
Adverse events
Adverse reaction information will include the attribution of adverse events,time of onset,time of termination,severity,frequency,treatment or not,and treatment details if exist.Clinical physicians will manage adverse reactions according to the patient's condition.The program for prevention and management of medical accidents will be commenced if necessary.
Sample size
A preliminary study with a small sample size was performed from April 2015 to September 2016.In this preliminary study,15 patients with DLM injury underwent surgery.Knee joint function was evaluated using Lysholm scoring,with excellent efficacy in 32 patients,good in 61 patients,fair in 18 patients,and poor in four patients.The excellent-and-good rate of knee joint function evaluated by Lysholm scores was 80.9%.
We hypothesized that the excellent-and-good rate of knee joint function evaluated by Lysholm scoring was 90%,30assumingβ= 0.1,power = 90%,α= 0.05(two-sided),and an effective sample size ofn= 163 calculated using PASS 11.0 software(PASS,Kaysville,UT,USA).Assuming a participant loss rate of 20%,we will require a sample size ofn= 196 patients in this study.
Statistical analysis
Data description
All data will be statistically processed using SPSS 22.0 software(IBM,Armonk,NY,USA).Measurement data will be expressed as means,standard deviations,medians,minimum and maximum values,and upper and lower quartiles.Count data will be expressed as numbers and percentages.
Selection of statistical methods
Excellent-and-good rates of knee joint function evaluated by Lysholm score,sex,course of disease,lesion region,and the incidence of adverse reactions will be compared between the wo groups using Pearson's chi-square test.Count data in the same group will be compared between before surgery and at the last follow-up using the McNemar test.Outerbridge grade will be compared between the two groups using the Kruskal-Wallis H method.Lysholm score and age will be compared between the two groups at the same time point using a twosamplet-test(normally distributed data)or Mann-WhitneyUtest(non-normally distributed data).Measurement data before surgery and at the last follow-up in the same group will becompared using a pairedt-test(normally distributed data)or Wilcoxon signed-rank test(non-normally distributed data).Risk factors that in fluence curative effects will be analyzed using logistic regression analysis.Odd ratio(OR)and 95%CIvalues will be calculated.An inspection level ofα= 0.05(bilateral)will be considered.
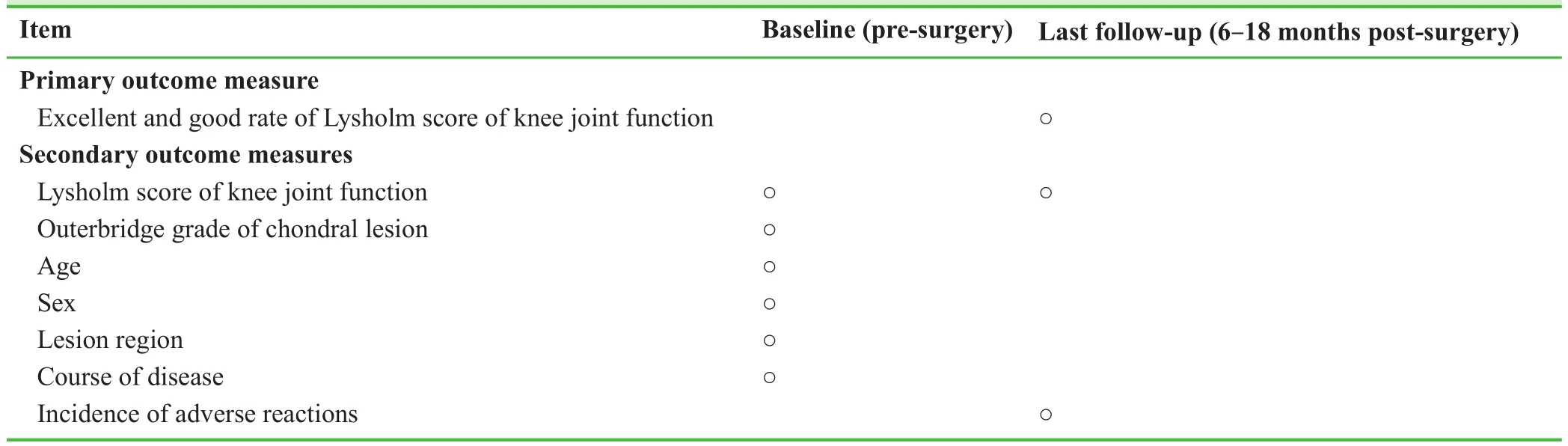
Table 2:Schedule of primary and secondary outcome measures
Data sets
Patients included in thefinal analysis are mainly the population assigned to the per protocol set.
Data collection and management
Data collection
Case report forms will befilled by the investigators accurately,completely,and on time.After accuracy confirmation and signature by the principle investigator,only the principal investigator or his authorized personnel has the right to make alterations.Alterations will be signed and dated by the principle investigator or authorized personnel.
Data management
According to items in the Case Report Form,Epi-Data 3.0 software will be used to establish the corresponding entry procedure.Logical review qualification conditions at the time of entry will be set,the database will be run,and a database system dedicated to this study will be established.Written records will be transferred to an electronic format by two professional staff members using a double data entry strategy.
Audits
Independent Data Monitoring Committee composition
The role and responsibilities of the Independent Data Monitoring Committee will be relative to the project steering committee,including doctors with related professional backgrounds,epidemiologists,radiologists,statisticians,clinical trial managers,and ethics experts.
Investigator qualification
Physicians responsible for imaging examination and arthroscope examination must have undergone professional training and have 5-10 years of experience in this researchfield.These physicians should have acquired a professional title of Associate Chief Physician or higher.
Auditing
Monitors will visit the trial institute regularly or carry out clinical quality audit work according to the actual situation.Monitors will report the progress of the trial to the Ethics Committee every 2 months and update the trial progress in the registration database.
Compensation to patients
Patients included in the clinical trial will be monitored and followed up,and may undergo close examinations in our hospital without charge.In addition,they will be able to receive transportation and registration fees for admission examination.
Ethics and dissemination
Ethical approval
This study was approved by Medical Ethics Committee,First Affiliated Hospital of Anhui Medical University of China(approval No.PJ2018-02-03)on February 5,2018(Additionalfile 1).The study protocol will be performed in accordance with theDeclaration of Helsinki.The version of study protocol will be 1.0.The manuscript was prepared according to the requirement of Transparent Reporting of Evaluations with Nonrandomized Designs(TREND)(Additionalfile 2).
Informed consent
Patients participating in the study and their family members should participate voluntarily.All patients should fully consent to the experimental process and sign an informed consent form on the premise of fully understanding the treatment plan(Additionalfile 3).
Dissemination
Results will be disseminated through presentations at scientific meetings and/or by publication in a peer-reviewed journal.Anonymized trial data will be published at www.figshare.com.
RESULTS
Small-sample-size study
A total of 115 patients with DLM injury who underwent arthroscopic meniscus surgery from April 2015 to September 2016 were included in a preliminary study.These patients were followed up for 6-18 months.
Baseline information
There were no significant differences in sex,lesion region,or Outerbridge grade of chondral lesion between the excellentand-good group and poor group(P> 0.05).However,significant differences in age and course of disease were observed between these two groups(P< 0.05)(Table 3).

Table 3:Baseline information of 115 patients with DLM
Lysholm scoring of knee joints
Lysholm scores for the knee joints of 115 patients with DLM injury before surgery and at the last follow-up were 65.8 ±9.39 and 89.15 ± 7.45,respectively,and there was a significant difference in Lysholm scores before surgery and at the last follow-up(P< 0.05).Knee joint function as assessed by Lysholm scoring was excellent in 32 patients,good in 61 patients,fair in 18 patients,and poor in 4 patients.The excellent-and-good knee joint function was observed in 93 patients,while poor knee joint function was observed in 22 patients,thus yielding an excellent-and-good rate of knee joint function of 80.9%.
Univariate and multivariate analysis of preoperative situation and postoperative outcomes in patients with DLM injury undergoing arthroscopic surgery
Univariate analysis revealed that there were significant differences in age,course of disease,and Outerbridge grade of chondral lesion between the excellent-and-good group and poor group(P< 0.05).However,no significant differences in other indices were observed between these two groups(P> 0.05; Table 4).
Logistic regression analysis of these three independent variables revealed that age,course of disease,and Outerbridge grade of chondral lesion are the risk factors that in fluence the efficacy of arthroscopic surgery in the treatment of DLM injury(Table 5).
DISCUSSION
Analysis of small-sample-size study
Age factor
The results of the small-sample-size study revealed that the onset age of patients with DLM injury was 5-78 years,with an average age of 35.65 ± 15.96 years,generally younger.However,the average age of patients with excellent or good efficacy was 33.28 ± 16.03 years,while that of patients with poor efficacy was 45.68 ± 11.30 years.Younger patients have a higher satisfactory rate.This possibly occurs because young people have strong tissue regeneration ability,and a stable and active meniscal edge can form if there is normal blood supply in the meniscal stump.There is a larger possibility,namely,the course of disease and knee joint degeneration.
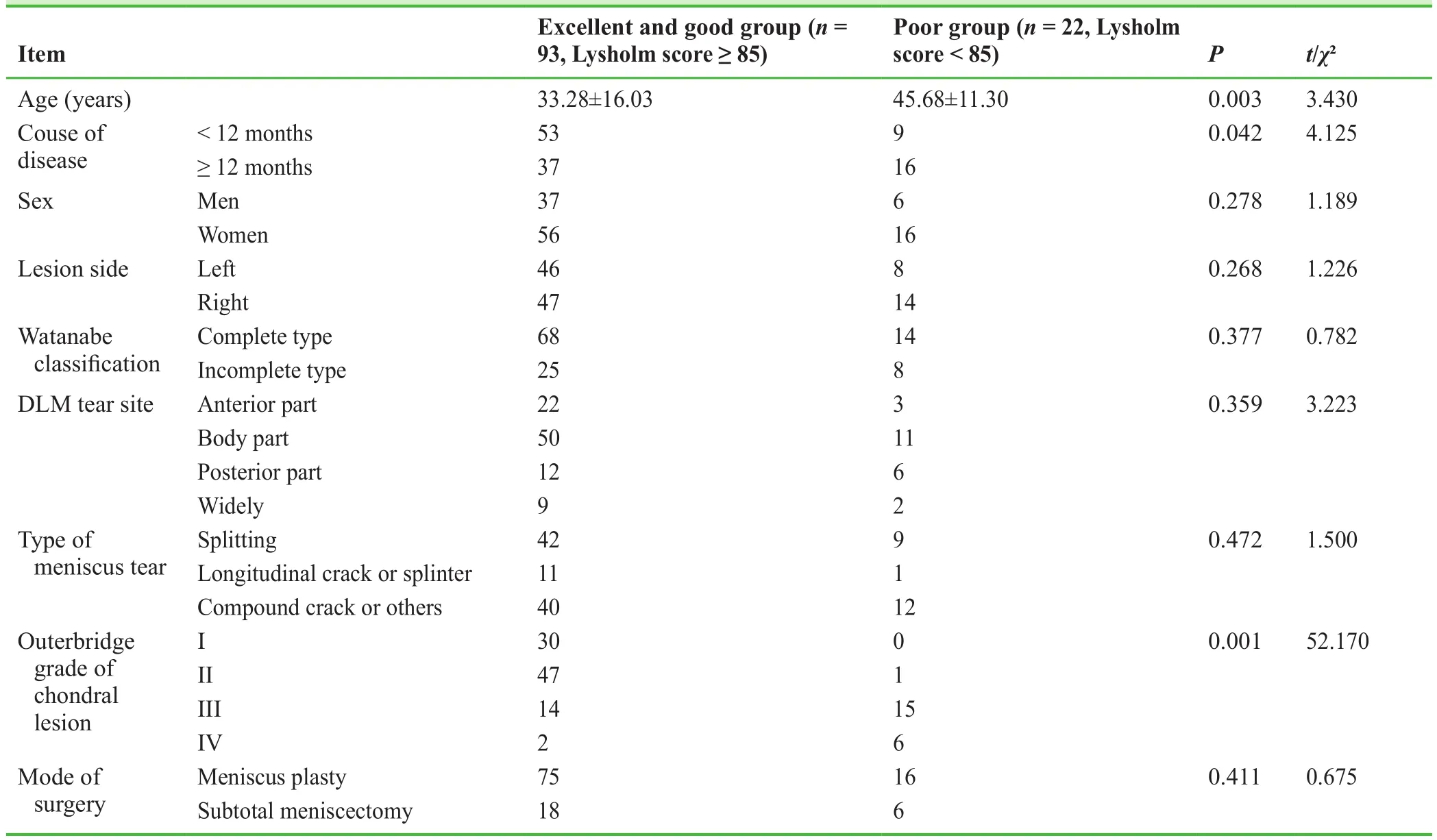
Table 4:Univariate analysis of factors that influence efficacy in two groups

Table 5:Multivariate logistic regression analysis of the risk factors that influence the efficacy of arthroscopic surgery
DLM tissue structural differences and chondral lesions
The meniscus is a mesh-like structure composed offibrous chondrocytes and type I collagenfiber.When the meniscus is subjected to large axial pressure,its thickness can be reduced by half because the unique meniscal structure can cushion the extrusion.In addition,pressure can be evenly dispersed to the cartilage surface of the tibial plateau.Thus,the meniscus is not easily damaged and its overall stability can be maintained.In the past,most scholars did not consider DLM and normal meniscus to differ in terms of tissue structure.However,current studies have found distinct structural differences between DLM and normal meniscus tissue.A normal meniscus is more morphologically and structurally adaptable than the DLM.Under the same pressure,the DLM is more prone to stress concentration and uneven distribution of joint fluid,resulting in meniscus injury.
Novelty of this study
This study will confirm the exact efficacy of arthroscopic surgery for DLM injury.Based on the results of a preliminary small-sample-size study,age and soft tissue injury are related to postoperative Lysholm score.Older adult patients with DLM injury who have severe chondral lesion have poor outcomes of arthroscopic meniscus plasty compared with those without DLM injury.Potential explanations are as follows:(1)DLM is similar to developmental disorders in that it has a long course of disease.With growth development,the disease condition gradually aggravates.If recurrent knee pain occurs,MRI of the knee is necessary.Surgical treatment is recommended for patients with DLM tear.If there is no DLM tear,conservative treatment should be given and regular MRI examination is necessary.(2)A large deformed meniscus leads to an increase in the lateral space of the knee joint.Meniscus plasty only restores the meniscus to a normal shape.However,the surrounding soft tissue does not adapt to this change,resulting in instability and pain in the lateral aspect of the knee joint,which in fluences the curative efficacy.
Limitations of this study
There are several limitations of this study.(1)The last followup time of for outcome measurements is 6-18 months,and the time interval between data collection is large.(2)Regarding DLM in the small-sample-size retrospective study,a normal control group containing patients without meniscus injury should be included.(3)Patient assignment according to Watanabe classification and arthroscopic observation is in fluenced by subjective factors,which may lead to biased results.(4)Arthroscopic surgery is performed at the same department under the same criteria,but postoperative rehabilitation is not managed by the same physician,which possibly in fluences the postoperative scoring of knee joint function.(5)A poor knowledge of statistics and small sample size may lead to biased results of univariate analysis and logistic regression analysis.(6)A long-term follow-up and a secondary arthroscopic examination should be performed.
Clinical significance
This study aims to validate that(1)arthroscopic surgery is effective for DLM injury;(2)age and Outerbridge grade of chondral lesion are closely related to the efficacy of arthroscopic meniscus plasty(surgical treatment is recommended as early as possible for DLM with clinical symptoms); and(3)arthroscopic meniscus plasty is unlikely to be ideal for older adult patients with severe chondral lesion.Taken together,future studies with longer follow-ups should be performed to investigate whether subtotal meniscectomy and meniscus plasty differ in curative efficacy.
Additionalfiles
Additionalfile 1:Hospital ethics approval(Chinese).
Additionalfile 2:TREND checklist.
Additionalfile 3:Informed consent documentation(Chinese).
Author contributions
Study design and authorization:JJM; patient recruitment:BX and JT;data collection and analysis:JJM,JT,and LW.All authors approved thefinal version of this manuscript..
Conflicts of interest
The authors have no con flicts of interest to declare.
Financial support
None.
Institutional review board statement
The study was approved by the Ethical Review Board of First Affiliated Hospital of Anhui Medical University(approval No.PJ2018-02-03)on February 5,2018 and well be performed according to theDeclaration of Helsinki.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.In the form,the patients have given their consent for their images and other clinical information to be reported in the journal.The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity,but anonymity cannot be guaranteed.
Reporting statement
This study followed the Transparent Reporting of Evaluations with Nonrandomized Designs(TREND)statement.
Biostatistics statement
The statistical methods of this study were reviewed by the biostatistician of First Affiliated Hospital of Anhui Medical University of China.
Copyright license agreement
The Copyright License Agreement has been signed by all authors before publication.
Data sharing statement
Individual participant data that underlie the results reported in this article,after deidentification(text,tables,figures,and appendices).Data will be available immediately following publication,with no end date.Results will be disseminated through presentations at scientific meetings and/or by publication in a peer-reviewed journal.Anonymized trial data will be available indefinitely at www.figshare.com.
Plagiarism check
Checked twice by iThenticate.
Peer review
Externally peer reviewed.
Open access statement
This is an open access journal,and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License,which allows others to remix,tweak,and build upon the work non-commercially,as long as appropriate credit is given and the new creations are licensed under the identical terms.
 Clinical Trials in Orthopedic Disorder2018年4期
Clinical Trials in Orthopedic Disorder2018年4期
- Clinical Trials in Orthopedic Disorder的其它文章
- Efficacy of silver needle acupuncture combined with muscle relaxation in the treatment of capulohumeral periarthritis:study protocol for a prospective,single-center,randomized,parallel-controlled trial
- Hemostasis following local versus intravenous tranexamic acid in patients undergoing posterior open reduction and internalfixation of thoracolumbar fractures:study protocol for a parallel-group,randomized controlled trial
- Efficiency of tight monitoring by nurse practitioners in rheumatoid arthritis patients in remission after treatment with rituximab:study protocol for a randomized,open-label,controlled trial
- Clinicopathological characterization of long bone non-union:a prospective cross-sectional study
- Local anesthetic infiltration before open reduction and internalfixation for ankle fracture:a single-blind randomized controlled study
- Ultrasound-guided supine lumbar plexus block versus iliac fascia block for analgesia in older adult patients undergoing hip replacement:a randomized controlled trial