
Pharmacodynamic profiling of optimal sulbactam regimens against carbapenemresistant Acinetobacter baumannii for critically ill patients
2018-06-30 02:37:52WeerayuthSaelimWichaiSantimaleeworagunSudaluckThunyaharnDhitiwatChangpradubPirapornJuntanawiwat
Weerayuth Saelim, Wichai Santimaleeworagun, Sudaluck Thunyaharn, Dhitiwat Changpradub, Piraporn Juntanawiwat
1Department of Pharmacy, Faculty of Pharmacy, Silpakorn University, Nakhon Pathom, 73000, Thailand
2The College of Pharmacotherapy of Thailand, The Pharmacy Council, Nonthaburi, 11000, Thailand
3Faculty of Medical Technology, Nakhonratchasima College, Nakhon Ratchasima, 30000, Thailand
4Division of Infectious Diseases, Department of Medicine, Phramongkutklao Hospital, Bangkok, 10400, Thailand
5Division of Microbiology, Department of Clinical Pathology, Phramongkutklao Hospital, Bangkok, 10400, Thailand
6Antibiotic Optimization and Patient Care Project by Pharmaceutical Initiative for Resistant Bacteria and Infectious Diseases Working Group
1. Introduction
Acinetobacter baumannii(A. baumannii) is a Gram negative coccobacilli that can cause nosocomial infections, such as respiratory tract infection, bacteremia, urinary tract infections, post-surgical meningitis and intra-abdominal infections[1].A. baumanniiis an emerging carbarpemem-resistant pathogen, becoming a global threat[2]. Carbapenem-resistantA. baumannii(CR-AB) has several resistance mechanisms, including enzyme production, loss of porins, an efflux pump and a change of penicillin binding protein[3].In Thailand, CR-AB is the most common causative pathogen of nosocomial pneumonia in tertiary care hospitals[4]. CR-AB has been reported to be the most prevalent pathogen in intensive care units in several studies[5,6]. In addition, colistin, sulbactam, and tigecycline are only major treatment options for CR-AB infection[7].
Colistin and tigecycline have good activity against CR-AB.Two studies in Thailand found more than 90% of CR-AB isolates were susceptible to colistin and tigecycline[8,9]. However, the pharmacokinetic properties and toxicities of colistin and tigecycline have limitations. Colistin poorly penetrates some tissues/organs and is nephrotoxic[10,11]. Tigecycline has a large volume of distribution resulting in a low serum concentration[12], so caution should be used in treatingA. baumanniibacteremia with tigecycline[13]. Since 2013,the US Food and Drug Administration has warned increased risk of death among ventilator-associated pneumonia patients with MDRAB treated with tigecycline[14,15].
Sulbactam is a β-lactamase inhibitor with activity against CR-AB.Sulbactam is not highly protein bound and penetrates most infected organs with adequate concentrations[16]. Sulbactam can be given in doses as high as 12 g daily without adverse reactions[17]. According to the 2016 guidelines recommended by the Infection Diseases Society of America/American Thoracic Society, sulbactam remains the drug of choice to treat MDR-AB pneumonia[18].
However, sulbactam is one of the β-lactam antibiotics. β-lactam antibiotics have augmented renal clearance and a large volume of distribution may cause inadequate tissue concentration[19]. Sulbactam shows a time-dependent bactericidal action at a percentage of the exposure time. When sulbactam is active, the free drug concentration remains above the minimum inhibitory concentration (%fT>MIC)in pharmacokinetic pharmacodynamic (PKPD) targets[20]. The Monte Carlo Simulation is a technique that randomly selects a pharmacokinetics parameter value from its distribution. That process is repeated many times to generate the pharmacokinetic parameter value incorporated with the structural pharmacokinetics model to predict the appropriate dosing regimen achieving the PKPD targets[21].
Thus, the aim of this study is to determine the pharmacodynamics of sulbactam by determining its MIC. It also aims to develop a potential dosage regimen to achieve PKPD targets using the probability target of attainment (PTA) and the cumulative fraction of response (CFR) for CR-AB treatment of critically ill patients.
2. Materials and methods
2.1. Bacterial isolates
The study was conducted at Phramongkutklao Hospital in Bangkok,Thailand, a 1 200-bed tertiary care center, from January 2014 to December 2015. All clinical isolates of CR-AB obtained from patients were included in the study. Each isolate was grown in tryptic soy broth containing 20% glycerol and kept at -70 ℃ until used.
2.2. Determination of multidrug-resistant isolates
CR-AB was identified using the disk diffusion test and defined as resistance to carbapenems [imipenem (10 μg) or meropenem(10 μg)][22]: the other antibiotics used during this test were:aminoglycosides [gentamicin (30 μg) or amikacin (30 μg)],antipseudomonal penicillins [piperacillin/tazobactam (100 μg/10 μg)], cephalosporins [ceftazidime (30 μg) or cefepime (30 μg)],sulfa drugs [trimethoprim-sulfamethoxazole (1.25 μg/23.75 μg)] and fluoroquinolones [ciprofloxacin (5 μg)]. The methods used followed the Clinical and Laboratory Standards Institute, guidelines, version 2017[23]. Isolates with a clear zone ≥11 mm to colistin (5 μg) were interpreted as susceptible.
2.3. MIC determination of sulbactam
The MIC of sulbactam was determined using the agar dilution method with Müller-Hinton agar (Oxiod) plates. The serial sulbactam (Wago, Japan) concentrations were freshly prepared between 1 and 1 024 μg/mL. A quality control strain,Escherichia coliATCC 25922 (Department of Medical Sciences Culture Collection,Bangkok, Thailand) was used[23]. This study investigated MIC range,MIC50, and MIC90 of sulbactam against CR-AB. MIC range was defined as a list; the MIC value was just the difference between the largest and smallest values. MIC50 and MIC90 values were defined as the lowest concentration of sulbactam at which 50% and 90% of the isolates were inhibited, respectively.
2.4. Pharmacokinetic pharmacodynamic model study
All pharmacokinetic parameters obtained from published studies of critically ill patients were collected[24,25]. The concentration versus time was studied using a two-compartment model for critically ill patients and a one-compartment model for critically ill patients who received continuous renal replacement therapy. The pharmacokinetic and pharmacodynamic properties of sulbactam were represented by the percentage of free drug time above the MIC during the interval time (%fT>MIC). The PKPD goal was defined as 40% to 60%fT>MIC which was the good outcome related to the efficacy[20].Dosage simulations were conducted using various dosages per day and dosage intervals at durations of infusion.
2.5. Monte Carlo Simulation
The PKPD investigation was conducted using a 10 000-subject Monte Carlo Simulation (Oracle Crystal Ball Classroom Faculty Edition-Oracle 1-Click Crystal Ball 201, Thailand). The Monte Carlo Program used to calculate %fT>MIC for intravenous dosage regimens of sulbactam depended on the linear pharmacokinetic behavior of the agent.
The PTA was defined by how likely a specific drug dose reached a target PKPD index (fT>MIC )[26]. In the present study, a target PKPD index was 40% and 60%fT>MIC. The CFR was the probability of drug dose covering a specified bacterial population[26]. Our bacterial population was the MIC of sulbactam among CR-AB isolates obtained from patients.
CFR was calculated by the cumulative fraction of proportional bacteria of each sulbactam MIC multiplied by PTA of each sulbactam MIC. Dosing regimen that reached above 80% of PTA and CFR was considered the optimal dosage for documented therapy and empirical therapy, respectively.
This study was approved by the institutional review board of the Royal Thai Army Medical Department and Phramongkutklao Hospital,Bangkok, Thailand (approval No. Q014h/59 issued on 24 November 2016).
3. Results
3.1. Characteristics and antimicrobial susceptibilities of CRAB
One hundred eighteen isolates of CR-AB were collected during the study period. Seventy-one percent of the isolates were from blood, 17% from the skin and soft tissue, 6% from intra-abdominal specimens, and 6% from other sources. Seventy-seven percent of the isolates were obtained from sterile sites. Using the disk diffusion method, most CR-AB isolates (90%) in our study were found to be resistant to gentamicin, amikacin, piperacillin/tazobactam,ceftazidime, cefepime, and ciprofloxacin, making them extensively drug-resistantA. baumannii. Of all the study isolates, 100% were susceptible to colistin and 91.7% were susceptible to tigecycline.
3.2. Minimum inhibitory concentrations of study isolates
The MIC range, MIC50, and MIC90 for sulbactam against studied isolates were 8 to >1 024 μg/mL, 64 μg/mL, and 192 μg/mL, respectively. Each MIC value of sulbactam included 8 μg/mL(0.8%), 16 μg/mL (5.1%), 32 μg/mL (11.9%), 64 μg/mL (42.4%), 80 μg/mL (15.3%), 96 μg/mL (5.1%), 128 μg/mL (7.6%), 192 μg/mL(5.1%), 256 μg/mL (0.8%), 512 μg/mL (3.4%), and >1 024 μg/mL(2.5%).
3.3. PTA
The PTA for the different sulbactam regimens at specific MICs,with targets of 40%fT>MIC and 60%fT>MIC is shown in Figures 1A and 1B for critically ill patients. Figures 1C and 1D indicate PTA among critically ill patients with CRRT. Among critically ill patients, for pathogens with a MIC of 4 μg/mL, all dosage regimens achieved the PTA target. However, only a sulbactam dosage of 12 g intravenous daily using 2-4 h infusion or continuous infusion that covered for isolates with a sulbactam MIC of 96 μg/mL, met the PTA at 40% and 60%fT>MIC. None of all sulbactam dosage regimens reached the PTA target for critically ill patients with CRRT.
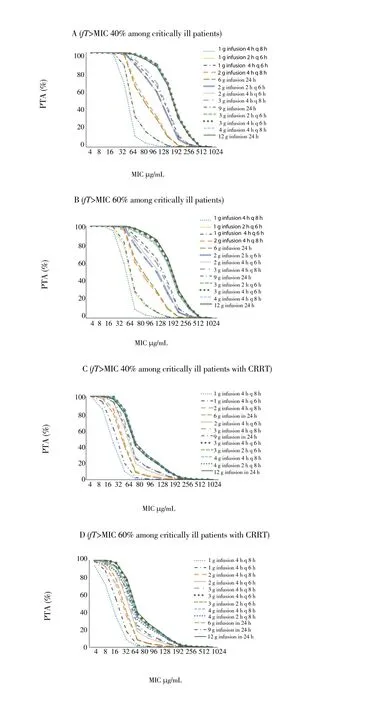
Figure 1. PTA for different sulbactam regimens at specific MICs, with targets of 40% fT>MIC and 60% fT>MIC.
3.4. CFR
Using a CFR >80%, only 4 drug regimens were determined to be appropriate for sulbactam: 3 g infused over 2 h given every 6 h, 3 g infused over 4 h given every 6 h, 12 g infused over 24 h given every 24 h and 4 g infused over 4 h given every 8 h (Table 1). However,none of the studied regimens gave a CFR >80% among patients with CRRT.
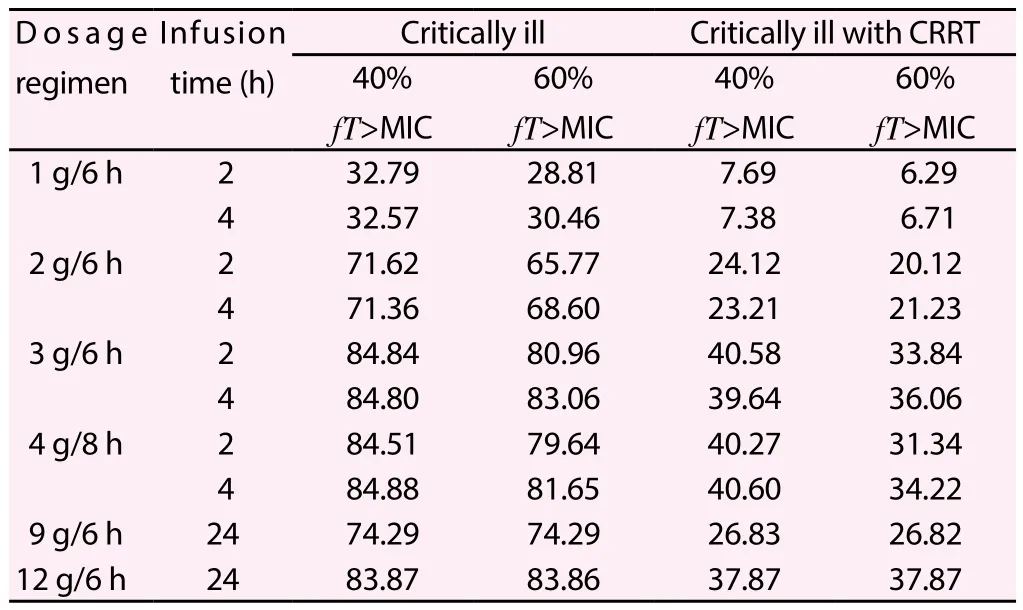
Table 1 Cumulative fraction of response of sulbactam with various drug regimens (%).
4. Discussion
CR-AB is the leading causative pathogen presenting the high mortality rate (73.3%) among critically ill patients[27]. Colistin is the agent most commonly used to treat MDR-AB and extensively drugresistantA. baumannii[28]. In our study, all isolates were susceptible to colistin. However, colistin has nephrotoxicity and poor tissue penetration that limits its usefulness[10,11]. Sulbactam has been purported be a good option to treat CR-AB[29].
With our study, MIC50, and MIC90 values of sulbactam against CR-AB were 64 μg/mL and 192 μg/mL, respectively. In Thailand,two studies performed at Siriraj Hospital[30] and at Queen Sirikit National Institute[31] showed values of MIC50/MIC90 at 32/32 and 16/89.6 μg/mL, respectively. However, unlike other related studies conducted in Thailand, the MIC50 and MIC 90 in the present study presented higher than ever before. These distinguished MIC results might be explained because almost CR-AB isolates in our study comprised extensively drug-resistantA. baumanniiand more than one half of isolates (60%) was obtained from critically ill patients at the ICU ward of a university-affiliated hospital.
Generally, the pharmacokinetics of sulbactam among critically ill patients differed from the general population in the aspects of volume of distribution (Vd). The reported Vd values in Thai healthy volunteers were 3.69 liters[32] while among critically ill patients,Vd of sulbactam were 14.56 liters[24]. The larger Vd values among critically ill patients effect lower serum sulbactam levels. The inadequate sulbactam concentration might be resolved by using a higher sulbactam dose and prolonged or continuous infusion as in our recommended dose of sulbactam at 12 g daily regimens. Our suggestion was similar to the results from reporting that 12 g of sulbactam daily could be achieved at the desired PTA[24].
Sulbactam is unavailable as a single agent in Thailand. Only sulbactam in combination with cefoperazone or ampicillin is available. A sulbactam dose of 12 g daily in a combination form with cefoperazone or ampicllin might result in adverse drug reactions.Thus, patients complying with a high dose of sulbactam should be closely monitored. However, several related studies have indicated that sulbactam in combination with colistin, fosfomycin or imipenem could reduce the MIC of sulbactam against CR-AB[33-35]. Thus, the beneficial synergism of a sulbactam combination might be necessary toward the increasing PTA and CFR targets.
Our study has some limitations. First, the isolates of the CRAB were from MIC distributions at a university-affiliated hospital which might be dissimilar when taken from other types of hospital.Second, our simulation used plasma pharmacokinetics and not tissue pharmacokinetics. Lastly, this study only suggested the probable dose of sulbactam to achieve the PKPD index. Further clinical studies are needed to determine the most beneficial dosage regimens.In conclusion, the present study shows the MIC of sulbactam against CR-AB is quite high. However, sulbactam could be maximized in a dosage as high as 12 g daily with prolonged or continuous infusion,especially in treatment of critically ill patients.
Conflict of interest statement
We declare that there is no conflict of interest.
Acknowledgements
We would like to thank the Microbiology Laboratory Unit of Phramongkutklao Hospital for keeping the MRD-AB isolates. We also thank Dr. Tossawan Jitwasinkul, Faculty of Pharmacy, Silpakorn University for her supportive knowledge and experience.
[1] Bergogne-Berezin E, Towner J.Acinetobacterspp. as nosocomial pathogens: microbiological, clinical, and epidemiological features.Clin Microbiol Rev1996; 9(2): 148-165.
[2] Pogue JM, Mann T, Barber KE, Kaye KS. Carbapenem-resistantAcinetobacter baumannii: epidemiology, surveillance and management.Expert Rev Anti Infect Ther2013; 11(4): 383-393.
[3] Potron A, Poirel L, Nordmann P. Emerging broad-spectrum resistance inPseudomonas aeruginosaandAcinetobacter baumannii: mechanisms and epidemiology.Int J Antimicrob Agents2015; 45(6): 568-585.
[4] Werarak P, Waiwarawut J, Tharavichitkul P, Pothirat C, Rungruanghiranya S, Geater SL, et al.Acinetobacter baumanniinosocomial pneumonia in tertiary care hospitals in Thailand.J Med Assoc Thai2012; 95: S23-S33.
[5] Santimaleeworagun W, Wongpoowarak P, Chayakul P, Pattharachayakul S, Tansakul P, Garey KW. Clinical outcomes of patients infected with carbapenem-resistantAcinetobacter baumanniitreated with single or combination antibiotic therapy.J Med Assoc Thai2011; 94(7): 863-870.
[6] Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Nosocomial bloodstream infections in US hospitals: analysis of 24 179 cases from a prospective nationwide surveillance study.Clin Infect Dis2004; 39(3): 309-317.
[7] Viehman JA, Nguyen MH, Doi Y. Treatment options for carbapenem-resistant and extensively drug-resistantAcinetobacter baumanniiinfections.Drugs2014; 74(12): 1315-1333.
[8] Tiengrim S, Tribuddharat C, Thamlikitkul V. In vitro activity of tigecycline against clinical isolates of multidrug-resistantAcinetobacter baumanniiin Siriraj Hospital, Thailand.J Med Assoc Thai2006; 89: S102-105.
[9] Piewngam P, Kiratisin P. Comparative assessment of antimicrobial susceptibility testing for tigecycline and colistin againstAcinetobacter baumanniiclinical isolates, including multidrug-resistant isolates.Int J Antimicrob Agents2014; 44(5): 396-401.
[10] Imberti R, Cusato M, Villani P, Carnevale L, Iotti GA, Langer M, et al.Steady-state pharmacokinetics and BAL concentration of colistin in critically Ill patients after Ⅳ colistin methanesulfonate administration.Chest2010; 138(6): 1333-1339.
[11] Ordooei JA, Shokouhi S, Sahraei Z. A review on colistin nephrotoxicity.Eur J Clin Pharmacol2015; 71(7): 801-810.
[12] Rodvold KA, Gotfried MH, Cwik M, Korth-Bradley JM, Dukart G, Ellis-Grosse EJ. Serum, tissue and body fluid concentrations of tigecycline after a single 100 mg dose.J Antimicrob Chemother2006; 58(6): 1221-1229.
[13] Peleg AY, Potoski BA, Rea R, Adams J, Sethi J, Capitano B, et al.Acinetobacter baumanniibloodstream infection while receiving tigecycline: a cautionary report.J Antimicrob Chemother2007; 59(1):128-131.
[14] Freire AT, Melnyk V, Kim MJ, Datsenko O, Dzyublik O, Glumcher F, et al. Comparison of tigecycline with imipenem/cilastatin for the treatment of hospital-acquired pneumonia.Diagn Microbiol Infect Dis2010; 68(2):140-151.
[15] US Food and Drug administration. FDA Drug Safety Communication:FDA warns of increased risk of death with IV antibacterial Tygacil(tigecycline) and approves new Boxed Warning. USFDA, 2013. [Online]Available from: https://www.fda.gov/Drugs/DrugSafety/ucm369580.htm.[Accessed on: 2017 April 15].
[16] Adnan S, Paterson DL, Lipman J, Roberts JA. Ampicillin/sulbactam:its potential use in treating infections in critically ill patients.Int J Antimicrob Agents2013; 42(5): 384-389.
[17] Betrosian AP, Frantzeskaki F, Xanthaki A, Douzinas EE. Efficacy and safety of high-dose ampicillin/sulbactam vs. colistin as monotherapy for the treatment of multidrug resistantAcinetobacter baumanniiventilatorassociated pneumonia.J Infect2008; 56(6): 432-436
[18] Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, et al. Management of adults with hospital-acquired and ventilatorassociated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society.Clin Infect Dis2016; 63(5): e61-e111.
[19] Sime FB, Udy AA, Roberts JA. Augmented renal clearance in critically ill patients: etiology, definition and implications for beta-lactam dose optimization.Curr Opin Pharmacol2015; 24: 1-6.
[20] Yokoyama Y, Matsumoto K, Ikawa K, Watanabe E, Shigemi A, Umezaki Y, et al. Pharmacokinetic/pharmacodynamic evaluation of sulbactam againstAcinetobacter baumanniiin in vitro and murine thigh and lung infection models.Int J Antimicrob Agents2014; 43(6): 547-552.
[21] Roberts JA, Kirkpatrick CM, Lipman J. Monte Carlo simulations:maximizing antibiotic pharmacokinetic data to optimize clinical practice for critically ill patients.J Antimicrob Chemother2011; 66(2): 227-231.
[22] Falagas ME, Karageorgopoulos DE. Pandrug resistance (PDR), extensive drug resistance (XDR), and multidrug resistance (MDR) among Gramnegative bacilli: need for international harmonization in terminology.Clin Infect Dis2008; 46(7): 1121-1122.
[23] Clinical and Laboratory Standard Institute.Performance standards for antimicrobial susceptibility testing; twenty-seventh informational supplement.CLSI document M100S; Wayne: PA; 2017.
[24] Jaruratanasirikul S, Wongpoowarak W, Wattanavijitkul T, Sukarnjanaset W, Samaeng M, Nawakitrangsan M, et al. Population pharmacokinetics and pharmacodynamics modeling to optimize dosage regimens of sulbactam in critically ill patients with severe sepsis caused byAcinetobacter baumannii.Antimicrob Agents Chemother2016; 60(12):7236-7244.
[25] Gao C, Tong J, Yu K, Sun Z, An R, Du Z. Pharmacokinetics of cefoperazone/sulbactam in critically ill patients receiving continuous venovenous hemofiltration.Eur J Clin Pharmacol2016; 72(7): 823-830.
[26] Asín-Prieto E, Rodríguez-Gascón A, Isla A. Applications of the pharmacokinetic/pharmacodynamic (PK/PD) analysis of antimicrobial agents.J Infect Chemother2015; 21(5): 319-329.
[27] Nazer LH, Kharabsheh A, Rimawi D, Mubarak S, Hawari F.Characteristics and outcomes ofAcinetobacter baumanniiinfections in critically ill patients with cancer: a matched case-control study.Microb Drug Resist2015; 21(5): 556-561.
[28] Khawcharoenporn T, Pruetpongpun N, Tiamsak P, Rutchanawech S,Mundy LM, Apisarnthanarak A. Colistin-based treatment for extensively drug-resistantAcinetobacter baumanniipneumonia.Int J Antimicrob Agents2014; 43(4): 378-382.
[29] Chen H, Liu Q, Chen Z, Li C. Efficacy of sulbactam for the treatment ofAcinetobacter baumanniicomplex infection: A systematic review and meta-analysis.J Infect Chemother2017; 23(5): 278-285.
[30] Pongpech P, Amornnopparattanakul S, Panapakdee S, Fungwithaya S,Nannha P, Dhiraputra C, et al. Antibacterial activity of carbapenem-based combinations againts multidrug-resistantAcinetobacter baumannii.J Med Assoc Thai2010; 93(2): 161-171.
[31] Punpanich W, Munsrichoom A, Srisarang S, Treeratweeraphong V.In vitroactivities of colistin and ampicillin/sulbactam againstAcinetobacter baumannii.J Med Assoc Thai2011; 94: S95-100.
[32] Jaruratanasirikul S, Wongpoowarak W, Aeinlang N, Jullangkoon M.Pharmacodynamics modeling to optimize dosage regimens of sulbactam.Antimicrob Agents Chemother2013; 57(7): 3441-3444.
[33] Santimaleeworagun W, Wongpoowarak P, Chayakul P, Pattharachayakul S, Tansakul P, Garey KW.In vitroactivity of colistin or sulbactam in combination with fosfomycin or imipenem against clinical isolates of carbapenem-resistantAcinetobacter baumanniiproducing OXA-23 carbapenemases.Southeast Asian J Trop Med Public Health2011; 42(4):890-900.
[34] Thamlikitkul V, Tiengrim S.In vitroactivity of colistin plus sulbactam against extensive-drug-resistantAcinetobacter baumanniiby checkerboard method.J Med Assoc Thai2014; 97: S1-6.
[35] Laishram S, Anandan S, Devi BY, Elakkiya M, Priyanka B, Bhuvaneshwari T, et al. Determination of synergy between sulbactam, meropenem and colistin in carbapenem-resistantKlebsiella pneumoniaeandAcinetobacter baumanniiisolates and correlation with the molecular mechanism of resistance.J Chemother2016; 28(4): 297-303.
 Asian Pacific Journal of Tropical Biomedicine2018年1期
Asian Pacific Journal of Tropical Biomedicine2018年1期
- Asian Pacific Journal of Tropical Biomedicine的其它文章
- A comprehensive review on anti-diabetic property of rice bran
- Ethnobotanical survey of antimalarial plants in Awash-Fentale District of Afar Region of Ethiopia and in vivo evaluation of selected ones against Plasmodium berghei
- Larvicidal activity of Neem oil and three plant essential oils from Senegal against Chrysodeixis chalcites (Esper, 1789)
- Protective effect of ashwagandha (Withania somnifera) against neurotoxicity induced by aluminum chloride in rats
- Oxidative stress mitigation, kinetics of carbohydrate-enzymes inhibition and cytotoxic effects of flavonoids-rich leaf extract of Gazania krebsiana (Less.): An in vitro evaluation
- Identification of commonly regulated genes in HPV18- and HPV16-infected cervical cancer cells treated with the curcumin analogue 1,5-bis(2-hydroxyphenyl)-1,4-pentadiene-3-one