
Distribution and equity trends for general practitioners in China from 2012 to 2015
2017-10-25 00:58:47YuanyuanWangWeiweiLiuXiaoliWang
Yuanyuan Wang, Weiwei Liu, Xiaoli Wang
Distribution and equity trends for general practitioners in China from 2012 to 2015
Yuanyuan Wang1, Weiwei Liu1, Xiaoli Wang2
Objective: This study aimed to identify the distribution and equity trends for general practitioners (GPs) in China from 2012 to 2015 and to provide evidence to guide the discipline’s development of general practice and for policy-making.
Methods:On the basis of data from the National Health Statistics yearbooks, the distribution and equity trends for GPs from 2012 to 2015 were analyzed with the Lorenz curve and Gini coefficient as indictors of health equity.
Results:From 2012 to 2015 the number of GPs increased at rates ranging from 9.3% to 32.5%,while the number of registered GPs increased at rates ranging from 32.6% to 37.2%. In 2015 the average number of GPs was 1.38 per 10,000 people (among the 31 provinces the highest rate was 3.90 per 10,000 people in Zhejiang and the lowest rate was 0.50 per 10,000 people in Xizang) and 1.98 per 100 km2(among 31 provinces the highest rate was 89.23 per 100 km2in Shanghai and the lowest rate was 0.01 per 100 km2in Xizang). From 2012 to 2015 the Gini coefficients weighted by population were 0.31, 0.29, 0.26, and 0.25 respectively, while the Gini coefficients weighted by geographical area were 0.74, 0.72, 0.72, and 0.72 respectively.
Conclusion:The number of GPs increased rapidly in China; however, the proportion of registered GPs was unsatisfactory, and there were inequities among the different provinces. The government should launch integrated strategies to encourage GP trainees to become registered GPs and optimize the distribution and equity of GPs.
General practice; health equity; Lorenz curve; Gini coefficient
Introduction
General practitioners (GPs) are well known as the first-contact gatekeepers of health in a population, with the potential to reduce inequities associated with access to essential health services [1]. However, in the past few decades of market-oriented reforms in China (beginning in the1980s), the health industry has become excessively commercialized and has pursued specialization and high-tech diagnosis and treatment to an unreasonable extent, resulting in five common shortcomings of health care delivery: inverse care, impoverishing care,fragmented and fragmenting care, unsafe care, and misdirected care [2].
The government and experts have become increasingly aware of the importance of GPs and appropriate technologies for an efficient and equitable health system. In new health reforms, the development of general practice has become a priority. In 2011 the State Council promulgated The Guidance of Establishing a System of General Practitioners and set the goal of “two or three GPs per 10,000 people in both urban and rural areas until 2020” [3]. Since 2013, statistical data on GPs have been routinely reported in the National Health Statistics yearbooks [4—7]. In 2016 the State Council launched the strategic aim of “striving to develop primary health care” in The Outline of Health China 2030 [8].
In recent years the government has encouraged GP residency standardized training programs and specialist — GP transferring training programs to enhance the workforce of GPs [9—11]. GPs and their teams (including nurses, public health professionals, and other community health workers)mostly work in urban community health services and in rural township health centers, both of which are a vital part of primary health systems in China. GPs and their teams are often involved in the following six care activities: providing primary medical care (chronic diseases, common diseases, and illnesses);overseeing disease prevention and immunization efforts; providing health care for specific populations (e.g.,children, pregnant women, elderly people, and people with mental illness); providing rehabilitation services; assisting with health education and family planning; and providing longitudinal continuity for person-centered care and open access to the management of individual and community problems.
Because GPs and their contributions to primary health care as well as the entire health system have been increasingly recognized in China, this study aimed to analyze the trends in the distribution and equity of GPs in China by using data on GPs from 2012 to 2015 from the National Health Statistics yearbooks to provide evidence to guide the discipline’s development of general practice and for policy-making.
Methods
Data sources
Statistical data on GPs and populations from 2012 to 2015 were retrieved from the National Health Statistics yearbooks (2013—2016) [4—7], and statistics data on the geographical areas were retrieved from the website of the State Council [12]. Data from 22 provinces, 5 autonomous regions and 4 municipalities (all areas are simply called as “provinces” in this article, for convenience, that is 31 provinces) in mainland China were collected but did not include data from Taiwan or the two special administrative regions of Hong Kong and Macao.
General practitioners
GPs were classified as (1) registered GPs who had been trained and then registered as a GP or assistant physician or (2) trained GPs who had been trained and qualified to be a GP but were not registered as a GP or assistant physician.
Lorenz curve and Gini coefficient
The Lorenz curve and Gini coefficient were initially developed by economists to describe the distribution and equity of income or wealth among different social groups. In recent years the two indicators have been introduced to evaluate the distribution and equity of health care resources and the fairness of health systems [13—15].
In this study, in the drawing of a Lorenz curve, the x- axis represented the cumulative proportion of the population (or geographical area) ranked from those with the minimum allocation of GPs to the maximum among the 31 provinces, while the y-axis represented the cumulative proportion of GPs. The diagonal line is called the line of perfect equity, and represents the absolute uniform distribution and equity of health care resources (the number of GPs); that is, the farther a data point is from the diagonal line, the greater the inequity on the basis of the Lorenz curve data [14].
The Gini coefficient (also called the Gini ratio or Gini index) is the ratio of the area between the line of perfect equity and the Lorenz curve versus the total area under the line of perfect equity, and theoretically ranges from 0 (perfect equity)to 1 (perfect inequity). When the Gini coefficient is used to evaluate the distribution of health resources, the following values have the following specific meanings: a value less than 0.3 indicates that the distribution is in a particularly equitable condition; a value between 0.3 and 0.4 represents a normal condition; a value between 0.4 and 0.6 raises concern; and a value greater than 0.6 represents a dangerous condition [16—18].
There have been several approaches and formulas to estimate the Gini coefficient by use of different mathematical equivalence processes [17]. In this study a simplified Gini coefficient formula from a previous study on GPs’ distribution and equity in 2012 in China [19] was adopted to keep the values consistent and comparable.
The following simplified formula was used in this study:

where G represents the Gini coefficient, Yirepresents the proportion of the population (or geographical area) in each province, Pirepresents the proportion of GPs in each province, and Pi′represents the cumulative number of GPs ranked by th e allocation of GPs (the number of GPs allocated per 10,000 population or per 100 km2) from the minimum to the maximum among the 31 provinces.
Indicators
Health resources were measured on the basis of the number of GPs per 10,000 population and the number of GPs per 100 km2, which ref l ect the distribution of GPs weighted by the population and by the geographical area respectively. The corresponding Lorenz curves and Gini coefficients were used to evaluate the equity of health resources.
Data processing
Microsoft Excel 2007 was used to conduct parallel entry and management of data, calculate indicators and draw figures.
Results
Allocation of GPs nationwide
In 2012, 2013, 2014, and 2015 the number of GPs was 109,794,145,511, 172,597, and 188,649 respectively, displaying rates of increase of 32.5%, 18.6%, and 9.3% annually. Thus the number of GPs per 10,000 people was 0.81, 1.07, 1.27, and 1.38(with an average annual increase of 0.19) and the number of GPs per 100 km2was 1.15, 1.53, 1.82, and 1.98 (with an average annual increase of 0.28) in 2012, 2013, 2014 and 2015 respectively.
The following two categories of GPs were considered:(1) registered GPs who had been registered as a GP and (2)trained GPs who had not been registered but were trained and qualified to be a GP. The proportions of the two categories were 3 3.9% versus 66.1% in 2012, 32.6% versus 67.4% in 2013, 37.2% versus 62.8% in 2014, and 36.2% versus 63.8%in 2015 (F ig. 1).
In 2012, 2013, 2014, and 2015 the following percentages of GPs were distributed in specific locations (Fig. 2): 19.2%,17.7%, 17.6% and 16.6% respectively in hospitals; 43.6%,41.4%, 39.9%, and 38.8% respectively in community health services; 35.1%, 39.1%, 40.7%, and 42.9% respectively in township health centers; and 2.1%, 1.9%, 1.7%, and 1.6%respectively in other health institutions (e.g., village clinics,independent outpatient clinics, and nursing homes).

Fig. 1. Number of GPs from the two categories in China from 2012 to 2015.
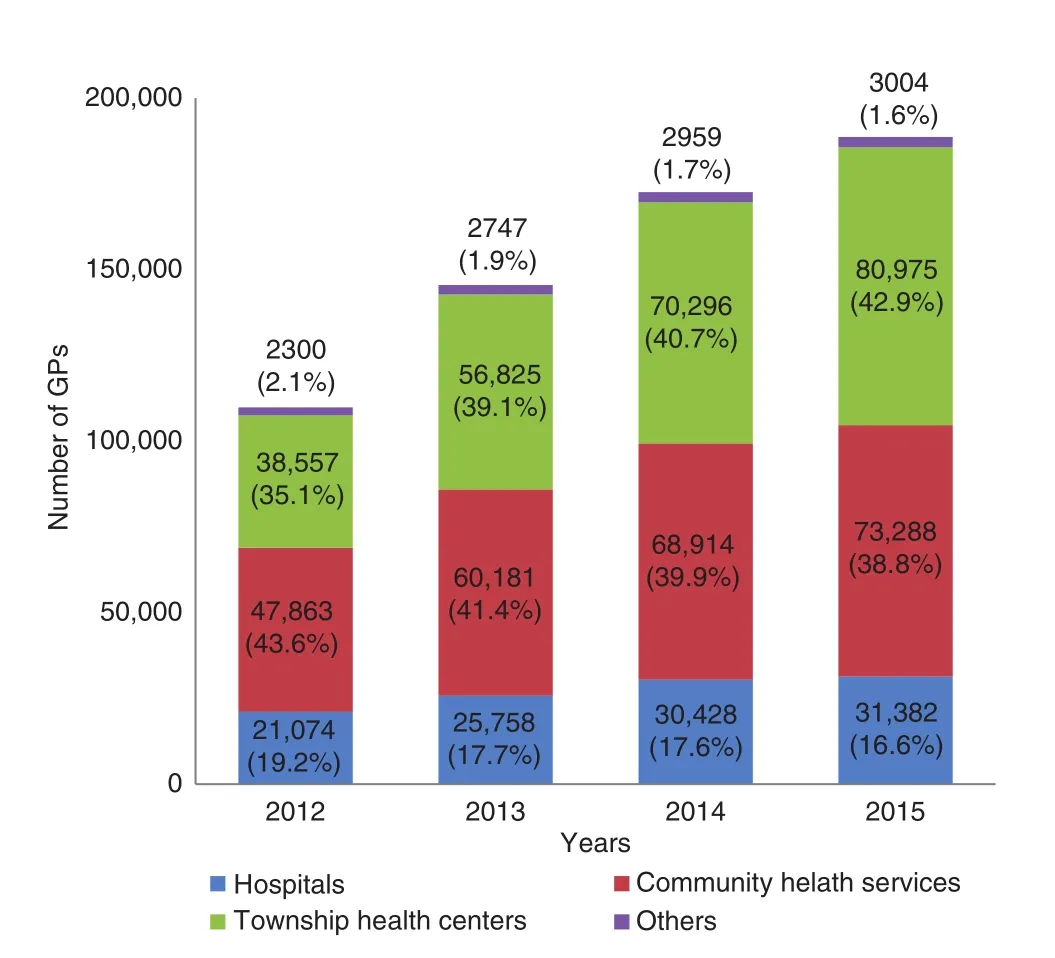
Fig. 2. Number of GPs in different institutions in China from 2012 to 2015.
GP allocation and allocation trends across the provinces
In 2015, only the following four provinces “reached the goal of 2—3 GPs allocated per 10,000 people”: Zhejiang(3.90), Beijing (3.81), Shanghai (3.04), and Jiangsu (2.61).The number of GPs per 10,000 people was lower than 1 in 11 provinces (35.5% of 31 provinces): Guangxi (0.97),Hainan (0.96), Chongqing (0.95), Hunan (0.90), Yunnan(0.90), Guizhou (0.89), Ningxia (0.85), Liaoning (0.83),Jiangxi (0.73), Shaanxi (0.56), and Xizang (0.50). Ranked by the average annual increase, the top three provinces were Zhejiang (0.55), Shanghai (0.27), and Qinghai (0.27), while the bottom three provinces were Liaoning (0.03), Shaanxi(0.02), and Beijing (?0.04).

Table 1. GP allocation and allocation trends in the 31 provinces from 2012 to 2015
On the basis of the number of GPs per 100 km2in 2015, the top three provinces were Shanghai (89.23), Beijing (50.39),and Zhejiang (20.52), while the bottom three provinces were Xinjiang (0.22), Qinghai (0.13), and Xizang (0.01). When ranked by the average annual increase (based on the number of GPs per 100 km2in 2015), the top three provinces were Shanghai (8.21), Zhejiang (2.97), and Tianjin (2.93), while the bottom three provinces were Xinjiang (0.03), Qinghai (0.02),and Xizang (0.00).
Detailed data for each province from 2012 to 2015 are given in Table 1.
GP equity and trends distribution
Figure 3 shows that the Lorenz curves weighted by geographical area were farther from the line of perfect equity than those weighted by population in each year, which indicates that the allocation of GPs by geographical area was more inequitable than that by population. The Gini coefficients weighted by population from 2012 to 2015 were 0.31, 0.29, 0.26, and 0.25 respectively, and displayed a slightly continuous declining trend. In contrast, the Gini coefficients weighted by geographical area were 0.74 in 2012 and consistently 0.72 from 2013 to 2015 (Fig. 4).
Discussion
The number of GPs increased rapidly, although only a low proportion were registered GPs.
The number of GPs has been increasing quickly, especially in township health centers in rural areas. It is estimated that the average number of GPs will reach 2.33 per 10,000 people and 3.38 per 100 km2in 2020, which means that the goal of“2—3 GPs allocated per 10,000 people by 2020” is achievable.

Fig. 3. Lorenz curves for GPs from 2012 to 2015. The x-axis represents the cumulative proportion of the population or geographical area, and the y-axis represents the cumulative proportion of GPs. Blue line, perfect equity; red line and symbols, weighted by population; green line and symbols, weighted by geographical area.
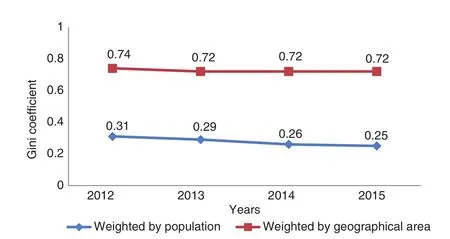
Fig. 4. Gini coefficients for GPs from 2012 to 2015.
However, the average number of GPs per 10,000 people in China is still far lower than in developed countries (e.g.,6.44 in Ireland, 6.62 in Germany, 5.94 in England, and 3.46 in America; see Fig. 5). Furthermore, in China, only approximately 35% of GPs are registered as GP specialists, while the other 65% of GPs are trained and qualified but not registered.Studies in different countries have shown many reasons why GPs leave practice, including policies, salaries, workload,little sense of professional autonomy and values, diminished job satisfaction, negative media portrayal, and low social prestige [24—27], most of which are common in China or even worse in China than in other countries. Moreover, there is an overall shortage in the health workforce in China, as most health workers are allocated to hospitals rather than primary care institutions (including urban community health services,rural township health centers, village clinics, and independent outpatient clinics) [28]. In this study, 16—19% of GPs worked in hospitals but did not work in primary care institutions.
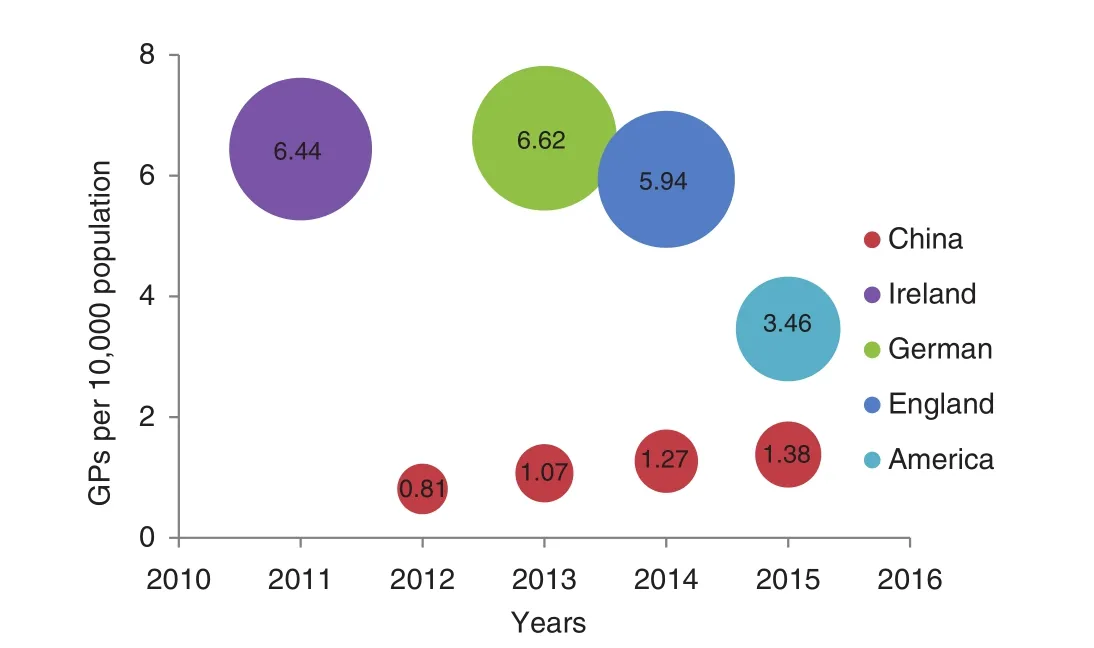
Fig. 5. Number of GPs per 10,000 people in different countries. Data for GPs in England, Germany, and Ireland are from studies published in journals [20—22], while data for GPs in the United States are from the website of the Association of American Medical Colleges [23].
Allocation of GPs differed significantly among provinces,and the inequitable distribution of GPs was more affected by geographical area than by population.
Until 2015, the number of GPs per 10,000 people was more than 2 in four provinces (Zhejiang, Beijing, Shanghai, and Jiangsu) but less than 1 in 11 provinces (Xizang had the lowest number, and the absolute values and rates of increase were both unsatisfactory in Liaoning and Shaanxi). With regard to the number of GPs per 100 km2, the greatest number was in Shanghai (89.23), the lowest number was in Xizang (0.01), and the absolute values and rates of increase were unsatisfactory in Xinjiang, Qinghai, and Xizang. This indicated that the allocation of GPs was insufficient in developing and remote provinces; this is similar to the situation for health care resources (institutions,beds, and medical personnel) in these provinces [17]. According to the Lorenz curves and Gini coefficients from 2012 to 2015,the distribution of GPs in the population was in a particularly equitable condition, while the distribution in geographical areas was in the dangerous condition throughout the period. This is because a lower density of health professionals correlates with worse health efficiency and service quality [29—31].
Of special note, there are many GP training bases in Beijing, from which GP trainees have previously been recruited to other provinces. However, with the increased development of GP training systems and training bases in many provinces over time, the number of trained GPs in Beijing has decreased.Therefore, it cannot be concluded simply that the allocation of GPs has been decreasing in this area.
Policy implications
This study has several policy implications. First, more GPs should be allocated to primary care institutions rather than hospitals. Second, the government should implement a series of strategies to address the shortage and inequality of GPs, especially in developing and remote provinces. Third, GPs should be encouraged to have a better profession-related self-assertiveness.
Limitations
In this study, we analyzed only the distribution and equity of GPs in terms of the quantity or number, and did not take into account the quality or their education levels. In general, the health workforce in underdeveloped areas usually displays less quality and is less well educated [29], which accentuates the misdistribution of GPs in different areas. Furthermore, the distribution of GPs weighted by income or GDP per capita was also not analyzed in this study. These limitations should be addressed in future studies.
Conclusion
Despite the rapid increase in the number of GPs in China,increasing proportions of trained GPs have not been registered. Moreover, there is a severe misdistribution of GPs by geographical area. Thus effective incentives should be offered to encourage trained GPs to work in GP practices, especially in developing and remote provinces.
conflicts of interest
The authors declare no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
1. World Heath Organization. Global strategy on human resources for health: workforce 2030. Geneva: World Heath Organization; 2015.
2. World Health Organization. The world health report 2008 — primary health care (now more than ever). Geneva: World Heath Organization; 2008.
3. State Council of China. The guidance of establishing a system of general practitioners. [accessed 2017 Mar 16]. Available from:www.gov.cn/zwgk/2011-07/07/content_1901099.htm.
4. National Health and Family Planning Commission. National health statistics yearbook 2013. Beijing: Peking Union Medical College Press; 2014.
5. National Health and Family Planning Commission. National health statistics yearbook 2014. Beijing: Peking Union Medical College Press; 2015.
6. National Health and Family Planning Commission. National health statistics yearbook 2015. Beijing: Peking Union Medical College Press; 2016.
7. National Health and Family Planning Commission. National health statistics yearbook 2016. Beijing: Peking Union Medical College Press; 2017.
8. State Council of China. The outline of health china 2030.[accessed 2017 Mar 16]. Available from: www.gov.cn/zhengce/2016-10/25/content_5124174.htm.
9. Li L, Du X, Ma Y, Liu R, Huang C, Guo S, et al. Connotation construct of ‘3+2’ training mode of assistant general practitioner.Chin Gen Pract 2017;20(4):472—6.
10. Xu G, Niu L, Wang J. Perspectives on China’s development in general practice (family medicine) residency programs and curriculum. Chin Gen Pract 2014;17(19):2171—8.
11. Zhang X, Liu Q, Zhang S, Jiang S, Tang Z, Su L. Thinking of establishing demand oriented job-transfer training curricula for general practitioners. Chin Gen Pract 2011;14(31):3599—601.
12. State Council of China. Administrative regional division of the People’s Republic of China. [accessed 2017 Mar 16]. Available from: www.gov.cn/guoqing/2005-09/13/content_5043917.htm.
13. Asl IM, Abolhallaje M, Raadabadi M, Nazari H, Nazari A, Salimi M, et al. Distribution of hospital beds in Tehran Province based on Gini coefficient and Lorenz curve from 2010 to 2012. Electron Physician 2015;7(8):1653—7.
14. Mauguen A, Begg CB. Using the Lorenz curve to characterize risk predictiveness and etiologic heterogeneity. Epidemiology 2016;27(4):531—7.
15. Llorca J, Delgado-Rodriguez M. Visualising exposure-disease association: the Lorenz curve and the Gini index. Med Sci Monit 2002;8(10):T193—7.
16. Zhao B, Yang L, Zheng N, Li H, Li W, An L. The equity analysis of urban community health resource allocation based on Gini coefficient and Theil index. Chin Gen Pract 2014;28:3301—3.
17. Jin J, Wang J, Ma X, Wang, Y, Li R. Equality of medical health resource allocation in China based on the Gini coefficient method. Iran J Public Health 2015;44(4):445—57.
18. Folland S, Goodman AC, Stano M. The economics of health and health care: international edition. Hong Kong: Pearson Education Asia; 2013.
19. Hu W, Yang J, Xu R, Ni R, Meng X, Yu E. Equity analysis of the allocation of general practitioners in mainland China. Chin Gen Pract 2015;22:2628—31.
20. Asaria M, Cookson R, Fleetcroft R, Ali S. Unequal socioeconomic distribution of the primary care workforce: whole-population small area longitudinal study. BMJ Open 2016;6(1):e8783.
21. Bauer J, Brueggmann D, Ohlendorf D, Groneberg DA. General practitioners in German metropolitan areas — distribution patterns and their relationship with area level measures of the socioeconomic status. BMC Health Serv Res 2016;16(1):672.
22. Teljeur C, Tyrrell E, Kelly A, O’Dowd T, Thomas, S. Getting a handle on the general practice workforce in Ireland. Ir J Med Sci 2014;183(2):207—13.
23. Association of American Medical Colleges. Number of people per active physician by specialty. 2015. [accessed 2017 Mar 16]. Available from: www.aamc.org/data/workforce/reports/458490/1-2-chart.html.
24. Doran N, Fox F, Rodham K, Taylor G, Harris M. Lost to the NHS: a mixed methods study of why GPs leave practice early in England. Br J Gen Pract 2016;66(643):e128—35.
25. Cerny T, Rosemann T, Tandjung R, Chmiel C. Reasons for g eneral practitioner shortage — a comparison between France and Switzerland. Praxis (Bern 1994) 2016;105(11):619—36.
26. Puertas EB, Arosquipa C, Gutierrez D. Factors that influence a career choice in primary care among medical students from high-, middle-, and low-income countries: a systematic review.Rev Panam Salud Publica 2013;34(5):351—8.
27. Sumanen M, Aine T, Halila H, Heikkil? T, Hypp?l? H, Kujala S,et al. Where have all the GPs gone — where will they go? Study of Finnish GPs. BMC Fam Pract 2012;13:121.
28. Zhang T, Xu Y, Ren J, Sun L, Liu C. Inequality in the distribution of health resources and health services in China: hospitals versus primary care institutions. Int J Equity Health 2017;16(1):42.
29. Anand S, Fan VY, Zhang J, Zhang L, Ke Y, Dong Z, et al. China’s human resources for health: quantity, quality, and distribution.Lancet 2008;372(9651):1774—81.
30. van Rensburg HC. South Africa’s protracted struggle for equal distribution and equitable access — still not there. Hum Resour Health 2014;12:26.
31. Hara K, Otsubo T, Kunisawa S, Imanaka Y. Examining sufficiency and equity in the geographic distribution of physicians in Japan: a longitudinal study. BMJ Open 2017;7(3):e13922.
1. Peking University Third Hospital, Beijing, 100191, China
2. Peking University Health Science Center, School of Public Health, Beijing, 100083, China
Weiwei Liu
Peking University Third Hospital, Beijing, 100191, China E-mail: c_lww@126.com
9 April 2017;Accepted 31 May 2017
 Family Medicine and Community Health2017年2期
Family Medicine and Community Health2017年2期
- Family Medicine and Community Health的其它文章
- Short sleep duration as a contributor to racial disparities in breast cancer tumor grade
- The relationship between anxiety about prostate cancer among patients with biochemical cancer recurrence and the use of complementary and alternative medicines, diet, and exercise
- Complex multimorbidity and health outcomes in older adult cancer survivorsa
- Symptoms predicting health-related quality of life in prostate cancer patients treated with localized radiation therapy
- Use of prostate-specific antigen testing in Medicare beneficiaries:Association with previous evaluation
- The association of inherited variation in the CLOCK gene with breast cancer tumor grade