
Do cardiopulmonary resuscitation real-time audiovisual feedback devices improve patient outcomes? A systematic review and metaanalysis
2023-12-02 08:24:36NitishSoodAnishSangariArnavGoyalChristinaSunMadisonHorinekJosephAndyHaugerLanePerry
World Journal of Cardiology 2023年10期
Nitish Sood,Anish Sangari,Arnav Goyal,Christina Sun,Madison Horinek,Joseph Andy Hauger,Lane Perry
Abstract BACKGROUND Cardiac arrest is a leading cause of mortality in America and has increased in the incidence of cases over the last several years.Cardiopulmonary resuscitation(CPR) increases survival outcomes in cases of cardiac arrest;however,healthcare workers often do not perform CPR within recommended guidelines.Real-time audiovisual feedback (RTAVF) devices improve the quality of CPR performed.This systematic review and meta-analysis aims to compare the effect of RTAVFassisted CPR with conventional CPR and to evaluate whether the use of these devices improved outcomes in both in-hospital cardiac arrest (IHCA) and out-ofhospital cardiac arrest (OHCA) patients.AIM To identify the effect of RTAVF-assisted CPR on patient outcomes and CPR quality with in-and OHCA.METHODS We searched PubMed,SCOPUS,the Cochrane Library,and EMBASE from inception to July 27,2020,for studies comparing patient outcomes and/or CPR quality metrics between RTAVF-assisted CPR and conventional CPR in cases of IHCA or OHCA.The primary outcomes of interest were return of spontaneous circulation (ROSC) and survival to hospital discharge (SHD),with secondary outcomes of chest compression rate and chest compression depth.The methodological quality of the included studies was assessed using the Newcastle-Ottawa scale and Cochrane Collaboration’s “risk of bias” tool.Data was analyzed using R statistical software 4.2.0.results were statistically significant if P <0.05.RESULTS Thirteen studies (n=17600) were included.Patients were on average 69 ± 17.5 years old,with 7022 (39.8%) female patients.Overall pooled ROSC in patients in this study was 37% (95% confidence interval=23%-54%).RTAVFassisted CPR significantly improved ROSC,both overall [risk ratio (RR) 1.17 (1.001-1.362);P=0.048] and in cases of IHCA [RR 1.36 (1.06-1.80);P=0.002].There was no significant improvement in ROSC for OHCA (RR 1.04;0.91-1.19;P=0.47).No significant effect was seen in SHD [RR 1.04 (0.91-1.19);P=0.47] or chest compression rate[standardized mean difference (SMD) -2.1;(-4.6-0.5)];P=0.09].A significant improvement was seen in chest compression depth [SMD 1.6;(0.02-3.1);P=0.047].CONCLUSION RTAVF-assisted CPR increases ROSC in cases of IHCA and chest compression depth but has no significant effect on ROSC in cases of OHCA,SHD,or chest compression rate.
Key Words: Real-time audiovisual feedback;Cardiopulmonary resuscitation;Cardiac arrest;Return of spontaneous circulation;Survival to hospital discharge;Cardiopulmonary resuscitation quality
INTRODUCTION
Nearly 356000 out-of-hospital cardiac arrest (OHCA) cases and 292200 in-hospital cardiac arrest (IHCA) cases occur annually in the United States,making cardiac arrest one of the leading causes of natural death in America[1-3].In addition,the incidence of cardiac arrest cases has increased over the last twenty years,but little progress has been made in improving survival to hospital discharge (SHD) and functional status including neurological and cardiovascular outcomes[2,4].Consequently,cardiac arrest places a significant burden on public health and society and remains important to research and manage effectively[5,6].
High quality cardiopulmonary resuscitation (CPR) increases survival outcomes in cases of cardiac arrest[7-14].The International Liaison Committee on Resuscitation guidelines specifically emphasize the quality of manual chest compression,including proper hand position,hands off time,compression rate,and compression depth[15].However,the quality of CPR performed by healthcare workers (HCWs) often does not meet recommended guidelines,with the average rate of chest compressions and compression depth being lower than recommended[16-25].
Real-time audiovisual feedback (RTAVF) devices have enabled improvement in consistency and quality of CPR both inside and outside the hospital[26,27].The American Heart Association (AHA) and the International Liaison Committee on Resuscitation have recommended the use of RTAVF devices for CPR training[28-30].Previous systematic reviews and meta-analyses examining the effect of RTAVF devices during cardiac arrest cases concluded that RTAVF-assisted CPR resulted in closer adherence to CPR guidelines but not improved patient outcomes[31,32].However,these studies focused on simulation manikin studies,including only three human trials.This systematic review and meta-analysis aims to compare the effect of RTAVF-assisted CPR with conventional CPR and to evaluate whether the use of these devices improved outcomes in both in-hospital and OHCA patients.
MATERIALS AND METHODS
Search Strategy
Database searches were performed by two independent authors in PubMed,SCOPUS,the Cochrane Library,and EMBASE with individualized search strategies developed for each database (Supplementary Table 1).The search included all studies from the establishment of the database to July 27,2020 without language,methodology,or document filters.References cited in relevant reviews and included studies were also examined.The current systematic review and meta-analysis was constructed in accordance with the PRISMA 2009 guidelines.

Table 1 Characteristics of included studies
Study Eligibility
Studies were included if HCWs were performing CPR using RTAVF devices,where HCWs were defined as anyone with medical training including physicians,nurses,paramedics,emergency medical services,physician assistants,and medical residents.Studies must compare RTAVF-assisted CPR with CPR performed without any device or disabled audiovisual feedback features on cardiac arrest patients,and complete data must be available with a minimum of two metrics reported with measures of central tendency and variability.Language was restricted to English.Simulation studies,animal studies,case reports,conference abstracts,reviews,trial protocols,and studies with incomplete or missing data were excluded.
Review Process and Data Collection
Abstracts of studies were reviewed for relevance by two independent authors.Abstracts with common agreement between reviewers were identified for further review of the full manuscript.Disagreements regarding the inclusion or exclusion of any studies were independently resolved by a third author.Data was extracted from articles selected for inclusion in the present study.Primary outcomes of interest were patient outcomes: return of spontaneous circulation(ROSC) and SHD.Secondary outcomes of interest were CPR quality metrics: chest compression rate and chest compression depth.Mean values and standard deviations were extracted from studies.Methodological quality was reviewed utilizing the Newcastle-Ottawa Quality Assessment scale for cohort studies and using the Cochrane Collaboration’s “risk of bias” tool for randomized controlled trials (RCT)[33,34].Methodological quality was assessed by two independent authors with disagreements resolved by a third author.
Statistical Analysis
Data was analyzed using R statistical software 4.2.0.Random-effects models were used[35,36].When values were presented as interquartile range or range or median,they were converted into mean and standard deviation for analysis using the methodology presented in Wanetal[37] 2014.Pooled risk ratio (RR) or standardized mean difference (SMD)was calculated for binary and continuous metrics respectively[38-40].Heterogeneity was assessed usingI2[41,42].Publication bias was assessed using funnel plots and Egger’s tests.Results were statistically significant ifP<0.05.
RESULTS
Study Selection
A PRISMA flow diagram is shown in Figure 1.The systematic search of articles identified 9422 results.102 full-text articles were identified as potentially relevant after title and abstract screening.Thirteen studies were included after fulltext review (Figure 1)[8,26,27,43-52].Thirteen studies reported data on ROSC and ten reported data on SHD.Important characteristics for each study are summarized in Table 1.
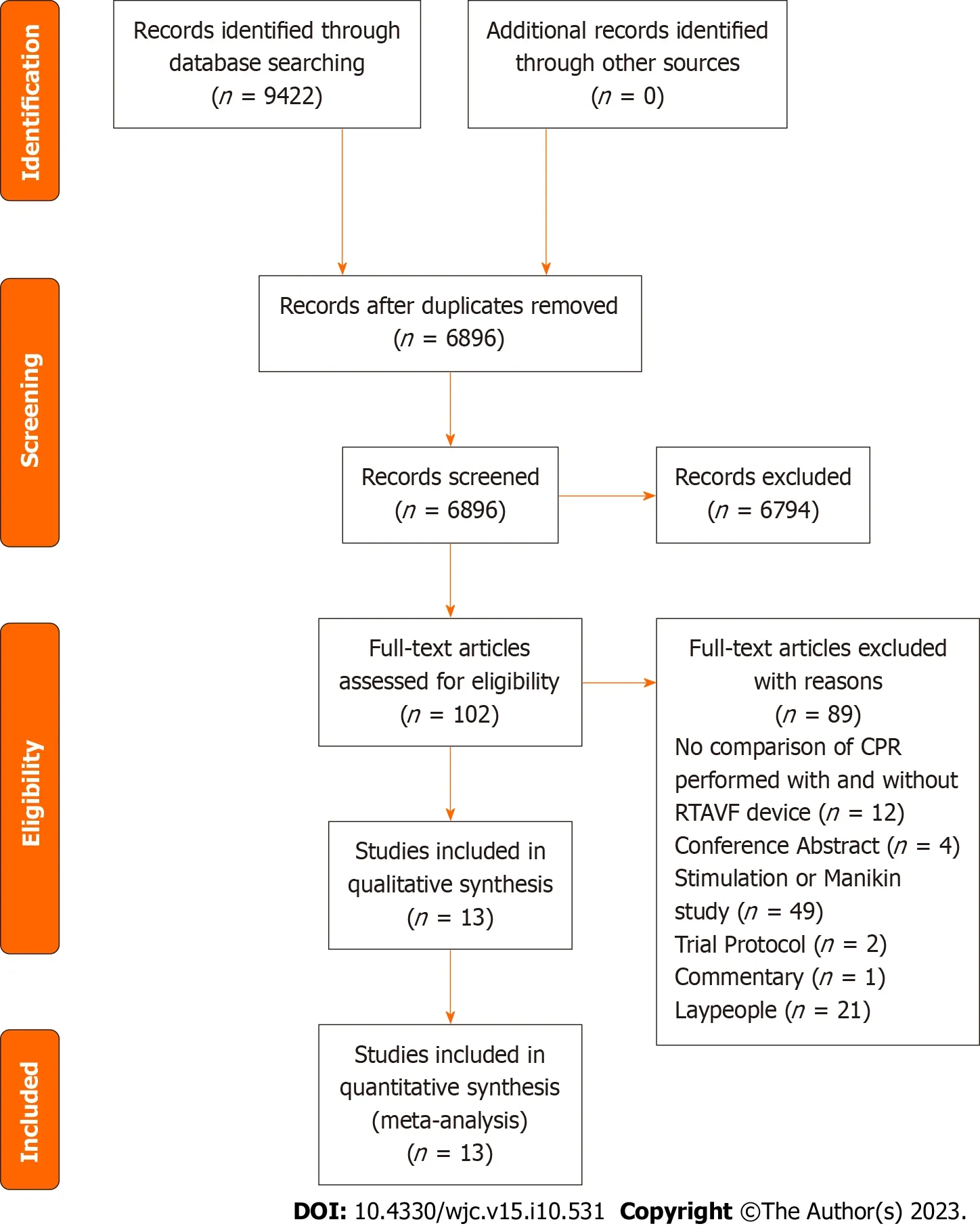
Figure 1 Preferred reporting items for systematic reviews and meta-analyses flow diagram of included and excluded articles.
Study Characteristics
A total number of 17600 participants from 13 studies were included for analysis.Patients were on average 69 ± 17.5 years old,with 7022 (39.8%) female patients.All studies were published between the years 2006 and 2020.Six studied the influence of RTAVF devices in OHCA,while six studied their influence in IHCA.One examined both OHCA and IHCA(Table 1)[44].All studies examined adult populations,with Parketal[49] 2018 examining patients greater than 15 years old.
Risk of Bias
Risk of bias was assessed in all 13 studies.Of the studies included,four were RCTs[45,46,51,52].Using Cochrane’s Risk of Bias tool,the risk of bias was assessed to be low risk in three RCTs and medium risk in one RCT (Supplementary Table 2).Using the Newcastle-Ottawa Scale,the risk of bias was assessed to be low in eight studies and medium in one study(Supplementary Table 3).Egger’s test found no evidence of publication bias in any outcomes of interest (Supplementary Figure 1).
Outcomes
Pooled ROSC was 37% (95% confidence interval (CI)=23%-54%) (Supplementary Figure 2A).Parketal[49] 2018 was identified as a potential outlier using leave-one-out sensitivity analysis with the lowest survival rate of 9%.Visual inspection of the associated funnel plot found no clear asymmetry (Supplementary Figure 2B).

Figure 2 Forest plot of return to spontaneous circulation. ROSC: Return of spontaneous circulation.
ROSC
Thirteen trials reported ROSC as an outcome of interest (n=17600).ROSC occurred in 1693 patients (21.0%) in the RTAVF-assisted CPR group and 1602 patients (16.8%) in the conventional CPR group.All studies included data on ROSC in both the RTAVF-assisted CPR group and the conventional CPR group.Using a random-effects model,patients in the RTAVF group were significantly more likely to achieve ROSC than the conventional CPR group (RR 1.17;95%CI=1.001-1.362;P=0.048) (Figure 2).
Subgroup analysis revealed that the location of cardiac arrest was significantly correlated with patient outcomes (Pvalue for interaction=0.02) (Supplementary Figure 3).ROSC in the setting of IHCA was significantly improved in the RTAVF group (RR 1.36;1.06-1.80;P=0.002).However,ROSC in the setting of OHCA was not significantly different between the two groups (RR 1.04;0.91-1.19;P=0.47).
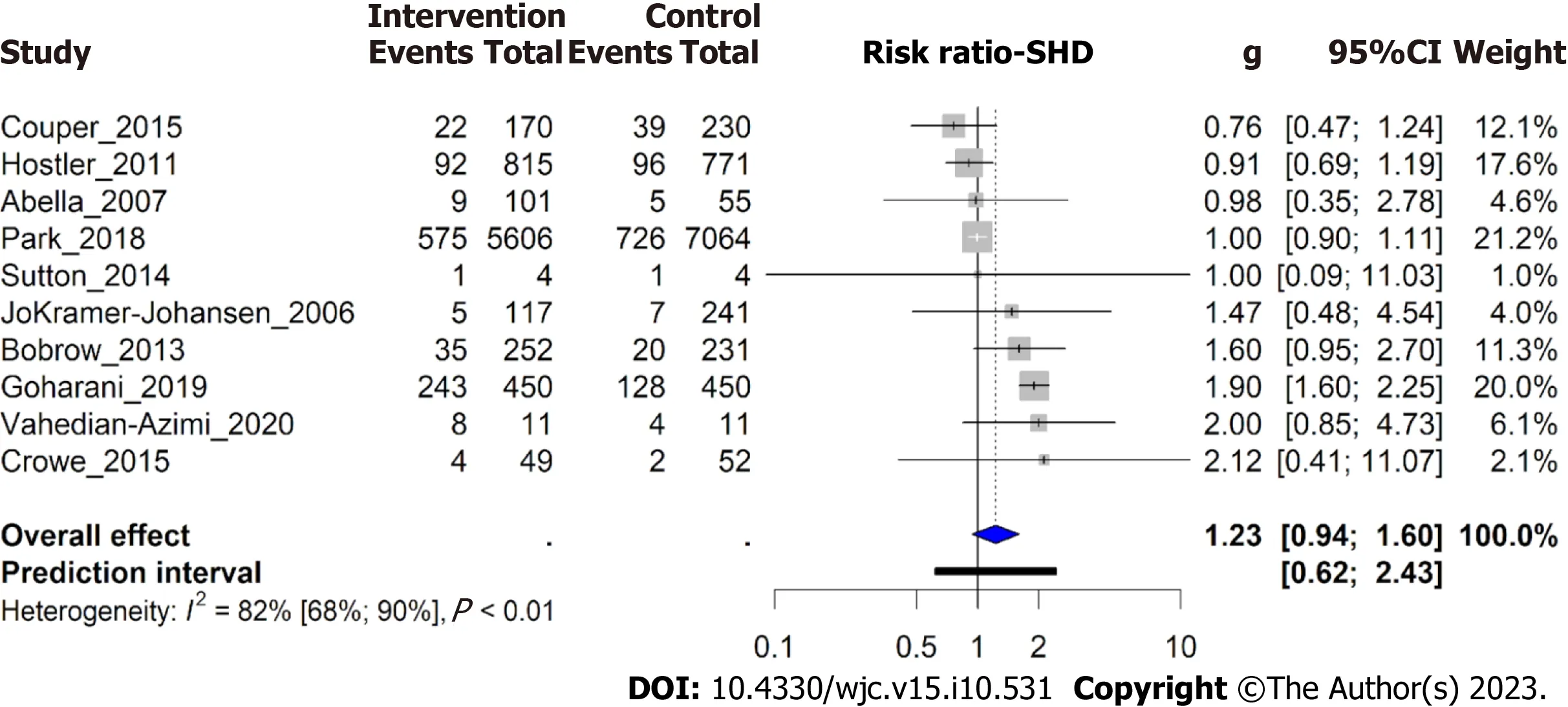
Figure 3 Forest plot of survival to hospital discharge. SHD: Survival to hospital discharge.
Potential causes of heterogeneity in ROSC were explored,with subgroup analysis on study type comparing RCTs with non-RCTs,and region comparing studies within Europe,Middle East/Asia,and North America (Supplementary Figure 4).Heterogeneity remained significant within at least one subgroup in both analyses.
SHD
Ten trials reported SHD as an outcome of interest (n=16684).SHD was reported in 994 patients (13.1%) in the RTAVFassisted CPR group and in 1028 patients (11.2%) in the conventional CPR group.No significant difference was found in SHD between the two groups (RR 1.23;0.94-1.60;P=0.12) (Figure 3).Subgroup analysis found no significant correlation between SHD and the location of cardiac arrest (Pvalue for interaction=0.26) (Supplementary Figure 5).
Secondary Outcomes
Eight studies reported compression rate as an outcome of interest (n=2804).The average compression rate was 107.3 ±9.4 in the RTAVF-assisted CPR group and 117.5 ± 13.8 in the conventional CPR group,with a nationally recommended rate of 100-120 compressions per minute[53].A non-significant difference was seen between the two,with patients in the intervention group receiving a lower compression rate [SMD -2.1;(-4.6-0.5);P=0.09] (Supplementary Figure 6).While both groups had an average compression rate within the nationally recommended guidelines,the proportion of compressions that fell between 100-120 compressions per minute was likely higher in the intervention group than in the control group (Supplementary Figure 6).Eight studies reported compression depth as an outcome of interest (n=2625).The average compression depth was 4.59 cm ± 0.91 cm in the intervention group and 4.24 cm ± 1.29 cm in the control group,with a nationally recommended compression depth of 5-6 cm in the average adult[53].Neither group had an average compression depth that met AHA guidelines.However,a significant difference was seen between the two groups,with patients in the intervention group receiving a higher compression depth,closer to AHA guidelines [SMD 1.6(0.02-3.1);P=0.047] (Supplementary Figure 7).
DISCUSSION
This manuscript analyzed the most recent evidence with regards to the efficacy of real-time audiovisual feedback devices in improving CPR quality and patient outcomes.A total of 13 studies (n=17600) were included,making it the largest study of this topic to date.
Currently,patient outcomes after cardiac arrest remain poor.This meta-analysis found an average ROSC of 37%,which is consistent with previous literature findings ranging between 13% and 72%[54-59].
The AHA mandated that beginning January 2019,all AHA courses that teach adult CPR will be required to use a realtime audiovisual feedback device.These devices typically measure one or more of the following CPR metrics: Chest compression rate,depth,hand position,recoil,ventilation volume,ventilation rate,and hands-off time.Multiple types of feedback devices exist,including manikins with integrated sensors,devices that can be added to existing manikins,and hand-held devices that can be easily transferred from patient to patient[60].As this meta-analysis examined the effect of using RTAVF devices during CPR on patient outcomes,the only type of RTAVF devices that were analyzed were handheld devices that can be used during CPR on patients,rather than manikin-based RTAVF devices.
Thirteen studies with a total of 17600 patients were analyzed.These studies were a mixture of 4 RCT,2 non-RCT,4 cohort studies,2 before-after studies,and 1 matched pair registry study.Studies took place across the globe with only 5 in the United States.These studies were both clinically and statistically heterogenous,with varying protocols and outcomes.Despite this heterogeneity,all studies did examine the primary outcome of ROSC with ten of thirteen also examining SHD.
Contrary to prior literature reviews,this analysis found that the use of real-time audiovisual feedback devices did significantly improve ROSC in cases of IHCA.This may be because prior meta-analyses included only three human intervention studies,while this meta-analysis had a larger number of studies and patients[31,32].In addition,Kirkbrightetal[32] 2013,Gugelmin-Almeidaetal[31] 2021,and Lvetal[61] 2022 included only 1,2,and 5 studies focusing on IHCA,respectively.This meta-analysis found that the location of cardiac arrest played a significant role in whether RTAVF devices influenced ROSC,with a significant increase in ROSC seen in cases of IHCA and no such increase seen in cases of OHCA.This could be another reason why prior reviews found no significant impact of RTAVF devices on ROSC.In particular,Lvetal[61] 2022 found that RTAVF-assisted CPR did not improve ROSC across all studies,but did not differentiate between ROSC outcomes in IHCA and OHCA settings.These findings suggest that hospitals should prioritize the rollout and adoption of RTAVF devices in areas most likely to see IHCA,such as intensive care units,telemetry units,and EDs,rather than with paramedics or ambulances[62,63].This difference in survival may be due to the inherent rushed nature of CPR for patients suffering OHCA.Unlike cases of IHCA where a dedicated HCW can focus exclusively on performing high quality CPR,in cases of OHCA,paramedics may be obligated to multi-task,performing CPR while also keeping track of the other required tasks to bring the patient into the hospital safely.As such,the quality of CPR may be reduced in cases of OHCAvsIHCA.Another explanation could be tied to the fact that the time-to-CPR from arrest is lower in cases of IHCAvsOHCA,and as such CPR quality may play a more important role in IHCA than in OHCA[64,65].
Despite the increase in ROSC when using RTAVF devices,no similar increase was seen in SHD.This insignificance may relate to how CPR quality plays little role in the improvement of survival after ROSC.It could also be due to the presence of comorbidities including heart failure,sepsis,and myocardial infarction and that effective CPR is one factor among many steps required for improved survival.Without additional improvements in other steps required in the care of post-cardiac arrest patients,the increase in CPR quality may be insufficient to translate into improved SHD.
Repeated studies in the literature have shown that CPR quality when performed on manikins improves when using a RTAVF device[31,32].Consistent with existing literature,this meta-analysis also found that CPR quality was increased in RTAVF-assisted CPR.The average compression rate in both groups fell within AHA guidelines,while the average compression depth in both groups fell outside of AHA guidelines[53].However,for both compression rate and depth,the RTAVF group was more likely to have a higher proportion of compressions falling within guidelines compared to the conventional CPR group,showing that RTAVF-assisted CPR was superior to conventional CPR.Prior studies have shown the importance of proper compression depth in patient outcomes[10,16,66].In CPR training courses being taught with RTAVF devices,a larger focus should be put on achieving adequate compression depth.
Overall,the evidence suggests that RTAVF-assisted CPR is of superior quality than conventional CPR.In addition,RTAVF-assisted CPR has a small benefit in patient outcomes,specifically improving ROSC in cases of IHCA.However,this meta-analysis has multiple limitations.First,the studies examined were both statistically and clinically heterogeneous,with varying study parameters,outcomes,and designs,limiting the internal validity of the meta-analysis.This was partially accounted for using a random-effects model and by subgroup analysis,but not all heterogeneity could be accounted for.This may partially be due to the limitations ofI2as a metric for heterogeneity.This study contained relatively larger studies than most examining this topic,and prior literature has documented that as sampling error decreases,I2tends to increase,which can erroneously lead to assumptions that clinical heterogeneity has also increased.In addition,as this meta-analysis examined the class of all RTAVF devices used in CPR,some degree of clinical heterogeneity is expected,as the expected effects of individual devices can vary.Second,nine of these thirteen studies were not RCT,which can introduce sources of both confounding and selection bias.However,ROSC outcomes of cardiac arrest patients are dependent upon many non-controllable factors that cannot undergo randomization including time from arrest to CPR initiation and presence of shockable rhythm which may limit the advantage an RCT would have over other nonrandomized studies designs.Third,this meta-analysis only examined RTAVF devices that could be used during CPR on patients rather than RTAVF devices that are built into manikins.As such,these results cannot be extrapolated to that class of RTAVF devices.Fourth,this meta-analysis only reviewed publications in the literature until 2020,precluding studies published thereafter from inclusion in this analysis.Fifth,this meta-analysis was limited by the evidence that could be extracted from prior reports in the literature,and evidence on long-term patient outcomes and neurological function from RTAVF-assisted CPR is lacking.Future research should examine such cohorts and associated long-term outcomes.In addition,further research into why the improvements seen in ROSC with RTAVF-assisted CPR were not translated into improvements in SHD is warranted,along with research examining which RTAVF device provides the highest improvement in patient outcomes and CPR quality.
CONCLUSION
This meta-analysis examined 13 studies (n=17600) and found that RTAVF-assisted CPR resulted in a significantly increased rate of ROSC,specifically in cases of IHCA but did not improve SHD.This is a novel finding,with prior metaanalyses finding that the use of RTAVF devices did not significantly improve patient outcomes.Consistent with what has been found previously,the use of RTAVF devices resulted in improved CPR quality,as measured by compression rate and depth.
ARTICLE HIGHLIGHTS
Research background
Cardiac arrest is a leading cause of mortality in America and continues to grow in prevalence.Cardiopulmonary resuscitation (CPR) increases survival outcomes in cases of cardiac arrest;however,healthcare workers often do not perform CPR within recommended guidelines.Real-time audiovisual feedback (RTAVF) devices provide live feedback on CPR performance and subsequently improves the quality of CPR performed.
Research motivation
Effective CPR in cardiac arrest is critical to emergent management and stabilization.RTAVF-assisted CPR devices may improve performance,compliance with recommended guidelines,and survival,therefore,this systematic review and meta-analysis seeks to compare the effect of RTAVF-assisted CPR devices with conventional CPR on patient outcomes in the setting of in-hospital cardiac arrest (IHCA) and out-of-hospital cardiac arrest (OHCA).
Research objectives
To investigate the impact of RTAVF-assisted CPR on patient outcomes and CPR quality with respect to in-and OHCA.
Research methods
The literature search was conducted on PubMed,SCOPUS,the Cochrane Library,and EMBASE from inception to July 27,2020,for studies reporting patient outcomes and/or CPR quality metrics between an RTAVF-assisted CPR and conventional CPR in the setting of IHCA or OHCA.The primary outcomes of interest extracted and analyzed were return of spontaneous circulation (ROSC) and survival to hospital discharge (SHD).Data was analyzed using R statistical software 4.2.0.Resultswere statistically significant ifP<0.05.
Research results
Thirteen studies (n=17600) were included after deduplication,screening,and full-text analysis.Patients were on average 69 ± 17.5 years old,with 7022 (39.8%) female patients.Overall pooled ROSC was 37% among all studies.RTAVF-assisted CPR significantly improved ROSC in the case of IHCAs and improved chest compression depth.No significant improvements were seen in ROSC in cases of OHCA,SHD,or compression rate.
Research conclusions
This meta-analysis found that RTAVF-assisted CPR increases ROSC in the setting of IHCA but has no significant effect on ROSC in the setting of OHCA or SHD.Consistent with previous manikin simulation studies,the meta-analysis found that RTAVF-assisted CPR results in improvements in both chest compression rate and depth.
Research perspectives
Cardiac arrest remains a leading cause of mortality with increasing prevalence.The findings of this study suggest that RTAVF-assisted CPR may improve ROSC in the setting of IHCAs but not in the setting of OHCA.Hospitals should prioritize implementing RTAVF devices in areas with the highest rates of IHCA rather than to paramedics or ambulances.
FOOTNOTES
Author contributions:Sood N,Sangari A,and Goyal A contributed equally to this work;Sood N and Sangari A designed the research study;Sood N,Sangari A,and Goyal A performed the research;Sood N performed the statistical analysis;Sood N,Sangari A,Goyal A,Sun C,Horinek M,Hauger JA,and Perry L analyzed the data and wrote the manuscript;Sood N,Sangari A,Goyal A,Sun C,Horinek M,Hauger JA,and Perry L reviewed the manuscript before submission;All authors have read and approved the final manuscript.
Conflict-of-interest statement:The authors deny any conflict of interest.
PRISMA 2009 Checklist statement:The authors have read the PRISMA 2009 Checklist,and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:United States
ORCID number:Nitish Sood 0000-0003-1516-0691;Anish Sangari 0000-0002-4388-7620;Arnav Goyal 0000-0002-6346-7690;Christina Sun 0009-0001-4701-4683;Madison Horinek 0009-0008-1748-2831.
S-Editor:Qu XL
L-Editor:A
P-Editor:Xu ZH
 World Journal of Cardiology2023年10期
World Journal of Cardiology2023年10期
- World Journal of Cardiology的其它文章
- Candida endocarditis: Update on management considerations
- Systemic right ventricle complications in levo-transposition of the great arteries: A case report and review of literature
- Cardiovascular complications following medical termination of pregnancy: An updated review
- Establishment of a prediction model for prehospital return of spontaneous circulation in out-of-hospital patients with cardiac arrest
- Integrated analysis of comorbidity,pregnant outcomes,and amniotic fluid cytogenetics of fetuses with persistent left superior vena cava
- Value of cardiac magnetic resonance on the risk stratification of cardiomyopathies