
Delorme's operation plus sphincteroplasty for complete rectal prolapse associated with traumatic fecal incontinence
2015-12-22 09:15:17MohamedOsmanWalidAbdElMaksoudYosryGaweesh
Mohamed M.Osman,Walid M.Abd El Maksoud,Yosry S.Gaweesh
Department of General Surgery,Faculty of Medicine,University of Alexandria,Alexandria 21526,Egypt.
Delorme's operation plus sphincteroplasty for complete rectal prolapse associated with traumatic fecal incontinence
Mohamed M.Osman,Walid M.Abd El Maksoud?,Yosry S.Gaweesh
Department of General Surgery,Faculty of Medicine,University of Alexandria,Alexandria 21526,Egypt.
Rectal prolapse associated with traumatic fecal incontinence is a rare clinical combination.This study was designed to assess Delorme’s operation with sphincteroplasty as a surgical management of this combination in terms of recurrence and improvement of fecal incontinence.In this prospective study,we enrolled patients suffering from short,full-thickness rectal prolapse associated with traumatic fecal incontinence who had been admitted to Alexandria Main University Hospital during the period of May 2010-January 2013.Preoperative data including cause of trauma,duration of symptoms,results of anal manometry,and degree of fecal incontinence using Wexner score were collected from all patients.Delorme’s procedure with overlap sphincteroplasty was done in all patients.Recurrence of prolapse and improvement of fecal incontinence were assessed after 1,3,6 and 12 months.The study included 13 patients aged(32±8.7)years,9 females and 4 males.Cause of sphincteric injury included previous anal surgery in 7 patients and normal labor in 6 patients.Duration between sphincteric injury and operation was(8.08±2.47)months.Preoperative Wexner's mean score was 16.07±3.4.Early postoperative complications included superficial wound infection(69.2%),minor wound dehiscence(61.5%),and postoperative bleeding(7.6%).Recurrence was detected in 1 patient at 6 month follow-up.Wexner’s score showed significant improvement for all patients after 6 months(4.00±2.04).In conclusion,combination of Delorme’s procedure and sphincteroplasty for treatment of patients with short complete rectal prolapse associated with traumatic fecal incontinence is a safe,effective surgical management with satisfactory results regarding anatomical and functional outcomes.
rectal prolapse,fecal incontinence,Delorme’s operation,sphincteroplasty.
Introduction
Management of complete rectal prolapse is more difficult when it is associated with fecal incontinence as it carries the challenge of correction of both anatomical and functional disorders[1].There are several anatomical abnormalities associated with prolapse,although it is unknown whether these are the cause of,or simply associated with,the anorectal dysfunction[2].Increased awareness of the functional abnormalities associated with rectal prolapse has resulted in the realization that the appropriate surgery should be based not only on the elements of simplicity,low recurrence rate and fewer complications,but it should also take into account the treatment or at least the alleviation of the functional abnormalities so commonly associated with rectal prolapse[3-4].Due to our current incomplete understanding
of the pathophysiology of the condition,there is no strong evidence in favor of any particular surgical approach[1].
Mucosal stripping of the prolapsed rectum followed by plication of the underlying muscular layer was first described by Delorme[5].Patients with a short,fullthickness rectal prolapse can be treated with a mucosal sleeve resection;however,for a longer prolapse,a mucosal sleeve resection is associated with a higher recurrence rate compared with abdominal approaches[6-7]. Sphincteroplastyhasbeenadvocatedtorestoresphincter function in patients with traumatic sphincteric injury. However,many factors such as prior surgery,anatomic derangements,and degree of incontinence may influence the outcome of the procedure[8].In addition,weaknessofthepelvicfloorandapatulousanusmayaugment the problem of rectal prolapse[9].
The purpose of this study was to assess clinical and functionalresultsofDelorme’soperationcombinedwith sphincteroplastyformanagementofcompleterectalprolapse associated with traumatic fecal incontinence.
Patients and methods
Patients
Patients,with complete rectal prolapse associated with traumatic fecal incontinence,admitted to the Colorectal Surgery Unit,Alexandria Main University Hospital,between May,2010 and January,2013 were included in the current study.Major inclusion criteria were the presence of short complete rectal prolapse (less than 10 cm)associated with traumatic fecal incontinence.Causes oftraumatic fecalincontinence included previous normal labor,anal fistula operation such as‘‘lay open’’,or fistulectomy.Major exclusion criteria were partial rectal prolapse or long complete rectal prolapse(more than 10 cm),non-traumatic fecal incontinence caused by neurologic problems affecting the anal sphincter,multiple sphincteric injuries or with previous surgical trials of repair.All patients who were excluded from the study were offered an alternative treatment.
Preoperative measures
All patients were subjected to the following:full history taking with special emphasis on the cause of traumatic incontinence and thorough clinical examination. Wexner’s score[10]was calculated preoperatively for all patients.Anorectal manometry was performed to determine the extent of sphincteric injury.Sigmoidoscopy was done in all patients to exclude other pathologic lesions.Informed consent was obtained from all patients regarding the procedure as well as potentially sharing research information.Preoperative measures included preoperative mechanical preparation with a polyethylene glycol solution done the day before surgery and antibiotic prophylaxis with metronidazole and cephalosporine.Anticoagulant therapy was administered preoperatively for prophylaxis of venous thromboembolism.
Operative work-up
Anesthesia,whether spinal or general,was determined according to the patients’general condition and the preference of the anesthetist,as well as the patients’choice.All the patients were positioned in the lithotomy position.All operations were performed by the same team of colorectal surgeons.
The operation started by reduction of the prolapse, then examination under anesthesia to confirm the location of sphincteric injury.Delorme’s procedure was used to repair the rectal prolapse;the prolapse was fully extended,and then injection of epinephrine solution(1:100,000)into the submucosa was performed followed by a circumferential mucosal incision,about2 cm above thedentate line.The mucosa was dissected from the muscularis layer (Fig.1A).The exposed muscular layer of the wall of the rectum was then folded by eight plicating sutures of 0 Poliglecaprone 25(Monocryl?)absorbable material(Fig.1B)and then gently tied.Eventually, the cut ends of the mucosa were sutured together. The prolapse was then reduced.Disinfection and draping were renewed at that time;then,a semi-lunar skin incision was done at the site of the sphincteric defect. Identification of the edges of the injured sphincter was achieved by gentle dissection(Fig.1C).The procedure was completed by performing overlap sphincteroplasty(Fig.1D).The excised mucosa was sent for pathological examination to assess any inflammatory or ischemic changes.
Postoperative work-up
All patients received intravenous metronidazole and ceftriaxone(three doses)within the first 24 hours after surgery.Oral feeding was allowed after 6 hours after surgery and patients were kept on low residue diet for the first postoperative week.Patients were discharged on the second postoperative day and prescribed oral metronidazole for 5 further days.
Patients were observed during early postoperative period to detect complications(wound dehiscence, bleeding or infection).Patients were followed up to assess recurrence and the condition of the continence during outpatient clinic visits at 1,3,6 and 12 months.
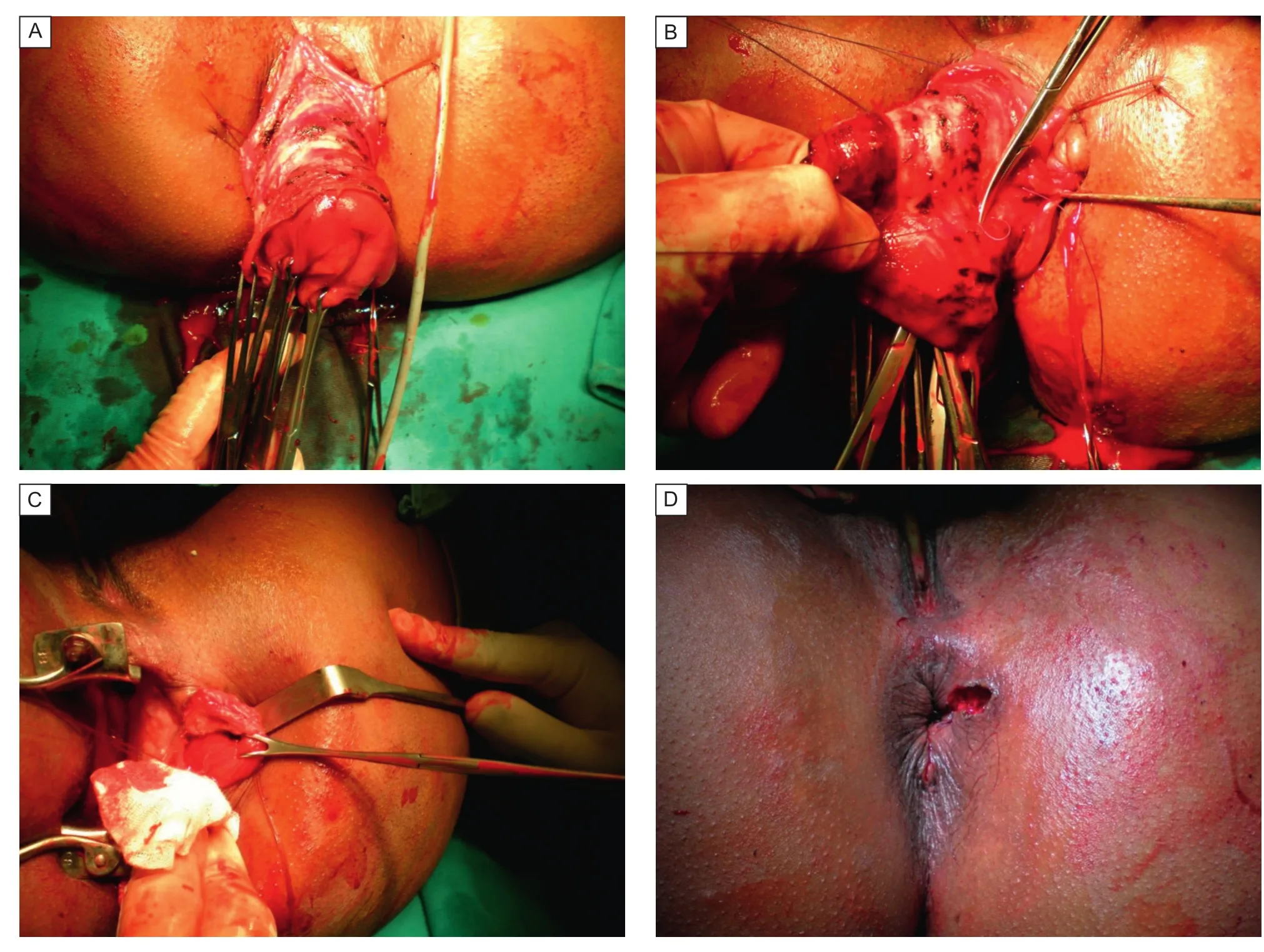
Fig.1Operative work-up.A:dissection of the mucosa from the muscularis propria.B:Plication of the exposed muscular layer of the wall of the rectum.C:Identification of the edges of the injured sphincter.D:Patient after completion of Delorme's procedure and overlap sphincteroplasty.
Outcomes
Primary endpoints:Recurrence detected by the doctor through examination during postoperative visits in outpatient clinic at 1,3,6 and 12 months.Fecal continence was evaluated using Wexner's score[10],by asking the patient during visits in outpatient clinic at 1, 3,6,and 12 months and reported by a doctor(not involved in the research),and compared with the preoperative status.
Statistical analysis
Frequency,percentage,arithmetic mean and standard deviation were applied.Unpaired Student‘‘t’’and one way ANOVA tests and Pearson correlation were used to test for significance at 5%level.Paired test was used to compare Waxner's score at different times.
Results
The study included 14 patients with short complete rectal prolapse and sphincteric injury.All patients underwent combined Delorme’s procedure and sphincteroplasty operations.All patients were followed-up for 1 year for recurrence and assessment of fecal incontinence.One patient was lost in followup and excluded from the study.
Mean age of the patients was(32.0±8.7)years. Nine female patients(69.2%)and only 4 male patients (30.8%)were included in the study.Etiologies of fecal incontinence were previous operation for anal fistula in all male patients and 3 female patients,while previous normal labor was the etiology in the remaining 6 female patients.Six patients(46.2%)were known to have rectal prolapse before trauma.Five patients (38.5%)were known to have occult rectal prolapse before trauma.Two patients(15.4%)complained of symptoms of occult rectal prolapse but were not diagnosed before trauma.Duration between trauma and surgical management was(8.08±2.47)months(4-13 months).Patients with previous normal labor had the sphincteric injury located anteriorly.On the other hand, patients with previous operation for anal fistula had the
sphincteric injury related to the site of the operation. Preoperative Wexner's score was 16.07±3.4(10-20).
Early postoperative complications were encountered in 10 patients(76.9%).Superficial wound infection was encountered in 9 patients(69.2%)while minor wound dehiscence occurred in 8 patients(61.5%). All of these conditions were treated successfully with conservative measures.No patients had major infection.One patient(7.6%)had postoperative bleeding within the first 24 hours.Bleeding was not controlled conservatively and required reoperation to identify the source of bleeding(bleeder at the mucosal anastomosis)and secure it.
During follow-up,recurrence of rectal prolapse occurred in one patient(7.6%)6 months after the surgery.She was offered an abdominal procedure to repair her rectal prolapse.Wexner’s score showed significant improvement for all patients after 6 months.Although it showed some improvement at 12 months,compared to 6 months,this improvement was not statistically significant(Table 1).
Univariate analysis revealed that no risk factors affected continence(Wexner’s score)as primary outcome at 12 months(Table 2).Histopathologic examination of the excised mucosa revealed solitary rectal ulcers in 3 patients(23%),inflammatory changes in 3 patients(23%)and normal mucosa in 7 patients (53.8%).
Discussion
There is great controversy regarding the etiology and pathophysiology of rectal prolapse and rectal intussusceptions over the past decades.Most patients with rectal prolapse have some degree of incontinence and reduced rectal capacity[1].Fecal incontinence accompanying rectal prolapse may be due to sphincter dilatation by the prolapse,weakness of the pelvic floor,or pudendal neuropathy caused by chronic traction of the nerves.On the other hand,reduced rectal capacity is usually due to the bulk of the prolapse,which may augment the problem of incontinence because a well-dis-tensible storage organ is important in preventing fecal incontinence in the presence of weakened sphincters[11].On the other hand,sphincteric injuries may be the cause of rectal prolapsed itself.It is not clear which of the events are primary and which are secondary.Sun et al.[12]studied the pathophysiology of rectal prolapse. He found that the highest anal pressure always remained higher than the rectal pressure during rectal distension in normal subjects,but not in patients with rectal prolapse.He concluded that weakness of the anal sphincter creates the conditions for prolapse of the rectum to occur.This may explain why rectal prolapse became worse after trauma in all patients in our study. It was converted from occult to overt in 5 patients. Also,it appeared after trauma as a new finding in 2 patients.
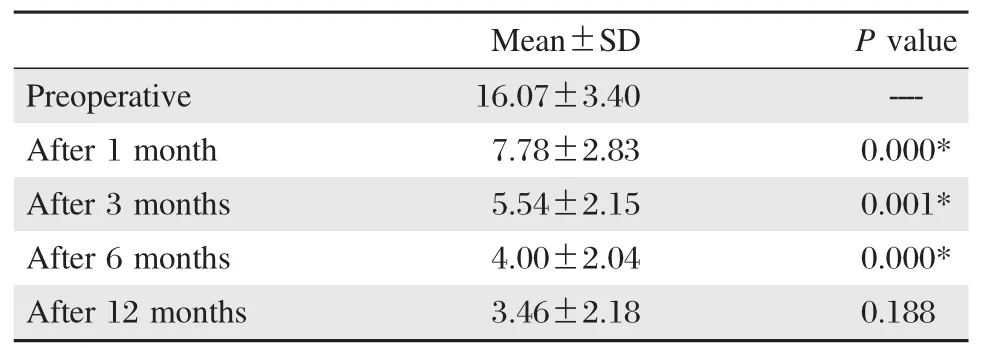
Table 1Comparison between Waxner’s score in the preoperative period and at 1,3,6,and 12 months.
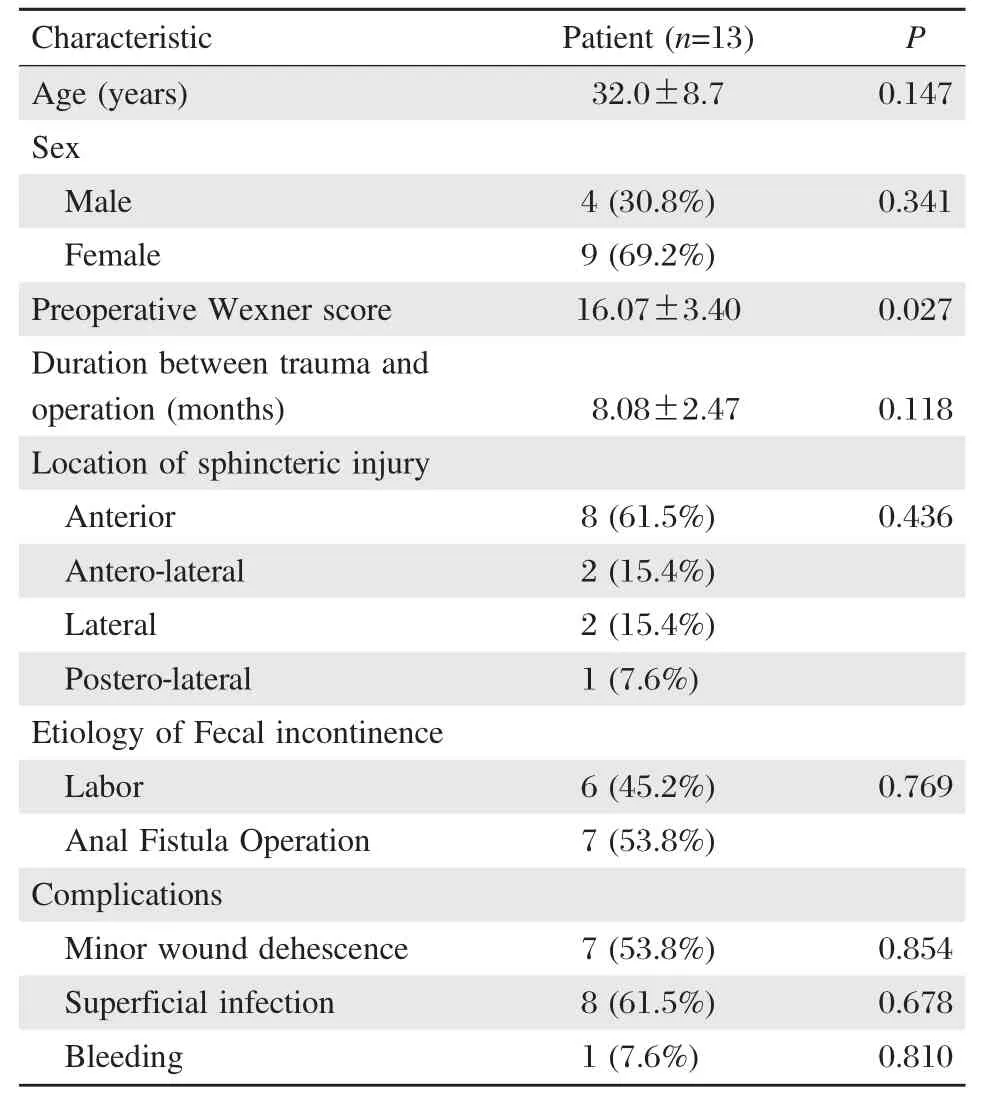
Table 2Univariate analysis of different risk factors affecting Wexner's score at 12 months.
Many studies reported fewer recurrence rates and better improvement of postoperative continence state after the abdominal procedure for rectal prolapse,compared to perineal procedures[13-15].However,abdominal procedures are not ideal and have many disadvantages. In addition to the general hazards of laparatomies,a well-known complication of abdominal rectopexy is constipation.Constipation and/or obstructed defecation is usually due to a number of factors,such as rectal stricture,increased recto-sigmoid angle,and peri-rectal denervation[16].A concomitant sigmoid resection,if added to rectopexy,may decrease the constipation rate[15].Pelvic nerve damage is another risk in abdom-
inal procedures.It may cause sexual dysfunction in men and adhesion formations which may affect fertility in women.The hypogastric nerve may be damaged during a sacral rectopexy,causing a disturbed ejaculation in male patients.Retrograde ejaculation and impotence may occur in up to 17%of the patients and are considered major in causes of dissatisfaction after posterior rectopexy[17-18].
Delorme’s procedure is a perineal procedure for repair of rectal prolapse.Many studies reported high recurrence rates after Delorme’s procedure(up to 32%),so it became less popular and was reserved for older,medically-unfit patients[18].We agree with Lieberth et al.[19]that many studies comparing the results of abdominal and perineal proceduressufferfromselectionbias.Statistically,correction for age and medical condition is required to validate their results and assure their significance.On the other hand, manystudiesevaluatingDelorme’sproceduredidnotconsider factors resulting in poor outcome such as proximal procidentia with retrosacral separation on defecography, severe fecal incontinence,and chronic diarrhea.In addition,recent published studies presented far better results for Delorme’s procedure,compared with older publications;thus,the recent recurrence rate reported was 10%-13%and there was improvement of continence in 63%-87%of patients[19-20].
In our study,we were treating patients with short, full rectal prolapse and severe fecal incontinence due to previous trauma.As there is no ideal operation, we thought that good candidate selection for each procedure is the key for satisfactory outcomes.We chose Delorme’s procedure based on the following factors: most of our patients were young,had good pelvic floors,and an abdominal procedure could have resulted in functional disturbance and led to unsatisfactory results.In addition,4 of our patients were young males and the possibility of sexual life impairment could have led to severe dissatisfaction even with complete cure of their original problems.Severe fecal incontinence is an adverse prognostic factor for the outcome of Delorme's procedure in some previous studies[21]. However,these studies were not studying traumatic fecal incontinence,which we think is completely different from fecal incontinence associated with longstanding rectal prolapse.The longer duration of symptoms in those cases led to chronic traction on pudendal nerves and,ultimately,resulted in neuropathy and poor outcome.In traumatic incontinence cases,patients present early and the duration of symptoms is usually shorter,leading to better results.
As we were planning for simultaneous repair of the prolapse and sphincteroplasty,performing rectal prolapse repair from the same surgical field seemed logical,faster,and to have less surgical morbidity. Furthermore,excision of a concomitant rectal ulcer is possible and was found in 23%of excised mucosa in our study.In addition to the above mentioned factors, Delorme’s procedure has lower operative risks,the lack of abdominal-surgical complications and a quicker recovery,making it a safer choice.There is rarely need to wait for ileus resolution and the time interval before stool passage is often much shorter than it is in abdominal procedures[22].The shorter hospital stay and earlier return to work result in a theoretical lower cost.
In the literature,only a few studies have been published on the efficacy of Delorme's procedure in the repair of a rectal prolapse in young patients[19].We could not find any published studies regarding treatment of rectal prolapse combined with traumatic fecal incontinence.Recent studies on Delorme’s procedure have reported low recurrence(9.75%)in young patients[19].The recurrence rate in our study was 7.6%,which is comparable to the recent studies and also with those of the popular transabdominal procedures.Fecal incontinence was improved dramatically after the addition of sphincteroplasty to Delorme’s procedure.Patients showed significant improvement till 6 months after the operation.Comparison of the results from postoperative months 6-12 showed some further improvement;however,it was not statistically significant.We think that 6 months is the proper time to assess the results of sphincteroplasty.Although the indication of sphincteroplasty in the Pescatori et al.[1]case series was not traumatic fecal incontinence,they reported continence improvement in 30%of Delorme procedures with sphincteroplasty.The complications of the combined procedures(Delorme procedure and sphincteroplasty)in our study were simple and easily treated,indicating the safety of the procedures.
Beingnonrandomizedandasingle-centerstudymaybe the limitations of our study.In addition,the paucity of patientswithcombinedrectalprolapseandtraumaticfecal incontinence prevented us from studying more patients.
In conclusion,we suggest combining Delorme's procedure with sphincteroplasty for treatment of patients with short,complete rectal prolapse associated with traumatic fecal incontinence.This combination is safe and effective,with satisfactory results in regards to anatomical and functional outcomes.However,further prospective randomized trials with larger numbers of patients are required to support our results.
Acknowledgements
Authors would like to thank Dr.Ahmed Aboelyazid, Lecturer of Public Health&Community Medicine,
Faculty of Medicine,Mansoura University for his sincere help.
[1] Pescatori M,Interisano A,Stolfi VM,et al.Delorme’s operation and sphincteroplasty for rectal prolapsed and fecal incontinence[J].Int J Colorect Dis,1998,13(5-6): 223-227.
[2] Mahmoud SA,Omar W,Abdel-Elah K,et al.Delorme’s Procedure for Full-Thickness Rectal Prolapse;Does it AlterAnorectalFunction[J].Indian J Surg,2012, 74(5):381-384.
[3] Schiedeck TH,Schwandner O,Scheele J,et al.Rectal prolapse:which surgical option is appropriate?[J].Langenbecks Arch Surg,2005,390(1):8-14.
[4] Eu KW,Seo-Choen F.Functional problems in adult rectal prolapse and controversies in surgical treatment[J].Br J Surg,1997,84(7):904-911.
[5] Delorme R.Sur le traitement des prolapsus du rectum totaux par l’excision de la muqueuse rectale au rectalcolique[J].Bull Mem Soc Chir Paris,1900,24:499-518
[6] Lee S,Kye BH,Kim HJ,et al.Delorme’s Procedure for Complete Rectal Prolapse:Does It Still Have It’s Own Role?[J]J Korean Soc Coloproctol,2012,28(1):13-18.
[7] Hwang YH.Role of the Delorme Procedure for Rectal Prolapse in Young Patients[J].Ann Coloproctol,2013, 29(2):41.
[8] Bleier JI,Kann BR.Surgical management of fecal incontinence[J].Gastroenterol Clin North Am,2013, 42(4):815-836.
[9] Madiba TE,Baig MK,Wexner SD.Surgical management of rectal prolapse[J].Arch Surg,2005,140(1):63-73.
[10]Vaizey CJ.Carapeti E.Cahill JA,et al.Prospective comparison of faecal incontinence grading systems[J].Gut, 1999,44(1):77-80.
[11]Altomare DF,Filippo Pucciani F.In:Rectal Prolapse: Diagnosis and Clinical Management.Chapter(24)Management of Associated Pelvic Dysfunctions:External Rectal Prolapse and Faecal Incontinence.Springer-Verlag 2008, 183-188.
[12]Sun WM,Read NW,Donnelly TC,et al.A common pathophysiology for full thickness rectal prolapse,anterior mucosal prolapse and solitary rectal ulcer[J].Br J Surg, 1989,76(3):290-295.
[13]Brown AJ,Anderson JH,McKee RF,et al.Strategy for selection of type of operation for rectal prolapse based on clinical criteria[J].Dis Colon Rectum,2004,47(1): 103-107
[14]Madiba TE,Baig MK,Wexner SD.Surgical management of rectal prolapse[J].Arch Surg,2005,140(1):63-73.
[15]Yakut M,Kaymakcioglu N,Simsek A,et al.Surgical treatment of rectal prolapse.A retrospective analysis of 94 cases[J].Int Surg,1998,83(1):53-55.
[16]Broden G,Dolk A,Holmstrom.Evacuation difficulties and other characteristics of rectal function associated with procidentia and the Ripstein operation[J].Dis Colon Rectum,1988,31(4):283-286.
[17]Fazeli MS,Kazemeini AR,Keshvari A,et al.Delorme’s Procedure:An Effective Treatment for a Full-Thickness Rectal Prolapse in Young Patients[J].Ann Coloproctol, 2013,29(2):60-65.
[18]Watkins BP,Landercasper J,Belzer GE,et al.Long-term follow-up of the modified Delorme procedure for rectal prolapse[J].Arch Surg,2003,138(5):498-502.
[19]Lieberth M,Kondylis LA,Reilly JC,et al.The Delorme repair for full-thickness rectal prolapse:a retrospective review[J].Am J Surg,2009,197(3):418-423.
[20]Montero JP,Puente MM,Pascual I,et al.Complete rectal prolapse clinical and functional outcome with Delorme’s procedure[J].Rev Esp Enferm Dig,2006,98(11):837-843.
[21]Hoel AT,Skarstein A,Ovrebo KK.Prolapse of the rectum,long term results of surgical treatment[J].Int J Colorectal Dis,2009,24(2):201-207.
[22]Bordeianou L,Hicks CW,Kaiser AM,et al.Rectal Prolapse:An Overview of Clinical Features,Diagnosis,and Patient-Specific Management Strategies[J].J Gastrointest Surg,2014,18(5):1059-1069.
?Corresponding author:Dr.Walid M.Abd El Maksoud,Assistant Professor,Department of General Surgery,Faculty of Medicine, Alexandria University,Alexandria 21526,Egypt.Tel:00201211433351, E-mail:dr.waleedmaksoud@gmail.com.
Received23May2014,Revised 16August2014,Accepted 25December 2014,Epub 01 March 2015
R657.1,Document code:A
The authors reported no conflict of interests.
 THE JOURNAL OF BIOMEDICAL RESEARCH2015年4期
THE JOURNAL OF BIOMEDICAL RESEARCH2015年4期
- THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- Class II transactivator(CIITA)mediates transcriptional repression of pdk4gene by interacting with hypermethylated in cancer 1(HIC1)
- TYMSgene 5′-and 3′-untranslated region polymorphisms and risk of non-syndromic cleft lip and palate in an Indian population
- Distraction osteogenesis for correction of post ankylosis mandibular deformities
- Impact of crosslinking/riboflavin-UVA-photodynamic inactivation on viability,apoptosis and activation of human keratocytesin vitro
- Co-firing of levator palpebrae and masseter muscles links the masticatory and oculomotor system in humans
- Comparison of dimension reduction-based logistic regression models for case-control genome-wide association study:principal components analysisvs.partial least squares