
Association between esophageal cancer in middle-aged and elderly patients and body mass index and waist-to-hip ratio
2014-09-25 02:14:48LihuiYanZhongyuanShanYingSunYingYanZhiquanLu
Lihui Yan, Zhongyuan Shan, Ying Sun, Ying Yan, Zhiquan Lu
Association between esophageal cancer in middle-aged and elderly patients and body mass index and waist-to-hip ratio
Lihui Yan1, Zhongyuan Shan2, Ying Sun2, Ying Yan2, Zhiquan Lu3
Objective:This study determined the relationship between esophageal cancer in middle-aged and elderly patients and body mass index (BMI) and waist-to-hip ratio (WHR).
Methods:A hospital-based case-control study was adopted. Two hundred eighty-two patients who were diagnosed with esophageal cancer through clinical endoscopy, X-ray examination, or histopathologic evaluation, and underwent surgery or received chemotherapy were enrolled as cases. The control group consisted of 282 patients without any cancers or esophageal diseases who were hospitalized during the same period in the same hospital. Face-to-face interviews were conducted using standard survey forms, and the height, weight, waist circumference, and hip circumference were measured to calculate the BMI and WHR. The odds ratio (OR) and 95% confdence interval (CI) between the patient BMI and WHR and esophageal cancer were estimated using a multi-factor logistic regression model.
Results:There was no statistical difference between the case and control groups with respect to age, gender, occupation, educational background, place of residence, and history of high blood pressure (P>0.05); however, there were more cases who smoked cigarettes and consumed alcohol than controls (P<0.05). Single-factor logistic regression analysis showed that the risk for esophageal cancer in overweight and obese patients was 1.53- and 1.82-fold that of normoweight patients, respectively. The risk for esophageal cancer in patients with a WHR in the highest quartile was 1.85-fold the control patients with a WHR in the lowest quartile. After confounding factors, such as gender and age, were adjusted, multi-factor logistic regression analysis indicated that the risk for esophageal cancer in overweight and obese patients increased by 59.4% (OR=1.594) and 78.2% (OR=1.782), respectively, when compared with normoweight patients.
Conclusion:BMI and WHR are important risk factors for esophageal cancer. Overweight and obese patients are at increased risk for esophageal cancer. Maintaining a normal weight may be a factor in preventing esophageal cancer.
Esophageal cancer, Body mass index (BMI), Waist-to-hip ratio (WHR), Casecontrol study
Introduction
Esophageal cancer refers to malignant lesions formed by the abnormal proliferation of esophageal squamous or glandular epithelium. Esophageal cancer is a common malignant tumor in some countries and regions worldwide. China has a high incidence rate of esophageal cancer, and also one of the highestmortality rates of esophageal cancer. According to the world cancer incidence and death report of 2012 released by the International Agency for Research on Cancer (IARC) on 25 August 2014, there were 455,784 cases of esophageal cancer worldwide with 223,306 cases in China (48.99%), and 400,156 deaths worldwide with 197,472 deaths in China (49.35%) [1].
According to the “Malignant Tumor Incidence Rate and Death Analysis of Registry Area in China,” which was released by the National Cancer Center, there were 287,632 cases of esophageal cancer in 2010, of which 204,449 were men and 83,183 were women. During the same year, there were 208,473 deaths associated with esophageal cancer, of which 148,865 were men and 59,608 were women [2]. The incidence of esophageal cancer (overall, 21.88/100,000; males, 30.38/100,000; and females, 12.96/100,000) ranks ffth, following lung, breast, gastric, and liver cancers. The esophageal cancer mortality rate ranks fourth amongst cancerrelated deaths (overall, 15.85/100,000; male, 22.12/100,000; and female, 9.29/100,000). The urban incidence of esophageal cancer (overall, 16.55/100,000; male, 23.92/100,000; and female, 8.81/100,000) ranks sixth, and the mortality rate ranks ffth (overall, 12.19/100,000; male, 17.84/100,000; and female, 6.26/100,000). The rural incidence of esophageal cancer (overall, 27.29/100,000; male, 36.95/100,000; and female, 17.17/100,000) ranks fourth, following lung, gastric, and liver cancers, and the mortality rate (overall, 19.58/100,000; male, 26.47/100,000; and female, 12.36/100,000) ranks fourth, following lung, liver, and gastric cancers.
With social and economic development, the standard of living and dietary structure of residents in China have undergone changes, and the incidence and mortality rates of esophageal cancer have decreased in urban areas. In areas with a high incidence of esophageal cancer, after 30 years of concerted efforts for prevention and control, the incidence and mortality rates of esophageal cancer have decreased, but the incidence and mortality rates are still at an unacceptably high level, resulting in a heavy burden on society and the economy, and seriously affecting the development of the local social economy [3]. Despite the high rate of morbidity associated with esophageal cancer, as well as the pain and burden, the etiology and natural history remain uncertain. Research has shown that the genesis of esophageal cancer may result from the effects of a number of factors, such as nitrosamines, mould and mould toxin contamination, nutritional imbalance, an unhealthy lifestyle, dietary habits, and genetic predisposition [4, 5]. In addition, domestic and international epidemiologic studies also indicate that the genesis of esophageal cancer is mainly related to environmental and dietary factors, including a limited intake of fresh fruits and vegetables and a poor intake of multiple micronutrients [6, 7]. There are scarce reports on the relationship between obesity (an increase in body mass index [BMI] and waist-to-hip ratio [WHR]) and esophageal cancer, and the reported results are inconsistent [8, 9]. Therefore, a hospitalbased case-control study method was designed involving a group of patients with and without esophageal cancer. The differences in general demographic characteristics and physical measures (height, weight, waist circumference [WC] and hip circumference [HC]) in the two groups of patients were investigated to determine the relationship between esophageal cancer and obesity, and to provide a scientifc basis for the prevention and control of esophageal cancer, as well as the implementation of intervention measures.
Subjects and methods
Subjects
Two hundred eighty-two patients with esophageal cancer ≥40 years of age who were admitted to the Oncology Department and Department of Chest Surgery of the First Affliated Hospital of Liaoning Medical College, the Third Affliated Hospital of Liaoning Medical College, and Jinzhou Central Hospital between September 2012 and March 2013 were enrolled as cases. The inclusion criteria were as follows [7]: (1) males and females ≥40 years old; (2) permanent residents of Jinzhou; (3) diagnosed with esophageal cancer >3 months previously by clinical endoscopy, X-ray examination, or histopathologic evaluation; (4) underwent surgery because of esophageal cancer in 1 of the above-mentioned 3 hospitals; (5) diagnosed with esophageal cancer through clinical histopathologic examination and received chemotherapy; and (6) willing to complete the questionnaire. To increase the comparability of the two groups and control the infuence of confounding factors on the results, 1 control case was assigned for each case according to age (±5 years), gender, and place of residence. The patients in the control group were hospitalizedin the same hospital during the same time period; 282 patients without esophageal disease or other digestive tract cancers, but diagnosed with other esophageal diseases comprised the control group. The inclusion criteria for the control group were as follows: (1) same gender as the patients in the case group; (2) age ±5 years of case patients; (3) no esophageal cancer or other digestive tract diseases; (4) no medications for esophageal or other digestive tract diseases within 3 months; (5) no digestive tract cancers; and (6) those who were willing to complete the questionnaire. All of the subjects signed informed consent.
Methods
Face-to-face interviews were conducted using a standard questionnaire self-designed to collect demographic data (age and gender), lifestyle (smoking cigarettes, consuming alcohol, and physical exercise), social and economic status (education, occupation, and family income), personal history of disease (hypertension, diabetes, and cardiovascular disease), and family history of esophageal cancer, and the investigators who had received professional training measured the height and weight using standard methods. The patients wore light clothing without shoes during measurement of the height and weight. The height was rounded to the nearest cm, and the weight was rounded to the nearest 100 g. The WC was measured with the patient in the upright position with the feet 25—35 cm apart, and a soft tape was placed at the midpoint on the line between the inferior border of the lumbar ribs and the iliac crest without compressing the skin and encircling the abdomen. After the subjects sat down for ≥ 5 min, the blood pressure was measured 3 times, and the mean of last two readings was taken for data analysis.
Judgment criteria
The adult BMI criteria in China [10] are divided into the following 4 groups: underweight, BMI≤18.50 kg/m2; normoweight, BMI=18.50—23.99 kg/m2; overweight, BMI=24.00—27.99 kg/m2; and obese, BMI≥28.00 kg/m2. The WHR was calculated according to the following formula: WHR=WC in cm/ HC in cm. The WHR was classifed as follows: normal, males with a WHR≤0.9 and females with a WHR≤0.88; and obese, males with a WHR>0.9 and females with a WHR>0.88. Based on the BMI and WHR values, the study patients were divided into four quartiles (Q1—Q4) for BMI and WHR, which were expressed as continuous variables. To reduce the infuence of extreme values (too high or too low) on the results of this study, the median values of the four BMI and WHR quartiles were utilized; within the same quartiles, the linear trend test was performed. In current epidemiologic studies, BMI is often utilized as an index to defne generalized obesity, and WC or WHR is used as an index to defne centripetal or abdominal obesity [11].
Measurement and control of potential confounding factors
It has been reported that gastroesophageal refux disease (GERD) is an important risk factor for the onset of esophageal cancer, but GERD is not related to BMI [7, 12]. To further control the infuence of confounding factors on the study results, patients in the control group completed an additional comprehensive questionnaire on potential confounding factors, including GERD-type symptoms. The GERD-related questions were as follows: (1) evaluate symptoms during the recent 6 months, including whether or not “heartburn, indigestion, or stomach pain is present”; (2) whether or not middle or upper abdominal discomfort occurs frequently; (3) during the intake of food, whether or not antacids are taken to relieve symptoms; (4) whether or not abdominal discomfort or pain is related to posture (such as, the recumbent position or lumbar fexion); (5) whether or not antacid drugs are taken frequently; and (6) whether or not there is a history of a diagnosis of esophageal hiatal hernia. After the preliminary analysis, GERD-type symptoms were defned if the answer to the following questions was yes: (1) whether or not “heartburn, indigestion, or abdominal pain is present”; (2) position is in the upper abdomen; and (3) antacids are taken to relieve symptoms. If there were GERD-type symptoms, such a control was excluded.
Statistical methods
Results
Comparison of demographic characteristics
There were 282 patients in the case group with an age range from 42 to 76 years and a mean age of 55.27±10.16 years. There were 282 patients in the control group with an age range from 42 to 76 years and a mean age of 55.18±10.33 years. There was no statistical difference between the two groups with respect to age, gender, occupation, educational background, place of residence, and history of high blood pressure (P>0.05). The family income of the patients in the case group was lower than the control group (χ2=5.356,P<0.05). A higher number of patients in the case group smoked cigarettes and consumed alcohol than patients in the control group (P<0.05). The percentage of patients in the case group with diabetes was also higher than the control group (χ2=11.445,P=0.001; Table 1).
Comparison of measured values
The mean BMI in the case group (24.43±3.40 kg/m2) was higher than the control group (22.79±3.30 kg/m2;P<0.01). The mean BMI values in the case group in each age group were greater than the control group; there was a signifcant difference between the two groups in the 45-, 50-, 65-, and 76-year age groups (P<0.05). The mean WHRs in the males in the case group (0.96±0.05) were signifcantly higher than the control group (0.91±0.05;P<0.01). The mean WHRs in the females in the case group (0.95±0.05) was higher than the control group (0.90±0.07;P<0.01). Similarly, after the WHRs were grouped by age, there was a signifcant difference between the two groups in the 50— and 55—59-year age groups (P=0.001); middle-aged women (42—49 year age group) had the most signifcant difference (P=0.001; Table 2).
Relationship between BMI and WHR with esophageal cancer
The results of logistic regression analysis on single factors showed that the risk for esophageal cancer in overweight and obese patients in the case group was1.53 times (95% CI, 1.032—2.524) and 1.82 times (95% CI, 1.163—2.857) that of normoweight patients, and the risk for esophageal cancer in patients within the highest WJR quartile was 1.85 times that of patients within the lowest WHR quartile (95% CI, 1.165—2.941). After confounding factors, such as gender and age, were adjusted, multiple-factor logistic regression analysis showed that the risk for esophageal cancer in overweight and obese patients increased by 59.4% (OR=1.594; 95% CI, 1.058—2.587) and 78.2% (OR=1.782; 95% CI, 1.101—2.786), respectively, when compared with normoweight patients in the control group. When compared with patients within the lowest WHR quartile, the risk for esophageal cancer of patients within the second highest, third highest, and highest quartiles of WHR increased by 4.8%, 32.6%, and 36.5%, respectively (Table 3).
Discussion
There was no statistical signifcance between the two groups with respect to age, gender, occupation, educational background, place of residence, and history of hypertension, which is consistent with the extant literature [5, 7]. A meta-analysis was conducted on the relationship between cigarette smoking and alcohol consumption and esophageal cancer (included in Reference 14), and the results showed that the combined OR of smoking and high expression of p53 protein and p53 gene change in esophageal cancer (high expression of p53 protein+p53 gene mutation) was 1.99 (95% CI, 1.30—3.06), 1.64 (95% CI, 1.13—2.37;P<0.05) [13]. Both the duration of cigarette smoking and consumption of alcohol exhibited a positive dose-response relationship with the the risk for esophageal cancer; domestic and international research reports are consistent in this regard [14—16]. The current study also showed that the proportion of patients in the case group with a history of diabetes was higher than the control group, which is basically consistent with other investigators’ results. A meta-analysis was conducted on the link between diabetes and esophageal cancer (included in Reference 6) [17], and the results showed that for both men and women, the number of patients with diabetes in the case group was signifcantly higher than the control group, and the OR value of female diabetic patients was higher than male diabetic patients (female,
OR=1.58 and 95% CI, 1.14—2.18; male, OR=1.41 and 95% CI, 1.07—1.86). Thus, the presence of diabetes was associated with esophageal cancer, and might be an independent risk factor for esophageal cancer.
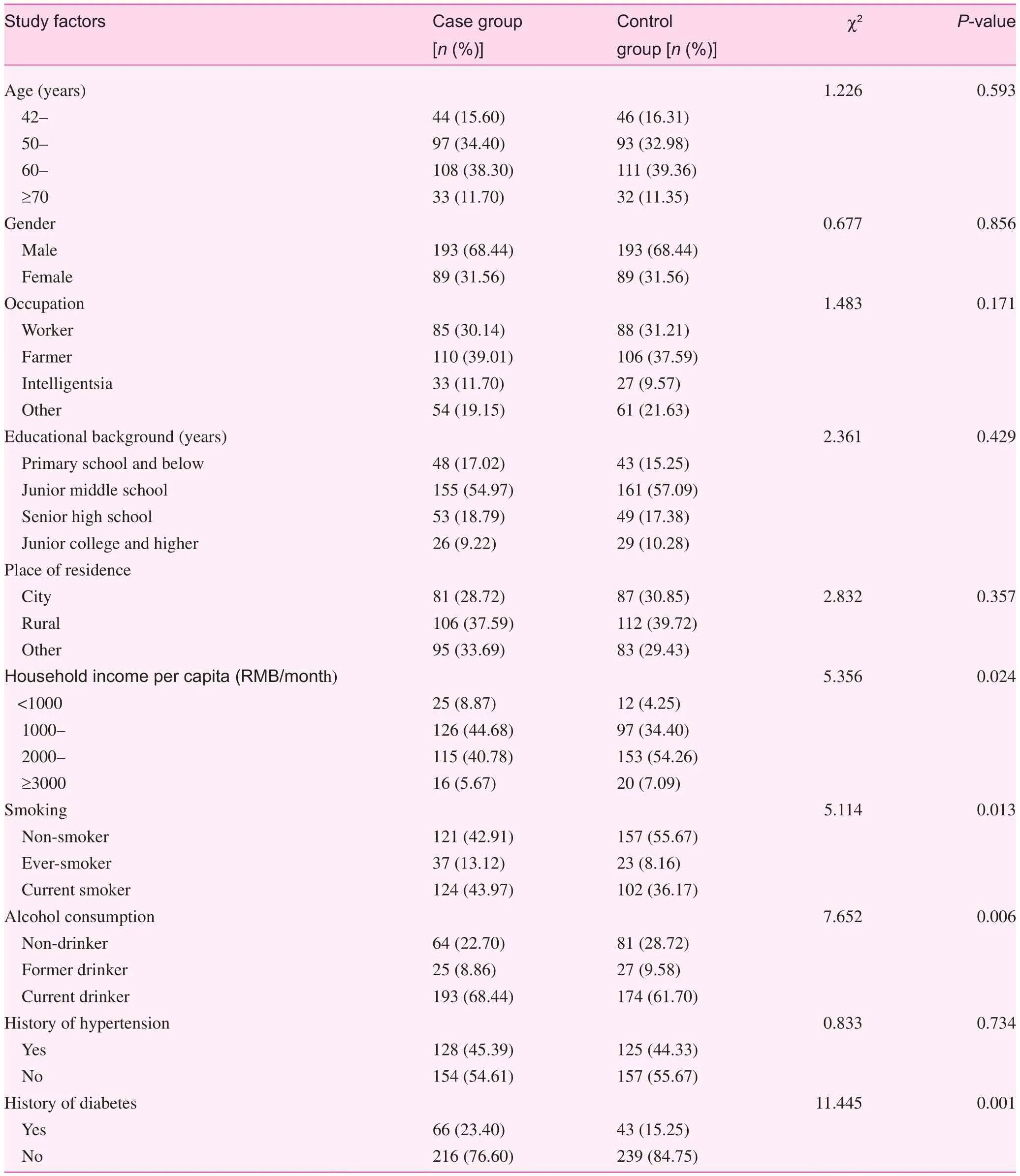
Table 1. Demographic characteristics of the study subjects
The current study showed that the mean BMI in the case group during each age group was signifcantly higher than the control group, and there was a signifcant difference between the two groups during the 45—, 50—, 65—, and 76-year age groups (P<0.05). In addition, the mean WHR of the males in the case group was signifcantly higher than the control group (P<0.01), and the mean WHR of the females in the case group was also higher than the control group (P<0.01). Similarly, for males, there was a very signifcant difference between the two groups during the 50— and 55—59-year age groups; middle-aged (42—49 years) women had the most signifcant difference (P=0.001). Single-factor logistic regression analysis revealed that the risk for esophageal cancer in groups of overweight and obese patients was 1.53 and 1.82 times the normoweight patients in the control group, while the risk for patients within the highest WHR quartile was1.85 times the control group patients within the lowest WHR quartile. After various confounding factors, such as gender and age, were adjusted, multiple-factor logistic regression analysis indicated that the risk for esophageal cancer in the overweight and obese patients in the case group increased by 59.4% (OR=1.594) and 78.2% (OR=1.782), respectively, when compared with normoweight patients. When compared with patients within the lowest WHR quartile, the risk for esophageal cancer in patients within the second highest, third highest, and highest WHR quartiles increased by 4.8%, 32.6%, and 36.5%, respectively
Table 2. Distribution and comparison of BMI and WHR at different ages between the case and control group
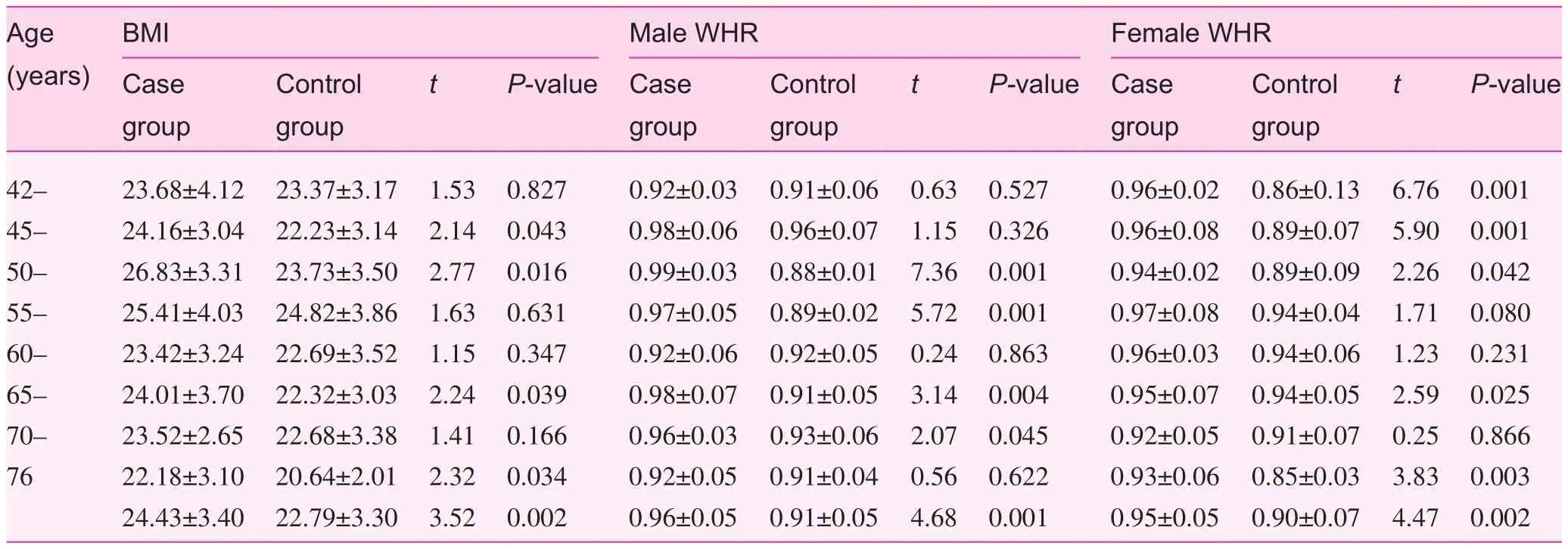
Table 2. Distribution and comparison of BMI and WHR at different ages between the case and control group
Age (years) BMI Female WHR Case group Male WHR Control grouptP-valueCase group Control grouptP-valueCase group Control grouptP-value 42— 23.68±4.12 23.37±3.17 1.53 0.827 0.92±0.03 0.91±0.06 0.63 0.527 0.96±0.02 0.86±0.13 6.76 0.001 45— 24.16±3.04 22.23±3.14 2.14 0.043 0.98±0.06 0.96±0.07 1.15 0.326 0.96±0.08 0.89±0.07 5.90 0.001 50— 26.83±3.31 23.73±3.50 2.77 0.016 0.99±0.03 0.88±0.01 7.36 0.001 0.94±0.02 0.89±0.09 2.26 0.042 55— 25.41±4.03 24.82±3.86 1.63 0.631 0.97±0.05 0.89±0.02 5.72 0.001 0.97±0.08 0.94±0.04 1.71 0.080 60— 23.42±3.24 22.69±3.52 1.15 0.347 0.92±0.06 0.92±0.05 0.24 0.863 0.96±0.03 0.94±0.06 1.23 0.231 65— 24.01±3.70 22.32±3.03 2.24 0.039 0.98±0.07 0.91±0.05 3.14 0.004 0.95±0.07 0.94±0.05 2.59 0.025 70— 23.52±2.65 22.68±3.38 1.41 0.166 0.96±0.03 0.93±0.06 2.07 0.045 0.92±0.05 0.91±0.07 0.25 0.866 76 22.18±3.10 20.64±2.01 2.32 0.034 0.92±0.05 0.91±0.04 0.56 0.622 0.93±0.06 0.85±0.03 3.83 0.003 24.43±3.40 22.79±3.30 3.52 0.002 0.96±0.05 0.91±0.05 4.68 0.001 0.95±0.05 0.90±0.07 4.47 0.002

Table 3. Association of BMI and WHR with the risk for esophageal cancer
Steffen et al. [8] conducted a prospective study involving 346,554 subjects participating in the European Cancer and Nutrition Survey. During the 8.9-year follow-up, there were 198 newly-diagnosed cases of esophageal cancer. The results of the survey showed that BMI, WC, and WHR were positively related with the risk for esophageal cancer (when the highest and lowest quintiles were compared, the RR=2.60 and 95% CI=1.23—5.51;P<0.01) [8].
At present, it is thought that fat metabolism is active in overweight and obese patients. Metabolism of fats can produce a variety of compounds which circulate throughout the body, and the metabolism of intra-abdominal fat is different than that of surrounding fat [18]. Some metabolites, such as insulin-like growth factor (IGF) and leptin, have been shown to be associated with malignant tumors. The fat metabolites may reduce cellular death by promoting growth changes during the cell cycle, and producing similar tumor-promoting changes at the cellular level [19, 20], and these compounds can directly affect the occurrence and development of tumor.
In summary, an increase in BMI and WHR is associated with the risk for esophageal cancer, and is an important risk factor for esophageal cancer, which is basically consistent with the international study reports. Overweight and obese patients have a signifcantly increased risk of esophageal cancer. Maintaining a normal body weight, following a reasonable diet, and participating in appropriate physical activities can lower the risk for esophageal cancer. Therefore, a change in bad dietary habits is recommended and measures, such as a reasonable diet, balanced nutrition, adequate intake of protein, reduced intake of high energy foods, and keeping a healthy lifestyle, such as participating in more physical activities or sports, can help maintain a normal BMI and WHR, and effectively prevent the occurrence of esophageal carcinoma.
Confict of interest
The authors declare no confict of interest.
1. GLOBOCAN 2012 (IARC): Estimated cancer incidence, mortality and prevalence worldwide in 2012. Section of Cancer Surveillance (25/8/2014). Available from: http://globocan.iarc.fr/Pages/ fact_sheets_population.aspx.
2. Chen WQ, Zhang SW, Zeng HM, Zheng RS, Zou XN, Zhao P, et al. Morbidity and death of malignant tumor in China in 2010. China Cancer 2014;23:1—10.
3. Zhang SW, Zhang M, Li GL, Wei WQ, Meng FS, Liu ZC, et al. Analysis on morbidity and death of esophageal cancer in China from 2003 to 2007. China Cancer 2012;21:1—12.
4. Ji AF, Wang JS, Yang JZ, Ma L, Wei W, Wang LD. Case control study of risk factors of esophageal cancer of residents in southeastern region of Shanxi Province. Mod Prev Med 2012;39:2929—31.
5. Xu JC, Liu GH, Zhou FJ, Miao H, Li L, Sun GX, et al. Case control study of risk factors of esophageal cancer of residents in Xuzhou of Jiangsu Province. Mod Prev Med 2010;37: 1812—914.
6. Freedman ND, Park Y, Subar AF, Hollenbeck AR, Leitzmann MF, Schatzkin A, et al. Fruit and vegetable intake and esophageal cancer in a large prospective cohort study. Int J Cancer 2007;121:2753—60.
7. Gao Y, Hu N, Han XY, Ding T, Giffen C, Goldstein AM, et al. Risk factors for esophageal and gastric cancers in Shanxi Province, China: a case-control study. Cancer Epidemiol 2011;35:e91—9.
8. Steffen A, Schulze MB, Pischon T, Dietrich T, Molina E, Chirlaque MD, et al. Anthropometry and esophageal cancer risk in the European prospective investigation into cancer and nutrition. Cancer Epidemiol Biomarkers Prev 2009;18:2079—89.
9. Corley DA, Kubo A, Zhao W. Abdominal obesity and the risk of esophageal and gastric cardia carcinomas. Cancer Epidemiol Biomarkers Prev 2008;17:352—8.
10. Data summarization and analysis cooperation group of China’s obesity tissue work. Value of prediction of abnormal relevant disease risk factors of adult body mass index and waistline in our country: study on proper body mass index and waistline tangential point. Chin J Epidemiol 2002;23:5—10.
11. Dirani M, Xie J, Fenwick E, Benarous R, Rees G, Wong TY, et al. Are obesity and anthropometry risk factors for diabetic retinopathy? The diabetes management project. Invest Ophthalmol Vis Sci 2011;52:4416—21.
12. Lagergren J, Bergstrom R, Lindgren A, Nyrén O. Symptomatic gastroesophageal refux as a risk factor for esophageal adenocarcinoma. N Engl J Med 1999;340:825—31.
13. Wang B, Zhang Y, Xu DZ, Wang AH, Zhang L, Sun CS, et al. Meta-analysis of smoking, drinking and P53 gene change of esophageal cancer. Chin J Epidemiol 2004;25:775—8.
14. Hardikar S, Onstad L, Blount PL, Odze RD, Reid BJ, Vaughan TL. The role of tobacco, alcohol, and obesity in neoplastic progression to esophageal adenocarcinoma: a prospective study of Barrett’s esophagus. PLoS One 2013;8:e52192.
15. Kimm H, Kim S, Jee SH. The independent effects of cigarette smoking, alcohol consumption, and serum aspartate aminotransferase on the alanine aminotransferase ratio in Korean men for the risk for esophageal cancer. Yonsei Med J 2010;51:310—7.
16. Wu M, Zhao JK, Zhang ZF, Han RQ, Yang J, Zhou JY, et al. Smoking and alcohol drinking increased the risk of esophageal cancer among Chinese men but not women in a high-risk population. Cancer Causes Control 2011;22:649—57.
17. Shi YH, Hou LY, Qiu JL. Meta analysis on case control study of diabetes and esophageal cancer. Chinese General Practice 2013;16:289—91, 297.
18. El-Serag HB, Tran T, Richardson P, Ergun G. Anthropometric correlates of intragastric pressure. Scand J Gastroenterol 2006;41:887—91.
19. Renehan AG, Zwahlen M, Minder C, O’Dwyer ST, Shalet SM, Egger M. Insulin-like growth factor (IGF)-I, IGF binding protein-3, and cancer risk: systematic review and meta-regression analysis. Lancet 2004;363:1346—53.
20. Attoub S, Noe V, Pirola L, Bruyneel E, Chastre E, Mareel M, et al. Leptin promotes invasiveness of kidney and colonic epithelial cells via phosphoinositide 3-kinase-, rho-, and rac-dependent signaling pathways. FASEB J 2000;14:2329—38.
1. Postgraduate Training Base, General Hospital of Shenyang Military Command, Liaoning Medical University, Jinzhou, 110016, China
2. Department of Radiotherapy, General Hospital of Shenyang Military Command, Shenyang, 110000, China
3. Teaching and Research Section, Liaoning Medical University, Jinzhou, 110016, China
Ying Yan
Department of Radiotherapy, General Hospital of Shenyang Military Command, Shenyang, 110000, China
E-mail: yanyingdoctor@sina.com
15 May 2014;
Accepted 22 August 2014
 Family Medicine and Community Health2014年3期
Family Medicine and Community Health2014年3期
- Family Medicine and Community Health的其它文章
- Preparation of a questionnaire for disease knowledge-attitudepractice awareness of patients with remitted schizophrenia based on a structural equation model
- Role of fractional fow reserve in guiding intervention for borderline coronary lesions
- Relationship between obstructive sleep apnea-hypopnea syndrome (OSAHS) and liver fbrosis
- Relationship between fbroblast growth factor 21 and thyroid stimulating hormone in healthy subjects without components of metabolic syndrome
- Family Medicine and Community Health
- Family Medicine and Community Health COCHRANE UPDATES & NICE GUIDELINES