
Changing trends of cardiovascular risk factors among Indians: a review of emerging risks
2014-03-21 07:49:51ArunKumar
Arun Kumar
Department of Biochemistry, Manipal College of Medical Sciences, Pokhara, Nepal
Changing trends of cardiovascular risk factors among Indians: a review of emerging risks
Arun Kumar*
Department of Biochemistry, Manipal College of Medical Sciences, Pokhara, Nepal
ARTICLE INFO
Article history:
Received 20 Sep 2014
Received in revised form 9 Oct 2014
Accepted 12 Oct 2014
Available online 15 Oct 2014
Cardiovascular risk factors
Genetic predisposition
Modifiable risk
Non-modifiable risk
Indians
The global burden of disease due to cardiovascular diseases (CVDs) is escalating, and the changing trends of CVD risk factors are identified among Indians experiencing rapid health transition. Contributory causes include: growing population with demographic shifts and altered age profile, socio-economic factors, lifestyle changes due to urbanization. Indians are also having genetic predisposition to cardiovascular diseases and adult are susceptible to vascular disease linking possible gene-environment interactions influencing ethnic diversity. Altered diets with more of junk foods along with diminished physical activity are additive factors contributing to the acceleration of CVD epidemics, along with all form of tobacco use. The pace of health transition, however, varies across geographical regions from urban to rural population with consequent variations in the relative burdens of the dominant CVDs. A comprehensive public health response must be looked to plan over all strategies to integrate policies and programs that effectively impact on the multiple determinants of CVDs to provide protection over the life span through primordial, primary and secondary prevention. Populations as well as individuals at risk must be protected through initiatives, enable nutritionbased preventive strategies to protect and promote cardiovascular health.
1. Introduction
The global population is projected to rise by 20% from 6.7 billion to 8.1 billion by 2030, but the crude death rate is expected to remain stable at around 8.4 deaths/thousand. However, a major shift is currently underway in the overall disease burden in the world. In 2008, five out of the top ten causes for mortality worldwide were non-communicable diseases (NCDs), which have figured out to be seven out of ten by the year 2030 and majority resides in the developing countries. It is projected that, by the year 2030, about 76% of the deaths in the world would be due to NCDs[1].
Cardiovascular diseases (CVDs) were once thought to be the disease impacting the rich and affluent community, but it is now well established that they afflict the poor as well[2]. Due to urbanization there is a changing trend in lifestyles, blue collar and high demanding jobs, unhealthy eating habits and less physical activity are the key reasons for high incidence rates in the rich population. These diseases not only affect the well being, but canalso retrain the economic growth of the country due to increased healthcare expenditure and diminished productivity.
Even there is increasing availability and focus on curative care in urban areas, this alone cannot clear up the problem of CVDs. The need of the hour is to focus on prevention and its early diagnosis and management and it is not that the health care providers alone can tackle this problem. There is an urgent need for the urban planners, educational institutions, employers, food and beverage industries, wellness and fitness players and above all the government policies to take up the challenge and work towards behaviour and lifestyle changes through positive and negative reinforcements.
In rural India, it is relatively more complex to solve this problem as it needs to create and improve awareness, access and affordability to all in the society. The lack of awareness coupled with the inadequate access to diagnosis leads to a very large number of patients needing tertiary care. The shortage of such high end facilities as well as their inability to pay, leads to high mortality among the rural population.
To solve this problem, urgent development is required to cross the cardiac value chain and collaboration with health care sectors including the Government, pharmaceutical companies, medical technology firms and health insurers. Recent developments have taken place in this direction, with the Government launching theNational NCD programme which would focus on prevention and awareness, and sporadic examples of innovations in medical and mobile technology that allow early detection and monitoring.
2. Global prevalence of CVDs
CVDs comprise of the disorders of the heart and blood vessels and commonly include multifactorial heterogenous conditions such as hypertension, coronary heart disease (CHD), stroke, congestive heart failure, cerebrovascular disease, peripheral arterial disease, rheumatic heart disease, deep vein thrombosis and pulmonary embolism. CVDs are the leading cause of deaths globally with maximum deaths annually. In 2008, CVDs represented 30% (17.3 million) of all deaths globally[3]. CHD and stroke accounted for 7.3 million and 6.2 million deaths of all the global deaths from CVDs, respectively[4]. The projected deaths from CVDs, mainly from heart disease and stroke have been estimated to reach 23.3 million by 2030[5].
3. Prevalence of CVDs in Indian subcontinent
Eighty percent of CVD related deaths are being reported from low and middle income countries like India[3]. The incidence of CVD is increasing everyday and 25% of all mortality is due to coronary artery disease. Population surveys from India have reported 9-fold increase in its prevalence and expected to cause doubling of deaths due to CVD by 2015 (Figure 1)[6].
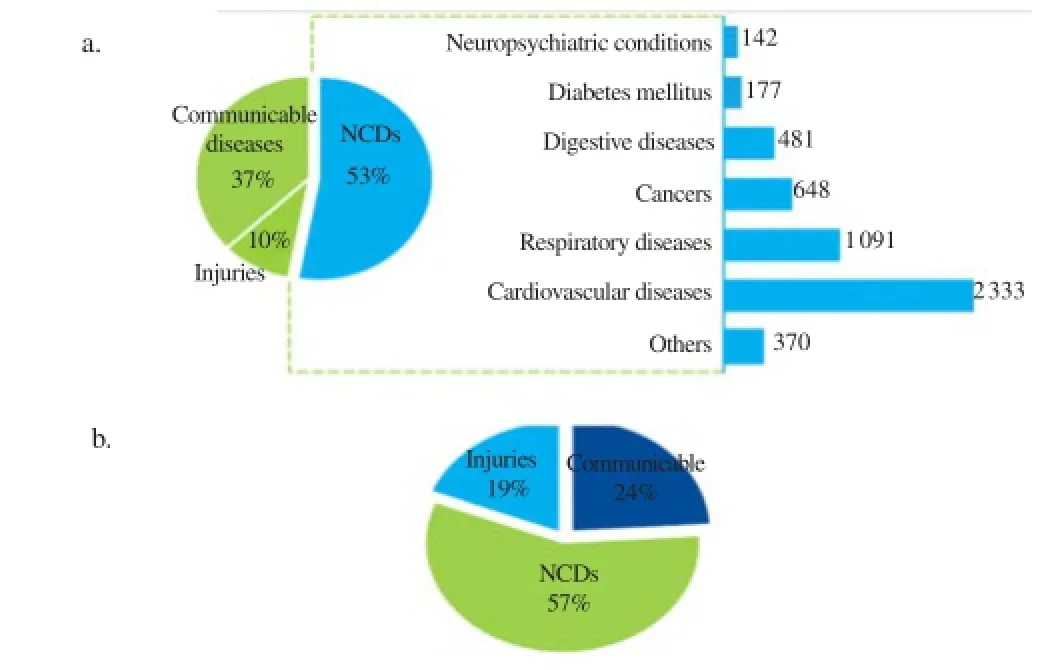
Figure 1.Prevalence of CVDs in India.a: Deaths in 2008 due to CVDs; b: Estimated disease burden in India by 2020.
4. Indians and cardiovascular risk
The concept of cardiovascular risk factors was first introduced in 1961 from the Framingham Heart Study, linking the presence of specific parameters like elevated cholesterol, hypertension, diabetes mellitus, tobacco use. Asian Indian lineage accounts for over onefifth of the world population[7]. Asian Indian phenotype is marked by combination of clinical (larger waist-to-hip and waist-to-height ratios signalling excess visceral adiposity), biochemical [insulin resistance, lower adiponectin and higher C-reactive protein (CRP) levels], and metabolic aberrations [raised triglycerides (TGs), lowand high-density lipoprotein-cholesterol (HDL-c)][8]. The growing prevalence of heart diseases in India can be attributed to presence of high lipoprotein, environmental and lifestyle risk factors in Indian population[8,9]. Inclinations to metabolic syndrome is another important reason for higher incidences of CVD in Indian population[8,10].
5. Genetic pre-disposition among Indians in the development of CVDs
Several studies have documented that mutation in specific genes result in early development of CVDs. On genetic analysis of hyperlipidemic patients a correlation was found in the development of CVD due to interaction of inherited hyperlipidemic genes and environmental factors like stress, unhealthy diet, smoking and sedentary life styles[11].
Some important CVD associated genetic variants are discussed below.
5.1. Lipoprotein associated genes
5.1.1. Lipoprotein lipase (LPL) gene
This gene is located on chromosome 8p22. It produces an enzyme LPL, which hydrolyses TG rich lipoproteins, thus clearing the latter from circulation. The occurrence of four different substitution mutations, viz., Gly188Glu, Asn291Ser, Asp9Asn and Ser447Ter has been reported in different studies[11]. The Asn291Ser substitution increases risk of myocardial infarction and also severity of atherosclerosis[12]. According to a meta-analysis, substitutions in Gly188Glu, Asn291Ser and Asp9Asn support an atherogenic lipoprotein profile with disease risk in heterozygous carriers of Gly188Glu, and borderline risk in other two types. However, the Ser447Ter showed an opposite trend. For the first three substitutions this differential activity on lipoprotein profiles maybe because the mutations occur at N terminal end (responsible for the enzyme catalytic activity). Contrary to this, Ser447Ter substitution occurs at the C terminal end and thus possibly influences uptake of lipoproteins by receptors[13].
Hypertension is one of the major risk factors for CVDs. LPL provides fatty acids (FA) through TG hydrolysis as the energy substrate for cardiac cells. A variant X447, in which two amino acids are deleted from the C terminal, is more efficient in TG hydrolysis thus providing protecting against CVD by sustaining low levels of TG and FA. However, in hypertensive individuals with the variant X447, even though the TG levels are lower than those hypertensives with normal S447, the FA levels are significantly higher. Subsequently, an overburden of uncleared FA results in an increased risk of CVD[14].
5.1.2. Low density lipoprotein receptor genes (LDLR)
LDLR gene is located on chromosome 19. Mutation in LDLR gene causes familial hypercholesterolemia, which is dose dependent autosomal dominant disorder, occurs at less than 60 years of age[15]. Atherosclerosis susceptibility, also known as atherogenic lipoprotein phenotype, is closely linked to LDLR locus.
5.1.3. Apolipoprotein genes
Apolipoproteins occur in two isoforms: Apo-48 and Apo-B100. The polymorphisms in apoliporotein gene may lead to increased risk of CVD. Apo-100 is a principal protein component of low density lipoprotein and is responsible for mediating cholesterol homeostasis. Four common polymorphisms, identified in its gene include: MspI (in codon 3611, amino acid change from arginine to glutamine); XbaI (exon 26, A→T in threonine codon, silent mutation); EcoRI (exon 29, GAA AAA; 4,154th nucleotide, Glu→Lys); 3’ HVR (multiallelic locus with tandem repeats 11 to 16 bp AT-rich DNA sequences beginning 73 bp, 3′ to second polyadenylation signal).
The presence of these mutations is correlated significantly with unfavorable lipid profiles which include high cholesterol and TG levels along with decreased concentrations of high density lipoprotein[16].
5.1.4. Apolipoprotein E genes
Apolipoprotein E genes play a major role in cholesterol and TG metabolism. A common polymorphism in this gene codes for 3 isoforms E2, E3 and E4 with equivalent allele ε2, ε3 and ε4, located on chromosome 19. Studies report that ε4 is associated with a slightly higher risk of CVD in both genders[17-19].
5.2. Endothelial nitric oxide synthase gene (eNOS)
Vascular endothelial dysfunction is a common characteristic of various CVDs. The maintenance of vascular homeostasis considerably depends on the bioavailability of endothelium-derived nitric oxide synthesized by endothelial nitric oxide synthase (eNOS). This enzyme has been implicated in pathogenesis of CVD. The eNOS variants in the 7q35-q36 region have been investigated for their association with CVD, especially hypertension[20].
The association of eNOS exon 7 Glu298Asp polymorphism with high risk for CVD has been reported in North Eastern Indian population with homozygous GG wild genotype as predominant
one[21].
5.3. Myocyte enhancer factor 2 gene (MEF 2)
MEF 2 transcription factor plays a major role in regulation of gene expression in multiple muscle cell types. Four MEF 2 genes (A, B, C, and D) have been identified[11], and the corresponding protein is strongly expressed in the coronary artery endothelium. The CVD pathogenesis is mediated by a seven amino acid deletion in this gene which reduces transcription activation and thus involvement of MEF2A signaling pathway[22].
5.4. Methylene tetrahydrofolate reductase gene (MTHFR)
MTHFR regulates folate-dependent homocysteine remethylation. Its deficiency causes hyperhomocysteinemia. Homozygous 677C→T mutation in MTHFR gene is associated with premature cardiovascular disease risk[23].
5.5. CYP11B2 and CYP2D6
CYP11B2 gene plays a major role in the regulation of renin angiotensin system as it encodes for aldosterone synthase enzyme responsible for aldosterone synthesis which is a main effecter in renin angiotensin system. Any disruption in the genetic loci of this enzyme results in enhanced aldosterone synthesis and consequently elevated blood pressure which precipitates CVD. Studies have documented a significant association between CYP11B2 polymorphism and essential hypertension in males which may consequently lead to CVD[24].
6. Risk factors for CVDs: an Indian perspective
Conventional risk factors for CVDs are broadly classified into two categories: modifiable and non-modifiable[25]. Modifiable risk factors can reduce the CVD risk if treated and controlled, while nonmodifiable risk factors could not be modified to reduce the CVD burden. The existing risk factors were based on three primary criteria: high prevalence in different populations; significant independent impact on the risk of CVD; and reduced cardiovascular risk with treatment and control[9]. The major non-modifiable risk factors for CVDs in Indian population include: advancing age, heredity factors family history, gender, ethnicity. The major modifiable risk factors for CVDs in Indian population includes two major aspects, i.e.: modifiable cardiometabolic risk factors (hypertension, dyslipidemia, diabetes mellitus, obesity) and modifiable lifestyle risk factors (smoking, less physical activity, nutrition, low social economic status).
CVD population groups exhibit a cluster of cardiometabolic risk factors, which are linked with a number of modifiable lifestyle risk factors (Figure 2). Multiple studies have revealed that modifiable risk factors are responsible for a large number of premature deaths due to CVD[26].
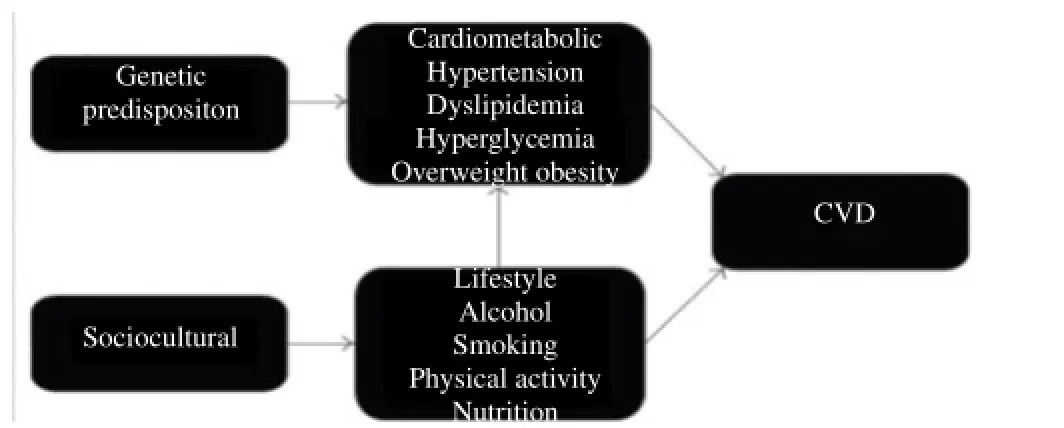
Figure 2.Causative pathways for CVD[26].
6.1. Modifiable cardiometabolic risk factors
6.1.1. Hypertension
Hypertension is a major risk factor for CVDs, including stroke and myocardial infarction, and its burden is increasing disproportionately in developing countries as they undergo demographic shift. For every 20 mmHg systolic or 10 mmHg diastolic increase in resting blood pressure there is a two-fold increase in risk of death fromischemic heart disease or stroke. Hypertension has been shown to cause decreased vascular fulfilment and endothelial injury[27]. Hypertension is considered to occur due to interaction of number of factors like anthropometry measurement, lipid profile, dietary vitamins, serum antioxidants, lipoprotein (a) and lipid peroxides and rise in oxidative stress. Results of a study conducted on 345 elderly hypertensive South Asian patients aged 56-64 years have shown that dietary vitamin intake was higher in hypertensive patients compared to normotensive controls. Besides, a significant difference was observed in anthropometric variables. The lipid profile showed a significant increase in total cholesterol, low density lipoproteins-cholesterol (LDL-c), TG in hypertensive patients (P<0.001). The serum endogenous antioxidants and enzyme antioxidants were also significantly decreased in hypertensive patients as compared to normotensive patients[28]. Another study was conducted on 86 elderly hypertensive patients aged 56-64 years to evaluate ischemia modified albumin as prognostic marker of to avoid future coronary complications, which showed significantly higher ischemia modified albumin levels in hypertensive patients as compared to normotensive controls (P<0.001)[29]. The carbonic anhydrase activity in hypertensive patients has also been show to be highly significant (P<0.001) as compared to that in the healthy controls[30].
6.1.2. Dyslipidemia
The association between dyslipidemia and CVDs is well established and particular among these abnormalities are elevated levels of LDL-c main risk factor of CVD. Asians experience the major proportion of the worldwide burden of CVD. This necessitates proper management of LDL-c, HDL-c and also TG subfractions[31-33]. The utility of lipid ratios as predictors of future risk of CHD risk in normolipidemic myocardial infarct (MI) patients has been documented in published studies. One such study compared lipid profile of 1 021 elderly normolipidemic MI patients with age/sex matched controls. Total cholesterol, TGs, LDL-c and HDL-c were estimated in the study. A significantly higher total cholesterol, total cholesterol/HDL-c ratio, TG, LDL-c and LDL-c/HDL-c ratio was observed in MI patients as compared to healthy controls (P<0.001)[34]. Also, the clinical data is suggestive of higher levels of lipid peroxidation markers (malondialdehyde and conjugated dienes), antioxidants and inflammatory markers in normolipidemic acute myocardial infarction (AMI) patients than controls. Results of these studies show the higher levels of lipoprotein (a), ceruloplasmin, CRP, fibrinogen, malondialdehyde and conjugated dienes whereas lower levels of bilirubin, ascorbic acid, uric acid, albumin, superoxide dismutase, catalase, glutathione peroxidise and paraoxonase-1 activities AMI patients than controls[35,36].
6.1.3. Diabetes mellitus
One of the main risk factor having distinctive association with CHD is diabetes, particularly its predominant form, type 2 diabetes mellitus. A two- to four-fold higher risk of developing CHD has been documented with diabetics than people without diabetes, and CVD accounts for 65%-75% of deaths in people with diabetes.
Moreover, the age- and sex-adjusted mortality risk in diabetic patients without pre-existing CHD was found to be equal to that of non-diabetic individuals with prior MI. These findings regarding higher risk of mortality are suggestive of common precursors to diabetes and CHD, with following implications that insulin resistance, visceral adiposity, and excess inflammation are characteristic pathophysiology of thrombogenesis. Besides, a complex mix of mechanisms such as oxidative stress, enhanced atherogenecity of cholesterol particles, abnormal vascular reactivity, increased haemostatic activation, and renal dysfunction have been considered as features characteristic of type 2 diabetes mellitus that may confer excess risk of CHD.
The typical “Asian Indian phenotype” refers to a combination of clinical (larger waist-to-hip and waist-to-height ratios indicating excess visceral adiposity), biochemical (insulin resistance, lower adiponectin, and higher CRP levels) and metabolic abnormalities (higher TG, LDL-c/HDL-c) that are more prevalent in individuals of South Asian origin and thus inclination of this group for developing diabetes and premature CHD. The protective female gender effect is lost in diabetic subjects, and women with diabetes are possibly more prone to develop coronary artery disease than men with diabetes[32,33].
6.1.4. Obesity
Body-mass index (BMI) may not truly reflect obesity in Indians as obesity is characterized by higher waist-hip ratios and higher body fat percentage at given level of BMI. Non-obese (BMI<25 kg/m2) Asian Indians with normal waist circumference have high CVD risk. The traditional cut-off point of BMI of 25 might not define overweight and obesity optimally in Asian Indians as they have higher percentage of body fat compared to whites[37]. Obesity might act a risk factor for heart failure through different mechanisms like increased total blood volume, increased cardiac output, left ventricular hypertrophy, left ventricular diastolic dysfunction, adipositas cordis[38].
6.2. Modifiable life style risk factors
6.2.1. Smoking
Smoking is estimated to kill five million people worldwide each year[39], and is an established risk factor since 1940s[40]. Smoking is estimated to cause nearly 10% of all CVD[41]. The risk of developing CVD is higher in female smokers, young men and chronic smokers[42].
There are multiple mechanisms which can contribute to CVD risk factors when one is a smoker. It can cause atherosclerosis, vascular injury, vascular dysfunction, and thrombosis although the precise mechanisms are yet to be unveiled[43]. Cigarette smoking increases the incidence of CVD in a dose-dependent manner[44-46], with even occasional smoking increasing the risk of CVD[47]. Even the risk reduction is documented by long-term prospective studies bycessation of smoking[48]. Study conducted by Kumar and Biswas on evaluation of parameters associated with CVD in smoker and non-smoker showed a highly significant decrease in paraoxonase activity[49], antioxidant status and elevation of lipid peroxides among smokers which are associated with cardiovascular risks.
6.2.2. Physical activity
Physical inactivity is responsible for almost 12% of the global burden of myocardial infarction[50]. The relative risk of CVD is reduced in regular physical activity[51-56]. Study conducted and reported from thirteen cities in India by Shah and Mathur (2010) showed lower physical activity among both sexes of urban population compared to rural ones[57]. The American College of Sports Medicine recommends at least 30 min of moderate-intensity physical activity for at least 5 d a week[58].
6.2.3. Nutrition
Poor dietary habits affect multiple cardiovascular risk factors including blood pressure, cholesterol levels, glucose levels, and obesity[59-65]. A diet high in nutrient rich (vitamins, minerals, antioxidants and fibre) fruits and vegetables can reduce the risk for many leading causes of death[59-65]. In meta-analyses of prospective cohort studies, each daily serving of fruits or vegetables was associated with a 4% lower risk of CHD (RR 0.96, 95% CI: 0.93 to 0.99) and a 5% lower risk of stroke (RR: 0.95, 95% CI: 0.92 to 0.97)[59,60]. Five or more daily servings of fruits and vegetables are recommended for optimal nutrition[60,61]. In a study conducted by Kumar et al. (2010), where the goal of the study was to address the association between dietary vitamin and cardiovascular risk in normolipidemic acute MI patients compared with healthy controls. The study observed that dietary intake of vitamin A, B1, B2, B3 was significantly higher in AMI patients compared to healthy controls but the intake of vitamin C was significantly higher in controls compared to AMI patients. Even though the vitamins intake was higher in patients, the associated cardiovascular risk factors were not reduced compared to controls. The study further concluded that diets rich in vegetables and fruits do not seem to reduce the cardiovascular risk in normolipidemic AMI patients[66].
7. Overall outlook
There are more than 1.27 billion people across India. More than 50% of the current Indian population is below age of 25 years and 65% is below 35 years. About 72.2% of the population lives in some 638 000 villages and the rest 27.8% in about 5 480 towns and urban agglomerations. Apart from India, indigenous population is distributed in 70 countries worldwide, in India there is a significant variation between and within peoples in terms of education, socioeconomic status, living conditions, and familial factors. In spite of diversity, they do share a striking commonality but there is a discrepancy in life expectancy. A higher prevalence of CVD may be considered the driving force behind this discrepancy, which is being aggravated by their lifestyle and subsequent cardiometabolic risk factors among them.
The populations from each of the states ranging from urban to rural and semi-rural with age group varying from 25 years to 65 years exhibits a cluster of cardiometabolic conditions. Most of them share common factors like higher rates of obesity and diabetes, hypertension and high cholesterol is greater among the urban population compared to the rural ones. While each of these factors have been reported to be independently associated to enhance the risk of CVD, the effects are also thought to be additive. Poor lifestyle choices, lack of awareness among rural community might herald and contribute to these cardiometabolic outcomes.
While smoking rates have fallen among Indian men, they have risen among women. Smoking can be attributed to rising cases of infertility and higher risk of cancer among Indian women these days in addition to cardiovascular risk. Research study examined the prevalence of smoking in 187 countries between 1980 and 2012 and found that while cigarette smoking among Indian men has fallen from 33.8% in 1980 to 23% in 2012, it has risen from 3% to 3.2% among Indian women within the same time frame. In other words, the number of female smokers in India has doubled from about 5.3 million to 12.2 million in the same period of time. This trend is more visible in the urban areas as; women in rural areas have the trend of consuming smokeless tobacco in large numbers. Compared to other countries, Indians also exhibit dangerous alcohol consumption behaviour, as well as lower consumption of fruits and green leafy vegetables.
Other factors include sedentary life styles especially among urban population.
Holistic strategies which delineate the interactions between lifestyle factors might help in promoting positive changes among the people who are at risk. Recently published systematic review reported that physical activity interventions have only small effect on children’s overall activity. Lifestyle changes and strategies to inculcate more of physical activities should be linked up with daily physical activity as well as lifestyle factors, including nutrition and sleep behaviour each of which may be influenced by increased physical activity levels and may affect cardiometabolic outcomes.
In order to maximize potential positive outcomes, strategies which aim to promote positive changes in lifestyle should not only be physiologically appropriate; they should also be sensitive to sociocultural norms.
The strategies implemented to promote lifestyle changes must be specific to a group or an individual and not to the population as a whole, especially when a geographical area includes different language and culturally distinct groups. Diversity competence involves knowledge, skills, and abilities that enable a researcher to deal with a specific population.
Since we are heading towards middle of 21st century, we need to be cautioned and alarmed of the prevailing risk factors existing in our society and the message should be disseminated to all through social media so that the community and individuals should not be ignorant of the strategies to maintain a disease free and a healthy livelihood.
Conflict of interest statement
I declare that I have no conflict of interest.
[1] World Health Organization. Prevention of diabetes mellitus-report of a WHO study group. WHO Technical Report Series no. 844. Geneva: World Health Organization; 1994. [Online] Available from: http:// whqlibdoc.who.int/trs/WHO_TRS_844.pdf [Accessed on 27th March, 2014]
[2] Ali SS, Mishra PK. Management strategies for treatment of cardiovascular diseases in India: a review.Biosci Biotech Res Comm2013;6(2): 170-173.
[3] World Health Organization. Global status report on noncommunicable diseases 2010-description of the global burden of NCDs, their risk factors and determinants. Geneva: World Health Organization; 2011. [Online] Available from: http://www.who.int/nmh/publications/ncd_ report2010/en/ [Accessed on 9th March, 2014]
[4] World Health Organization. Global atlas on cardiovascular disease prevention and control-policies, strategies and interventions. Geneva: World Health Organization; 2011. [Online] Available from: http://www. who.int/cardiovascular_diseases/publications/atlas_cvd/en/ [Accessed on 9th March, 2014]
[5] Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030.PLoS Med2006;3(11): e442.
[6] Dr Ram Manohar Lohia Hospital and associated Postgraduate Institute of Medical Education and Research. National programme for prevention and control of diabetes, cardiovascular disease and stroke. Guidelines on assessment and management of cardiovascular risk for medical officers. New Delhi: Dr Ram Manohar Lohia Hospital and associated Postgraduate Institute of Medical Education and Research. [Online] Available from: http://www.searo.who.int/india/topics/cardiovascular_ diseases/NCD_Resources_CVD_RISK_MANAGEMENT_BOOKLET. pdf [Accessed on 7th March, 2014]
[7] Deloitte. Cardiovascular diseases in India-challenges and way ahead. International heart protection summit 2011. Mumbai: Deloitte; 2011. [Online] Available from: https://www.deloitte.com/assets/Dcom-India/LocalAssets/Documents/Cardiovascular_diseases_in_India.pdf [Accessed on 7th March, 2014]
[8] Enas EA, Singh V, Munjal YP, Gupta R, Patel KC, Bhandari S, et al. Recommendations of the second Indo-US health summit on prevention and control of cardiovascular disease among Asian Indians.Indian Heart J2009;61: 265-274.
[9] Gupta S, Gudapati R, Gaurav K, Bhise M. Emerging risk factors for cardiovascular diseases: Indian context.Indian J Endocrinol Metab2013;17(5): 806-814.
[10] Forouhi NG, Sattar N. CVD risk factors and ethnicity: a homogeneous relationship?Atheroscler Suppl2006;7: 11-19.
[11] Sai RA, Dhamodaran V, Thiagarajan P. Role of genetic variants in development of cardiovascular diseases.Int J Pharm Sci Health Care2012;1(2): 45-53.
[12] Jemaa R, Fumeron F, Poirier O, Lecerf L, Evans A, Arveiler D, et al. Lipoprotein lipase gene polymorphisms: associations with myocardial infarction and lipoprotein levels, the ECTIM study. Etude Cas Témoin sur l’Infarctus du Myocarde.J Lipid Res1995;36: 2141-2146.
[13] Wittrup HH, Tybj?rg-Hansen A, Nordestgaard BG. Lipoprotein lipase mutations, plasma lipids and lipoproteins, and risk of ischemic heart disease: a meta-analysis.Circulation1999;99: 2901-2907.
[14] Talmud PJ, Flavel DM, Alfakih K, Cooper JA, Balmforth AJ, Sivananthan M, et al. The lipoprotein lipase gene serine 447 stop variant influences hypertension-induced left ventricular hypertrophy and risk of coronary heart disease.Clin Sci (Lond)2007;112: 617-624.
[15] Melissa AA, Hutter CM, Zimmern RL, Humphries SE. Familial hypercholesterolemia and coronary heart disease: a huge association review.Am J Epidemiol2004;160(5): 421-429.
[16] Singh VP, Ramesh V, Somvanshi S, Tewari S, Khan F, Sinha N, et al.
Association of DNA polymorphism at the apolipoprotein B-100 gene locus with plasma lipid concentration and coronary artery disease among North Indians.Am J Biochem Biotechnol2006;2(4): 138-145.
[17] Wilson PWF, Schaefer EJ, Larson MG, Ordovas JM. Apolipoprotein E alleles and risk of coronary disease-a meta-analysis.Arterioscler Thromb Vasc Biol1996;16: 1250-1255.
[18] Kolovou G, Damaskos D, Anagnostopoulou K, Cokkinos DV. Apolipoprotein E gene polymorphism and gender.Ann Clin Lab Sci2009;39(2): 120-133.
[19] Bennet AM, Angelantonio E, Ye Z, Wensley F, Dahlin A, Ahlbom A, et al. Association of apolipoprotein E genotypes with lipid levels and coronary risk.JAMA2007;298(11): 1300-1311.
[20] Bhanoori M. Endothelial nitric oxide synthase (eNOS) variants in cardiovascular disease: pharmacogenomic implications.Indian J Med Res2011;133: 464-466.
[21] Shankarishan P, Borah PK, Ahmed G, Mahanta J. Prevalence of endothelial nitric oxide synthase (eNOS) gene exon 7 Glu298Asp variant in North Eastern India.Indian J Med Res2011;133: 487-491.
[22] Wang L, Fan C, Topol SE, Topol EJ, Wang Q. Mutation of MEF2A in an inherited disorder with features of coronary artery disease.Science2003;302: 1578-1581.
[23] Kluijtmans LA, van den Heuvel LP, Boers GH, Frosst P, Stevens EM, van Oost BA, et al. Molecular genetic analysis in mild hyperhomocysteinemia: a common mutation in the methylenetetrahydrofolate reductase gene is a genetic risk factor for cardiovascular disease.Am J Hum Genet1996;58: 35-41.
[24] Rajan S, Ramu P, Umamaheswaran G, Adithan C. Association of aldosterone synthase (CYP11B2 C-344T) gene polymorphism & susceptibility to essential hypertension in a south Indian Tamil population.Indian J Med Res2010;132: 379-385.
[25] Gupta S, Gudapati R, Gaurav K, Bhise M. Emerging risk factors for cardiovascular diseases: Indian context.Indian J Endocrinol Metab2013;17(5): 806-814.
[26] Lucero AA, Lambrick DM, Faulkner JA, Fryer S, Tarrant MA, Poudevigne M, et al. Modifiable cardiovascular disease risk factors among indigenous populations.Adv Prev Med2014; doi: 10.1155/2014/547018.
[27] Maraj I, Makaryus JN, Ashkar A, McFarlane SI, Makaryus AN. Hypertension management in the high cardiovascular risk population.Int J Hypertens2013; doi: 10.1155/2013/382802.
[28] Kumar A. Correlation between anthropometric measurement, lipid profile, dietary vitamins, serum antioxidants, lipoprotein (a) and lipid peroxides in known cases of 345 elderly hypertensive South Asian aged 56-64 y- a hospital based study.Asian Pac J Trop Biomed2014;4(Suppl 1): S189-S197.
[29] Kumar A. Prognostic implications of ischemia modified albumin in known cases of 86 elderly hypertensive South Asian aged 56-64 years - a hospital based study.Asian Pac J Trop Dis2014;4(Suppl 1): S429-S434.
[30] Biswas UK, Kumar A. A study on lipid profile, oxidation stress and carbonic anhydrase activity in patients with essential hypertension.J Clin Diagn Res2010;4: 3414-3420.
[31] Karthikeyan G, Teo KK, Islam S, McQueen MJ, Pais P, Wang X. Lipid profile, plasma apolipoproteins, and risk of a first myocardial infarction among Asians an analysis from the INTERHEART study.J Am Coll Cardiol2009;53: 244-253.
[32] Ali MK, Venkat Narayan KM, Tandon N. Diabetes & coronary heart disease: current perspectives.Indian J Med Res2010;132: 584-597.
[33] Mohan V, Venkatraman JV, Pradeepa R. Epidemiology of cardiovascular disease in Type 2 diabetes: the Indian scenario.J Diabetes Sci Technol2010;4(1): 158-170.
[34] Kumar A, Biswas UK, Nagtilak S, Ramiah S. Lipid ratio useful indicator in predicting risk of myocardial infarction in elderly normolipidemic patients: a report from a multi center study.Asian Pac J Trop Dis2011;1: 123-126.
[35] Kumar A, Nagtilak S, Sivakanesan R, Gunasekera S. Cardiovascular risk factors in elderly normolipidemic acute myocardial infarct patients - a case controlled study from India.Southeast Asian J Trop Med Public Health2009;40(3): 581-592.
[36] Kumar A, Sivakanesan R, Gunasekera S. Oxidative stress and antioxidant status in normolipidemic AMI patients.Indian J Clin Biochem2008;23(3): 296-298.
[37] Joshi PP. Why is coronary heart diseases increasing in Indians? Cardiovascular risk factors in the Indian scenario.South Asian J Prev Cardiol2003;7: 4.
[38] Poirier P, Giles TD, Bray GA, Hong YL, Stern JS, Pi-Sunyer FX, et al. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss. AHA summary statement.Arterioscler Thromb Vasc Biol2006;26: 968-976.
[39] Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030.PLoS Med2002;3: e442.
[40] Law MR, Morris JK, Wald NJ. Environmental tobacco smoke exposure and ischaemic heart disease: an evaluation of the evidence.BMJ1997;315(7114): 973-980.
[41] World Health Organization, World Heart Federation, World Stroke Organization. Global atlas on cardiovascular disease prevention and control. Geneva: World Health Organization; 2011. [Online] Available from: http://www. who.int/cardiovascular_diseases/publications/atlas_cvd/en/ [Accessed on 9th March, 2014]
[42] Teo KK, Ounpuu S, Hawken S, Pandey MR, Valentin V, Hunt D, et al. Tobacco use and risk of myocardial infarction in 52 countries in the INTERHEART study: a case-control study.Lancet2006;368(9536): 647-658.
[43] Ambrose JA, Barua RS. The pathophysiology of cigarette smoking and cardiovascular disease: an update.J Am Coll Cardiol2004;43(10): 1731-1737.
[44] Conen D, Everett BM, Kurth T, Creager MA, Buring JE, Ridker PM, et al. Smoking, smoking cessation, and risk for symptomatic peripheral artery disease in women: a cohort study.Ann Intern Med2011;154(11):719-726.
[45] Lee YH, Shin MH, Kweon SS, Choi JS, Rhee JA, Ahn HR, et al. Cumulative smoking exposure, duration of smoking cessation and peripheral arterial disease in middle-aged and older Korean men.BMC Public Health2011;11: 94.
[46] Tomiyama H, Hashimoto H, Tanaka H, Matsumoto C, Odaira M, Yamada J, et al. Continuous smoking and progression of arterial stiffening: a prospective study.J Am Coll Cardiol2010;55(18):1979-1987.
[47] Stoner L, Sabatier MJ, Black CD, McCully KK. Occasional cigarette smoking chronically affects arterial function.Ultrasound Med Biol2008;34(12): 1885-1892.
[48] Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors.J Epidemiol Community Health2004;58(11): 930.
[49] Kumar A, Biswas UK. Smoking is associated with reduced serum paraoxonase, antioxidants and increased oxidative stress in normolipidaemic acute myocardial infarct patients.Heart Asia2011;3: 115-119.
[50] Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study.Lancet2004;364(9438): 937-952.
[51] Sattelmair J, Pertman J, Ding EL, Kohl HW, Haskell W, Lee IM. Dose response between physical activity and risk of coronary heart disease: a meta-analysis.Circulation2011; doi: 10.1161/ CIRCULATIONAHA.110.010710.
[52] Mansikkaniemi K, Juonala M, Taimela S, Hirvensalo M, Telama R, Huupponen R, et al. Cross-sectional associations between physical activity and selected coronary heart disease risk factors in young adults. the cardiovascular risk in young finns study.Ann Med2011;44(7): 733-744.
[53] Moholdt T, Wisloff U, Nilsen TI, Slordahl SA. Physical activity and mortality in men and women with coronary heart disease: a prospective population-based cohort study in Norway (the HUNT study).Eur J Cardiovasc Prev Rehabilit2008;15(6): 639-645.
[54] Church T. Exercise in obesity, metabolic syndrome, and diabetes.Prog Cardiovasc Dis2011;53(6): 412-418.
[55] Carroll S, Dudfield M. What is the relationship between exercise and metabolic abnormalities? A review of the metabolic syndrome.Sports Med2004;34(6): 371-418.
[56] Long AN, Dagogo-Jack S. Comorbidities of diabetes and hypertension: mechanisms and approach to target organ protection.J Clin Hypertens2011;13(4): 244-251.
[57] Shah B, Mathur P. Surveillance of cardiovascular disease risk factors in India: the need & scope.Indian J Med Res2010;132: 634-642.
[58] Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, et al. American college of sports medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise.Med Sci Sports Exerc2011;43(7): 1334-1359.
[59] He FJ, Nowson CA, Lucas M, Mac Gregor GA. Increased consumption of fruit and vegetables is related to a reduced risk of coronary heart disease: meta-analysis of cohort studies.J Human Hypertens2007;21(9): 717-728.
[60] Dauchet L, Amouyel P, Hercberg S, Dallongeville J. Fruit and vegetable consumption and risk of coronary heart disease: a metaanalysis of cohort studies.J Nutr2006;136(10): 2588-2593.
[61] Dauchet L, Amouyel P, Dallongeville J. Fruit and vegetable consumption and risk of stroke: a meta-analysis of cohort studies.Neurology2005;65(8):1193-1197.
[62] Nishida C, Uauy R. WHO scientific update on health consequences of trans fatty acids: introduction.Eur J Clin Nutr2009;63(Suppl 2): S1-S4.
[63] Mitrou PN, Kipnis V, Thiebaut AC, Reedy J, Subar AF, Wirf?lt E, et al. Mediterranean dietary pattern and prediction of all-cause mortality in a US population: results from the NIH-AARP diet and health study.Arch Int Med2007;167(22): 2461-2468.
[64] Keast DR, O’Neil CE, Jones JM. Dried fruit consumption is associated with improved diet quality and reduced obesity in US adults: national health and nutrition examination survey, 1999-2004.Nutr Res2011;31(6): 460-467.
[65] ESPGHAN Committee on Nutrition, Agostoni C, Braegger C, Decsi T, Kolacek S, Koletzko B, et al. Role of dietary factors and food habits in the development of childhood obesity: a commentary by the ESPGHAN committee on nutrition.J Pediatr Gastroenterol Nutr2011;52(6): 662-669.
[66] Kumar A, Sivakanesan R. Cardiovascular risk factors in normolipidemic acute myocardial infarct patients on admission -do dietary fruits and vegetables offer any benefits?Online J Health Allied Sci2010;9(3): 1-8.
*Corresponding author: Dr. Arun Kumar, Associate Professor, Department of Biochemistry, Manipal College of Medical Sciences, Pokhara, Nepal.
Tel: +977-9816664537
E-mail: arun732003@gmail.com
Foundation Project: Supported by a grant from Confederation of Epidemiological Associations registered under Govt of Kerala (Grant number: 30-956/2013 CEA).
10.12980/APJTB.4.201414B401
 Asian Pacific Journal of Tropical Biomedicine2014年12期
Asian Pacific Journal of Tropical Biomedicine2014年12期
- Asian Pacific Journal of Tropical Biomedicine的其它文章
- An unusual cause of optic neuritis: rickettsiosis disease
- Seroprevalence of syphilis in patients attending a tertiary care hospital in Southern India
- Histopathological and molecular study of Neospora caninum infection in bovine aborted fetuses
- Genetic polymorphisms of GSTM1, GSTP1 and GSTT1 genes and lung cancer susceptibility in the Bangladeshi population
- Expression of p-PPARγ in the aging thoracic aorta of spontaneously hypertensive rat and inhibitory effect of rosiglitazone
- In vitro germination and propagation of a threatened medicinal orchid, Cymbidium aloifolium (L.) Sw. through artificial seed