
Giant Hydroureteronephrosis Associated with Ipsilateral Inguinal Hernia and Contralateral Hydronephrosis:a Case Study
2010-11-18 13:32:52ZhiqiangWangXiaohongDongBaizhiYangandXiuhongWang
Chinese Medical Sciences Journal 2010年4期
Zhi-qiang Wang*,Xiao-hong Dong,Bai-zhi Yang,and Xiu-hong Wang
Department of Urology,Shouguang Hospital of Traditional Chinese Medicine,Shouguang 262700,China
GIANT hydronephrosis is a rare urological entity.It was first defined as the presence of more than 1 000 mL of fluid in the collecting system.1That disease is seen more often in males than in females (2.4∶1) and more often on the left side than on the right side (1.8∶1).2It is usually secondary to ureteropelvic junction obstruction,stone,or congenital abnormality.Among the etiologies of giant hydroureteronephrosis,obstruction of ectopic ureteral orifice into prostatic urethra is a very rare one.Most of the cases are diagnosed and treated in infancy or childhood.However,some patients remain asymptomatic until later in life.Adults may present with intermittent abdominal or flank pain,renal insufficiency,urinary tract infection,or gross hematuria after minor trauma.3,4Here we report a unique case of a giant hydroureteronephrosis associated with ipsilateral inguinal hernia and contralateral hydronephrosis to contribute to better understanding of this disease.
CASE DESCRIPTION
A 32-year-old obese man complained of a reducible lump at left groin,which was intermittently painful and had been growing over 8 months.He presented no urinary symptoms,and denied any history of incontinence,ureteral trauma,urinary tract infection,instrumentation,or surgical intervention.At physical examination a reducible swelling with a cough impulse was identified at left groin.No palpable abdominal masses were found.Examination of the external genitalia produced no remarkable results.Serum creatinine level was 1.4 mg/dL and other biochemical results were within the reference ranges.
An abdominal ultrasound scan revealed a severe right hydronephrosis with dilated proximal ureter.A multicystic,multiseptate,helicoidal mass was found originating from the left renal hilum and extending to the pelvic floor,which was verified in computed tomography (CT) (Fig.1).His renal function was evaluated using mercaptoacetyltriglycine renal scintigraphy,which exhibited an equal contribution from both kidneys.Cystoscopy revealed a craniolateral ureteral orifice on the left.In urethroscopy,an ectopic orifice was found in the prostatic urethra,proximal to the seminal colliculus.We failed to pass even a 3F ureteral catheter through the orifice.
The severe right hydronephrosis with dilated proximal ureter in this case was suspected to result from the pression of the left hydroureteronephrotic sac;hence heminephroureterectomy was performed through an incision on medioventral line.The left hydroureteronephrotic sac was dissected from surrounding tissues and the urinary bladder;its adhesion with the right middle segment ureter and communication with the posterior part of the prostatic urethra were identified.The sac was then resected completely,measured as 70-cm long and 24-cm wide,containing 10 L fluid.The tension-free repair for left inguinal hernia by prolene hernia system was performed at the same time.Combination of direct and indirect inguinal hernia was found during the surgery.Pathological evaluation of the tip of the resected sac indicated features of a dysplastic kidney.The wall of the sac consisted of muscle cells and transitional epithelium (Fig.2).

Figure 1.Preoperative image of the giant left hydroureteronephrosis and right hydronephrosis.
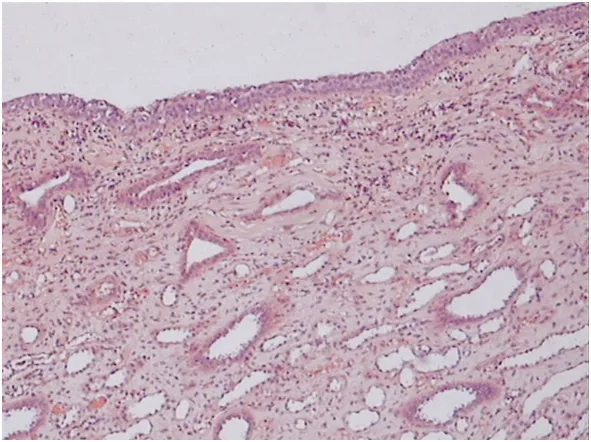
Figure 2.Histological findings show transitional epithelium on the upper side and primitive ducts on the lower side in the wall of the hydroureteronephrotic sac.HE ×40
The patient recovered from surgery without complications.During the follow-up period,serum creatinine levels were within the normal range with an average of 1.3 mg/dL(range,0.9-1.7 mg/dL).CT after 3-month follow-up showed considerable reduction of the right hydronephrosis(Fig.3).

Figure 3.Reformatted CT urogram at follow-up three months after operation shows mildly hydronephrotic right kidney and normal left kidney.
DISCUSSION
Giant hydroureteronephrosis caused by obstruction of the upper pole ureter in duplex kidney due to ectopic ureteral orifice into the prostatic urethra is a very rare urological entity.The ectopic ureter itself is abnormal.Usually,the ureter is variably dilated and drainage is impaired.An ectopic ureter may be severely obstructed,causing giant hydroureteronephrosis.It is a slowly progressive disease,and might present only with a huge abdominal mass or abdominal distension.3Adults with this condition may present with intermittent abdominal or flank pain,renal insufficiency,or urinary tract infection.4We were hence surprised that the only symptom of giant hydroureteronephrosis in this 32-year-old man was reducible lump at left groin.Similar cases have been recorded in the literature.Kaya et al5reported a rare case of giant hydroureteronephrosis in adult due to ureterovesical stricture presenting as a palpable abdominal mass.During surgery,approximately 7 liters of urine were drained.The patient in that case had a palpable abdominal mass 2 years before admission to the hospital.5We report here a rare case of giant hydroureteronephrosis associated with ipsilateral inguinal hernia and contralateral hydronephrosis presenting with only left inguinal hernia.The 32-year-old male patient underwent heminephroureterectomy and tensionfree inguinal hernia repair.
In differential diagnosis,multicystic dysplastic kidney,hydatid disease,giant hydroureteronephrosis associated with primary obstructed megaureter,giant hydroureteronephrosis due to calculi,and congenital giant hydroureteronephrosis may be considered.6In our case,the left giant hydroureteronephrosis increased intra-abdominal pressure and subsequently led to left inguinal hernia.The dilated ureter crossed the midline,adhering to the middle segment of right ureter and causing partial obstruction of the contralateral ureter.
Meticulous clinical and paraclinical examinations with imaging techniques,especially CT,could provide evidence for diagnosis and assist with determination of the optimal treatment.Since most ectopic ureters drain from upper pole that have minimal function,heminephroureterectomy is often recommended.3A two-stage procedure with gradual preoperative decompression is advocated to prevent possible cardiopulmonary collapse and alimentary tract dysfunction which might be caused by sudden decrease in intra-abdominal pressure.7In the present case,however,the recommended two-stage procedure is inadequate to resolve the problem of left inguinal hernia and therefore not adopted.Because of the nonfunctional left upper pole as confirmed in CT,we did not try to drain the left hydroureteronephrosis with a percutaneous nephrostomy prior to the operation.Throughout the surgical procedure,it is important to evaluate the body fluid status and blood volume because decreased intravascular volume might be encountered.To avoid this potential problem,the patient in this case received 1.5 L of 5% glucose in lactated Ringer’s irrigation preoperatively.Close monitoring during the operation is thought to be safe,which covers electrocardiogram,blood pressure,urine output,and central venous pressure.
1.Stirling WC.Massive hydronephrosis complicated by hydro-ureter.J Urol 1939;42∶520-33.
2.Chiang PH,Chen MT,Chou YH,et al.Giant hydronephrosis∶report of 4 cases with review of the literature.J Formos Med Assoc 1990;89∶811-7.
3.Schlussel RN,Retik AB.Ectopic ureter,ureterocele,and other anomalies of the ureter.In∶Wein AJ,editor.Campbell-Walsh urology.9th ed.Philadelphia∶Saunders Elsevier;2007.p.3383-422.
4.Hemal AK,Aron M,Wadhwa SN.Nephroplication and nephropexy as an adjunct to primary surgery in the management of giant hydronephrosis.Br J Urol 1998;81∶673-7.
5.Kaya C,Pirincci N,Karaman MI.A rare case of an adult giant hydroureteronephrosis due to ureterovesical stricture presenting as a palpable abdominal mass.Int Urol Nephrol 2005;37∶681-3.
6.Graff J,Funke PJ,Hertle L,et al.Giant hydroureteronephrosis.Case report and review of the literature.Urol Int 1986;41∶447-50.
7.Kogan BA.Disorders of the ureter &ureteropelvic junction.In∶Tanagho EA,McAninch JW,editors.Smith’s general urology.17th ed.New York∶McGraw-Hill;2007.p.348-70.
 Chinese Medical Sciences Journal2010年4期
Chinese Medical Sciences Journal2010年4期
- Chinese Medical Sciences Journal的其它文章
- Endothelial Nitric Oxide Synthase Gene Polymorphisms Associated with Susceptibility to High Altitude Pulmonary Edema in Chinese Railway Construction Workers at Qinghai-Tibet over 4 500 Meters above Sea Level△
- Thoraco-abdominal Aorta Revascularization through a Retroperitoneal Approach
- Clinicopathological Features of Non-familial Colorectal Cancer with High-frequency Microsatellite Instability△
- Epigenetic Repression of SATB1 by Polycomb Group Protein EZH2 in Epithelial Cells△
- NF-E2:a Novel Regulator of Alpha-hemoglobin Stabilizing Protein Gene Expression△
- Expression of Cyclooxygenase-2 and Its Relationship with Mismatch Repair and Microsatellite Instability in Hereditary Nonpolyposis Colorectal Cancer△